Fibroepithelial polyp (including pleomorphic fibroma)
Fibroepithelial polyp (including pleomorphic fibroma)
Clinical features Fibroepithelial polyps (acrochordon, skin tag, soft fibroma) are very common lesions that typically present in adults, especially obese females, with a predilection for the neck, axillae and groin.1,2 Perianal lesions are also frequently encountered. Rare lesions have been documented in the umbilicus.3
Pleomorphic fibroma refers to a small proportion of cases of acrochordons that show cells with bizarre hyperchromatic and pleomorphic nuclei (Figs 35.86 and 35.87).18 Multinucleation is also a feature, but mitotic figures are very few and never atypical. These cells are actin positive and the changes are likely to be the result of degeneration, as seen in other tumors such as pleomorphic lipoma and ancient schwannoma. Similar lesions have been described under the name cutaneous pseudosarcomatous polyp.19,20 Changes similar to pleomorphic fibroma may also be seen in ‘regressed’ or hyalinized examples of solitary myofibroma or dermatomyofibroma.
By immunohistochemistry, cells may be positive for CD34.21
Differential diagnosis Pleomorphic fibroma can be distinguished from a dermal atypical lipomatous tumor by the absence of an adipocytic component including lipoblasts in the former. MDM2 immunohistochemistry and MDM2 gene amplification is not seen in pleomorphic fibroma.22 In a single case report however,
1724 Connective tissue tumors
females. Most lesions are less than 4 cm in diameter. Tumors may resemble a plaque lesion of dermatofibrosarcoma protuberans or a keloid. An exceptional case presenting in a linear distribution, one with an annular configuration have been documented.7,8 Rare cases occur in children and have predilection for the neck.9–14 Multiple tumors are very rare.15 Local recurrence is exceptional.
MDM2 immunohistochemistry was positive in a pleomorphic fibroma but this was not associated with MDM2 gene amplification.23 Recently, uniform genetic loss of RB1 (13q) has been documented in pleomorphic fibroma as well as recurrent losses in 10q, 16q, and 17p.24 Loss of nuclear RB1 can also be demonstrated by immunohistochemistry.24 This strongly suggests a genetic relationship to spindle cell and pleomorphic lipomas as well as cellular angiofibromas and mammary-type myofibroblastomas—all of which are known to harbor RB1 loss.
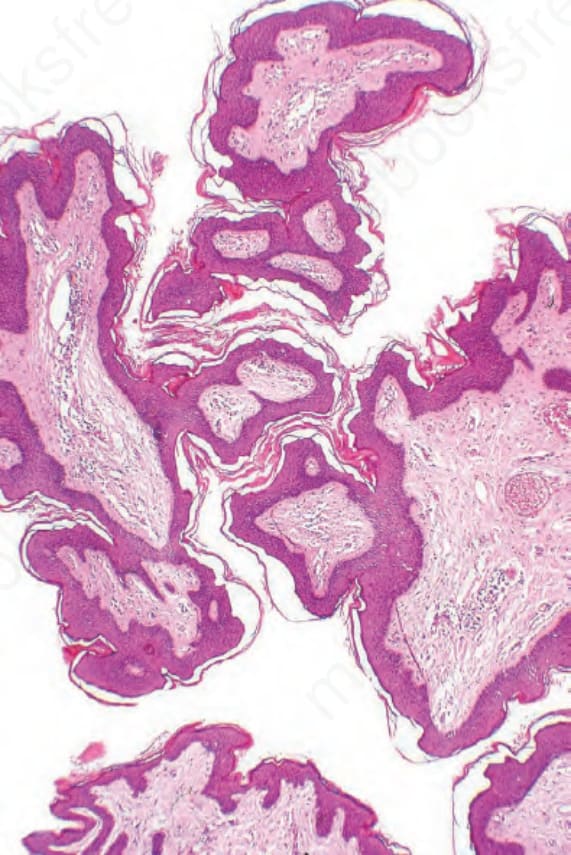
Fig. 35.84 Acrochordon: histologically, it consists of connective tissue covered by squamous epithelium.
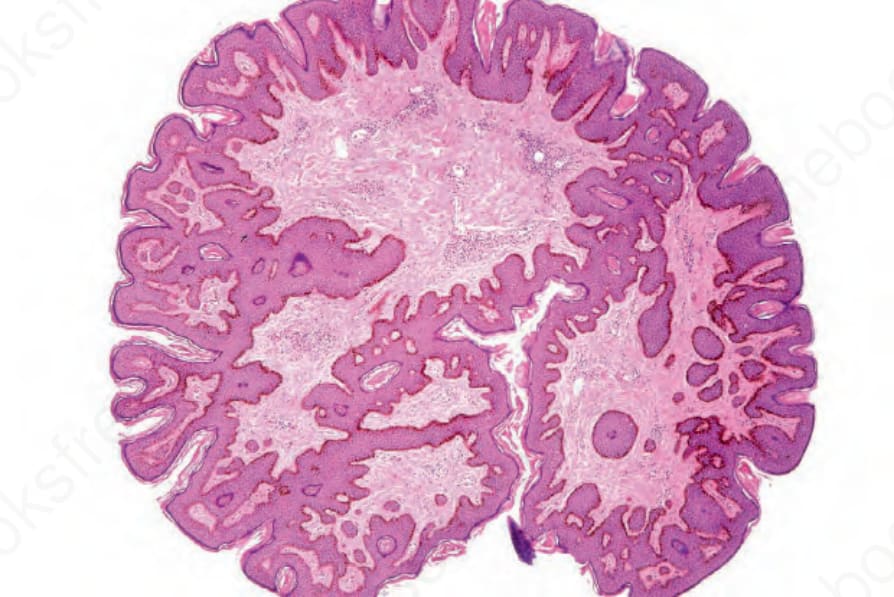
Fig. 35.85 Acrochordon: this unusually sectioned example shows the features to advantage.
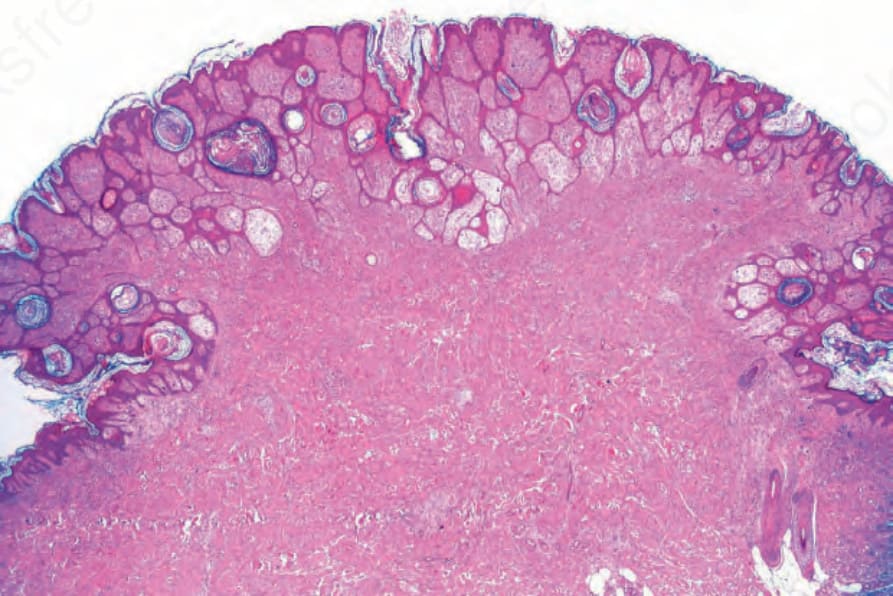
Fig. 35.86 Pleomorphic fibroma: this lesion is characterized by the presence of scattered mononuclear and multinucleated giant cells.
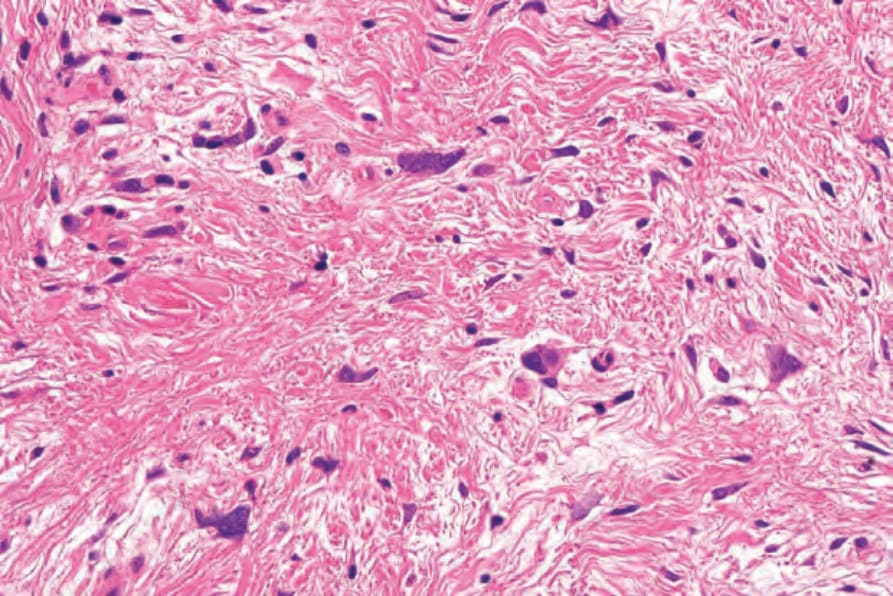
Fig. 35.87 Pleomorphic fibroma: note the fusiform and stellate cells with hyperchromatic irregular nuclei.