Desmoplastic fibroblastoma
Desmoplastic fibroblastoma
Clinical features Desmoplastic fibroblastoma (collagenous fibroma) is a distinctive, benign soft tissue tumor that mainly presents in a subcutaneous, fascial or intramuscular location.1–4 Presentation in the dermis is very rare and in one of the reported cases, the patient had a long-standing history of pemphigus.5–9 Lesions are asymptomatic and present as a slowly growing mass, most commonly located on the arm, shoulder, thigh, forearm, back and hands and feet.4 Size varies from 1 to 20 cm but the majority of tumors measure less than 4 cm.
Unusual tumors presenting on the neck mimicking a goiter, on the face mimicking a parotid tumor, in the oral cavity (including the tongue), in a lacrimal gland and within a joint have been documented.10–16 Most patients are middle-aged to elderly males but cases in younger patients and in children may rarely occur.4,17 A case with bone involvement has been described.18 The clinical behavior is entirely benign with no local recurrences reported in the literature to date.
and a prominent collagenous stroma.1–4 Tumor cells are elongated or stellate, with vesicular nuclei, a small nucleolus and pale cytoplasm. Mitotic figures are not seen. In some cases, there is focal myxoid change. Vascularity is not prominent and consists of small blood vessels with thin walls.
Pathogenesis and histologic features Cytogenetic studies in multiple cases have shown clonal abnormalities involving 11q12 which seems to be associated with deregulated expression of FOSL1.19–24 This locus is identical to that found in a single case of fibroma of tendon sheath.25 However, based on other studies, it is not likely that the entities are related (see fibroma of tendon sheath). One case with trisomy 8 has been reported.26
Tumors are fairly well circumscribed, round or oval and sometimes appear lobulated (Figs 35.102 and 35.103). Low-power examination reveals a lesion with very focal infiltration of surrounding tissues, poor cellularity
Immunohistochemistry shows diffuse positivity for vimentin, focal positivity for α-SMA and occasional positivity for keratin.4 In addition tumor cells are uniformly positive for FOSL1.27 There is negative staining for other markers including S100 protein, CD34 and desmin.
Ultrastructural studies suggest that the cells in the lesion are fibroblasts or myofibroblasts.7,28
Differential diagnosis The main differential diagnosis is fibromatosis. The latter tumor has an infiltrative growth pattern, is cellular, tumor cells have an elongated appearance and there is a prominent vascular network. An old lesion of nodular fasciitis is usually more hyalinized, with focal inflammation and degenerative changes. Fibroma of tendon sheath almost always occurs in acral sites and has a prominent lobular architecture with a conspicuous vascularity. Also, tumor cells are negative for FOSL1.27
1730 Connective tissue tumors
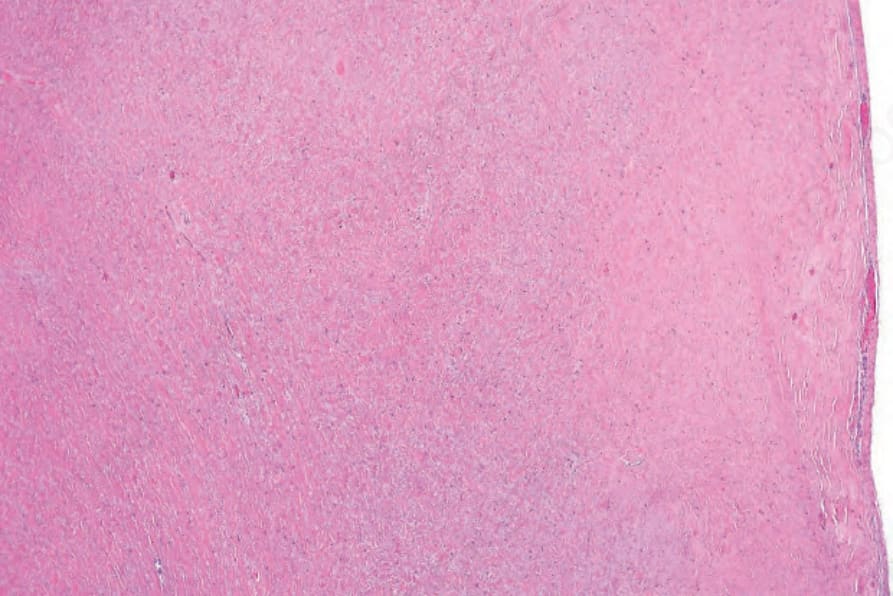
Fig. 35.102 Desmoplastic fibroblastoma: a low-power view showing a paucicellular tumor with abundant collagen.
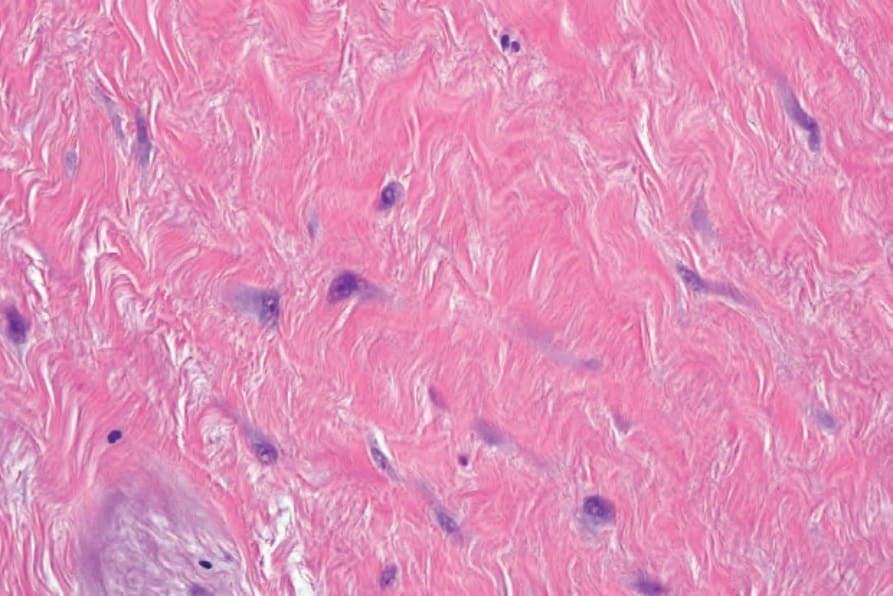
Fig. 35.103 Desmoplastic fibroblastoma: the tumor cells are fusiform or stellate. Mitotic figures are absent.
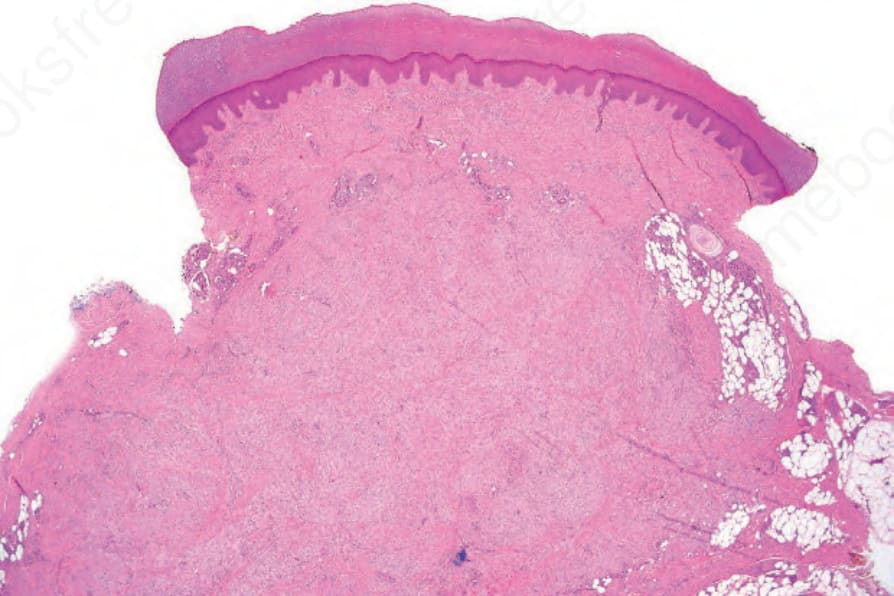
Fig. 35.104 Inclusion body fibromatosis: the tumor is composed of bland spindled cells with a collagenous stroma.
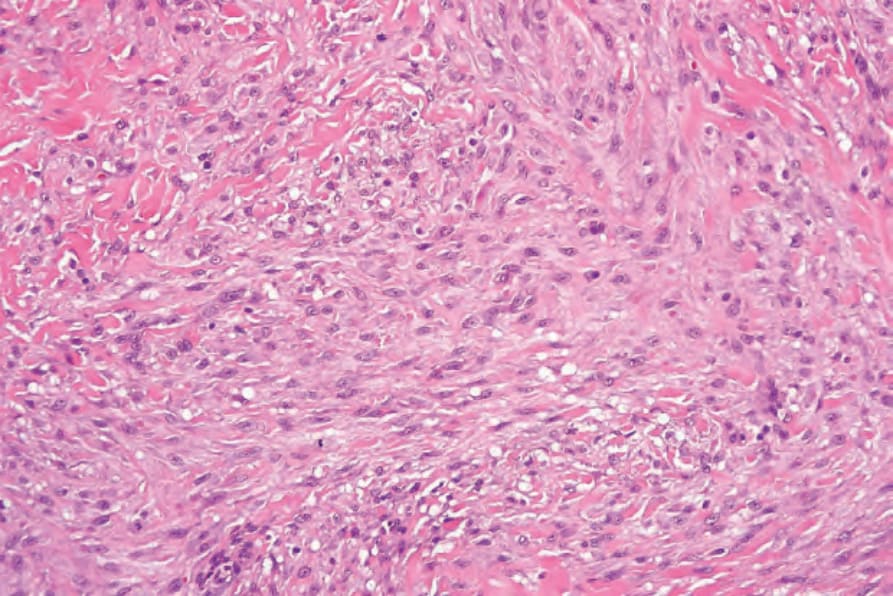
Fig. 35.105 Inclusion body fibromatosis: the spindled cells have uniform vesicular nuclei with small nucleoli.