Dermatomyofibroma
Dermatomyofibroma
Clinical features Dermatomyofibroma is a rare tumor that presents as a solitary, slowly growing, asymptomatic, skin-colored or hypopigmented plaque.1–6 It usually presents on the upper trunk or neck of young adults, with a predilection for
Histologic features Histology is distinctive and shows a plaque-like proliferation of fascicles of bland spindled cells with pale eosinophilic cytoplasm and elongated vesicular nuclei with one or two nucleoli (Figs 35.88–35.90). These fascicles tend to be parallel to the epidermis. The papillary dermis is usually spared and there is entrapment, but no destruction of adnexal structures by the tumor. Focal extension into the subcutaneous tissue is sometimes seen and occurs mainly along the septa in a perpendicular fashion. Rare cases display prominent hemorrhage.16 Myofibroblastic differentiation is suggested immunocytochemically by actin and calponin expression (Fig. 35.91). However, expression of actin and calponin is variable and may be focal or negative.6 CD34 may be focally positive.6 H-caldesmon and desmin are negative.
Electron microscopy shows cells with features of fibroblasts and myofibroblasts.17
1725 Benign fibrous and myofibroblastic tumors and tumorlike lesions
Differential diagnosis Dermatomyofibroma should be distinguished from plaque-stage dermatofibrosarcoma protuberans, in which the tumor cells are more basophilic and infiltrative. In addition, tumor cells in dermatofibrosarcoma protuberans are actin negative, and are usually diffusely positive for CD34. Dermatomyofibroma may also be confused with diffuse neurofibroma. The latter, however, is paler, lacks parallel orientation of tumor cells to the epidermis, and is S100 protein and CD34 positive. Rare hemorrhagic cases may be confused with nodular stage Kaposi sarcoma. However, in the latter condition, tumor cells are arranged in nodules, and are accompanied by numerous cleft-like spaces containing red blood cells. Inflammatory cells including plasma cells are always present, eosinophilic globules are prominent and all cases show nuclear reactivity with immunohistochemistry for human herpesvirus.16
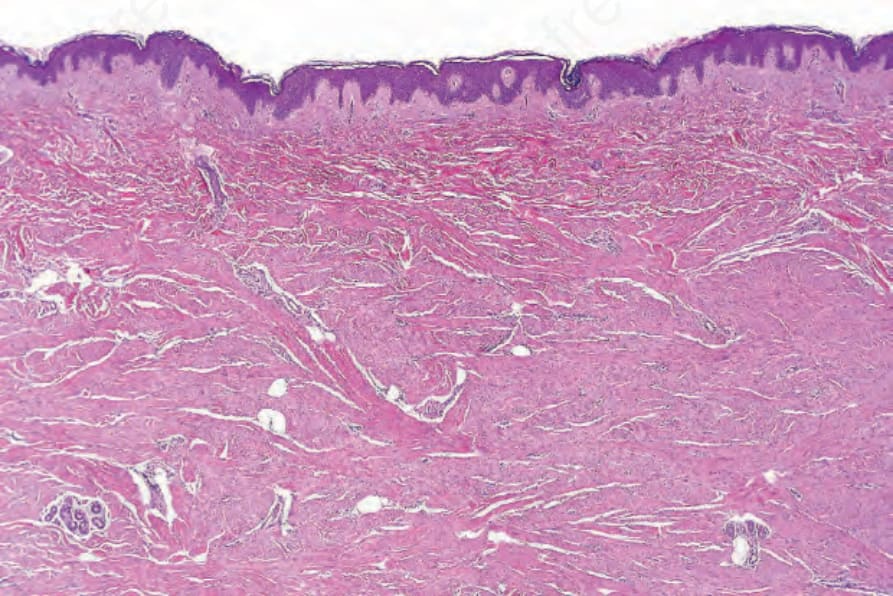
Fig. 35.88 Dermatomyofibroma: low-power view showing fascicles of spindled cells orientated parallel to the surface epithelium.
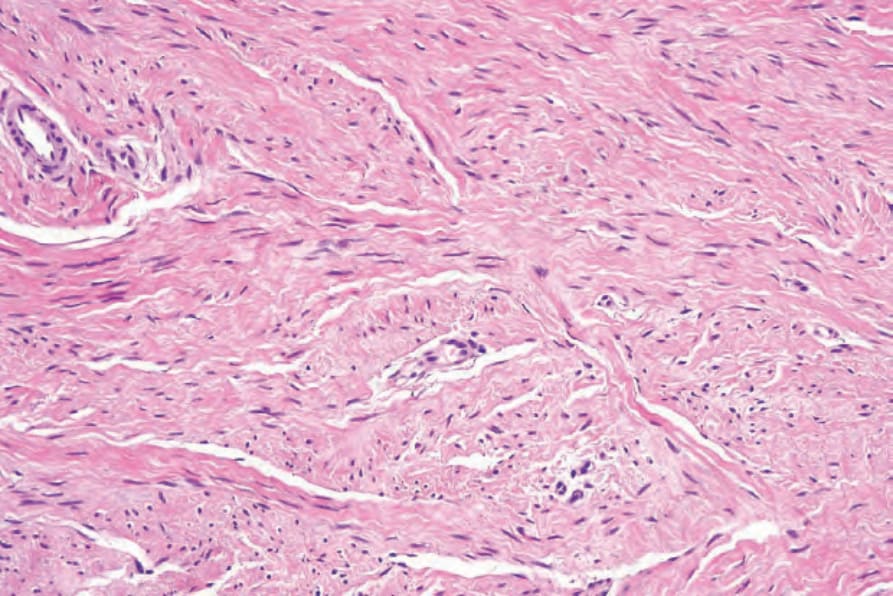
Fig. 35.89 Dermatomyofibroma: the fascicles grow between the dermal collagen bundles.
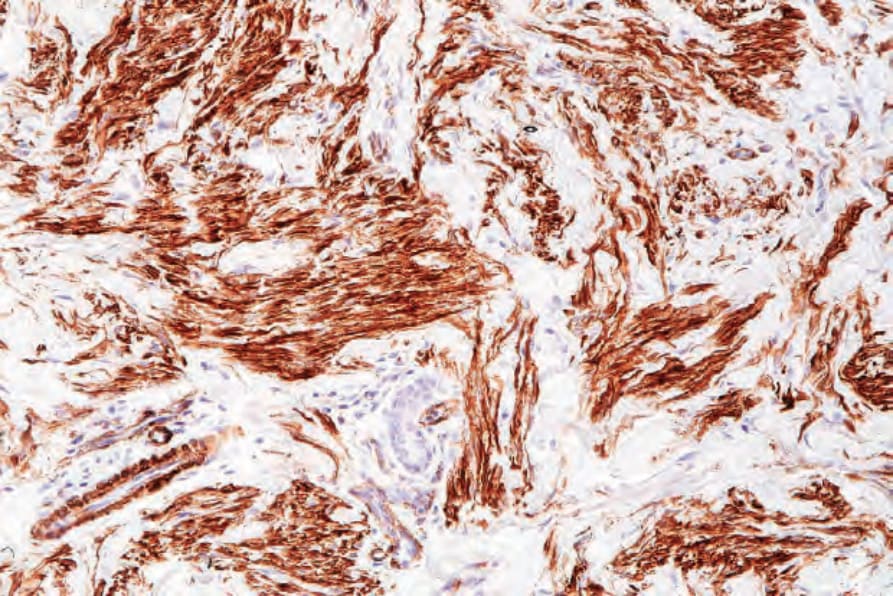
Fig. 35.91 Dermatomyofibroma: the tumor cells express smooth muscle actin.