Elastofibroma
Elastofibroma
Clinical features Elastofibroma is an uncommon, deep-seated pseudotumor that is thought to represent a degenerative and reactive change in elastic fibrous tissue.1–5 It almost always arises in the infrascapular region, most often in the elderly, and is usually unilateral. There is only one report of a lesion developing in early life.6 Rare cases have been reported in the hip, hand, olecranon, upper arm, eye and oral cavity.7–9 Elastofibromatous changes are present in a number of samples obtained from patients operated for spinal canal compression.10 Infrequently, lesions are bilateral and multiple;11–13 Often, the second lesion is subclinical and can only be detected radiologically.14 A visceral location is very rare but includes the trachea and gastrointestinal tract.15 Females are predominantly affected and, although tumor size varies, fixation to the periosteum of the underlying ribs is invariable. Familial presentation has been described in up to 30% of cases.5,16 Tumors are usually asymptomatic and may reach a large size. Simple excision is the treatment of choice but asymptomatic lesions do not necessarily need to be removed.17,18 Recurrence is extremely uncommon.
Pathogenesis and histologic features It is a commonly held belief that elastofibroma arises as a consequence of chronic frictional trauma between the scapula and underlying connective tissues, but a relationship with heavy manual labor is unsubstantiated. The theory that the process is a result of degeneration is given support by the finding of changes similar to those of elastofibroma in tissue taken in autopsies of elderly patients with no discernible mass.19,20
Cytogenetic studies have shown clonal and nonclonal structural changes, particularly aberrations of the short arm of chromosome 1.21–24
Elastofibroma is typically an ill-defined unencapsulated mass merging with adjacent connective tissue and composed of fairly acellular collagenous and adipose tissue containing numerous elastic fibers (Figs 35.80 and 35.81). These fibers, ideally demonstrated by an appropriate histochemical
1723 Benign fibrous and myofibroblastic tumors and tumorlike lesions
These polyps are often multiple and can be associated with pregnancy. Contrary to what was proposed in the past, they do not appear to be a marker for colonic polyps.4,5 An association with diabetes mellitus has been suggested.6,7 Lesions are usually less than 1 cm in diameter and can be papular, filiform or pedunculated (Fig. 35.83). Rarely, tumors such as squamous cell carcinoma, keratoacanthoma and basal cell carcinoma may develop within a fibroepithelial polyp.8–11 Lymphedematous fibroepithelial polyps have been documented in the glans penis and prepuce as a result of chronic condom and catheter use.12 It has been suggested that fibroepithelial polyps should not be submitted for histologic examination since malignant tumors only very exceptionally show similar clinical features.13 This is, however, controversial and, in our view, all should be carefully evaluated. Melanoma, for example, may very rarely grossly mimic a fibroepithelial polyp. Fibroepithelial polyps in children are very rare and their occurrence has been reported as a presenting sign of the nevoid basal cell carcinoma syndrome.14 Lesions identical to fibroepithelial polyps have been described in the tongue of immunosuppressed patients and may also occur in the skin.15,16 In these patients, the polypoid lesions show features of basal cell carcinoma. Fibroepithelial polyps can be associated with the rare Birt-Hogg- Dubé syndrome.
stain, tend to be coarse, thick or globular, and are sometimes distributed as irregular masses (Fig. 35.82). It has been shown that the fibers represent true elastin and not elastotic collagen.25,26 Amyloid deposition has been reported in one case.27 The cells in the background tend to be positive for CD34 but negative for myofibroblastic markers.28
Histologic features Fibroepithelial polyps show a normal or hyperplastic epidermis surrounding a core of fibrovascular tissue with loose or dense collagen fibers (Figs 35.84 and 35.85). Fat cells can be present and, if abundant, the lesion shows overlap with nevus lipomatosus superficialis. Focal pagetoid dyskeratosis may be an incidental finding in keratinocytes.17
Differential diagnosis Identification of the distinctive changes in the elastic fibers allows for easy recognition of the condition. Nuchal fibroma is distinguished from elastofibroma by the absence of altered elastic fibers and the presence of fairly thick collagen bundles in the former condition.
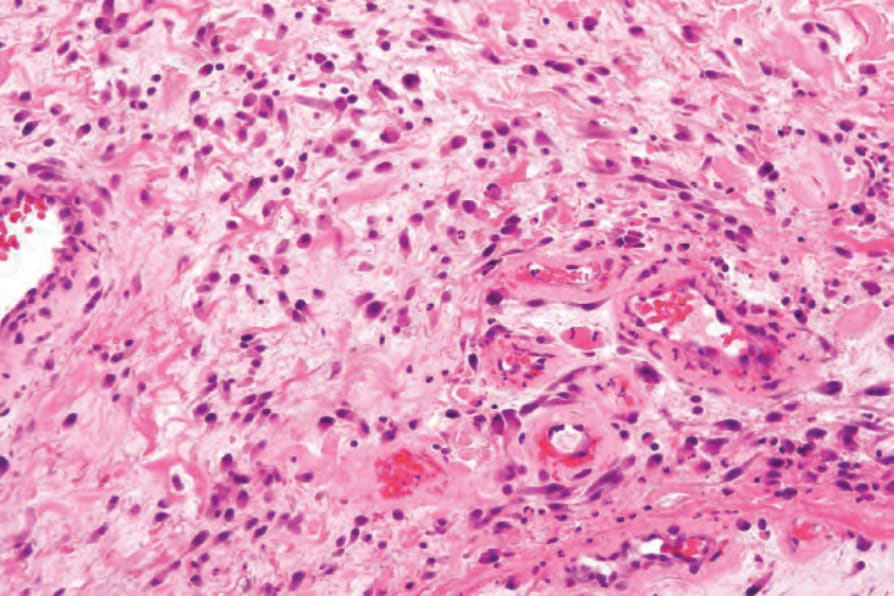
Fig. 35.78 Ischemic fasciitis: this field shows an atypical cellular population.
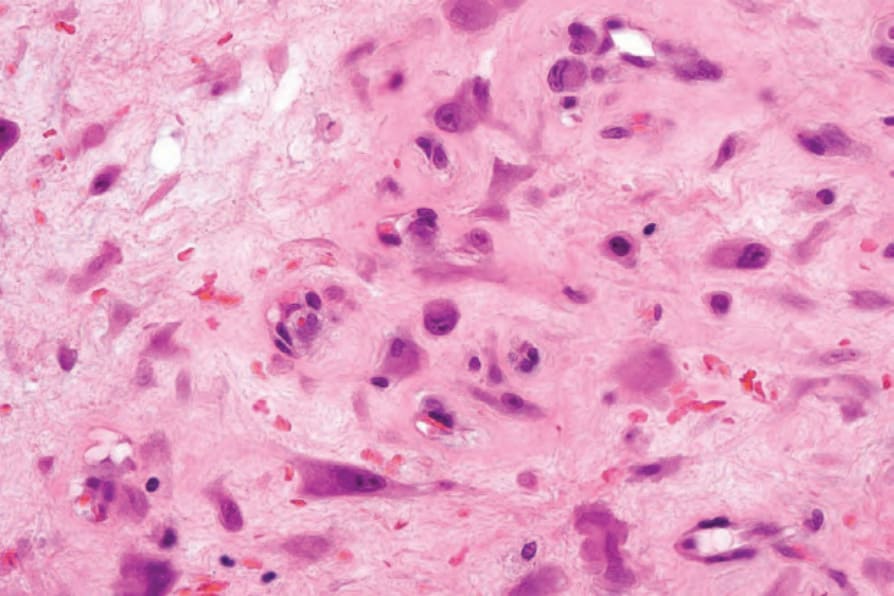
Fig. 35.79 Ischemic fasciitis: there are atypical spindled cells and histiocyte-like cells, some with a ganglion-like appearance.
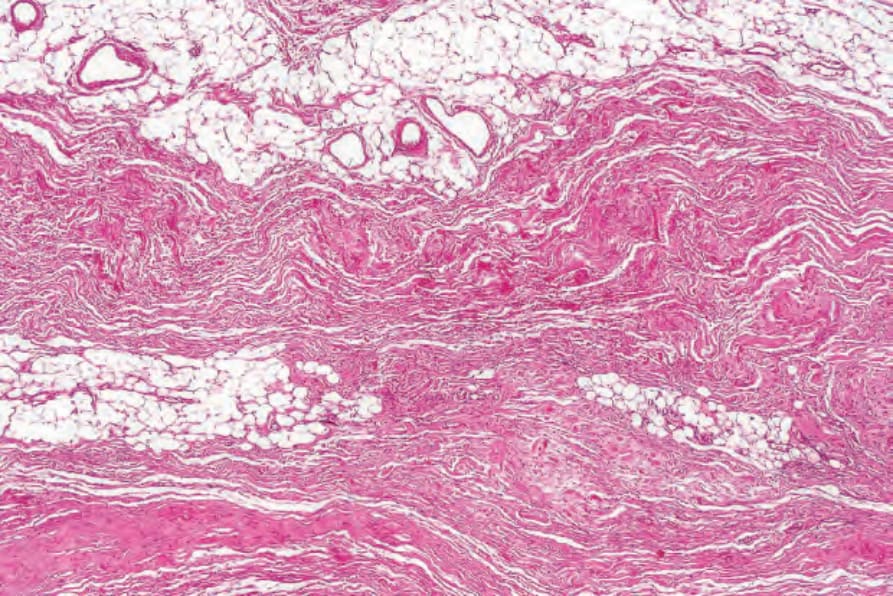
Fig. 35.80 Elastofibroma: there is an admixture of collagen bundles and thickened, irregular, eosinophilic elastic fibers.
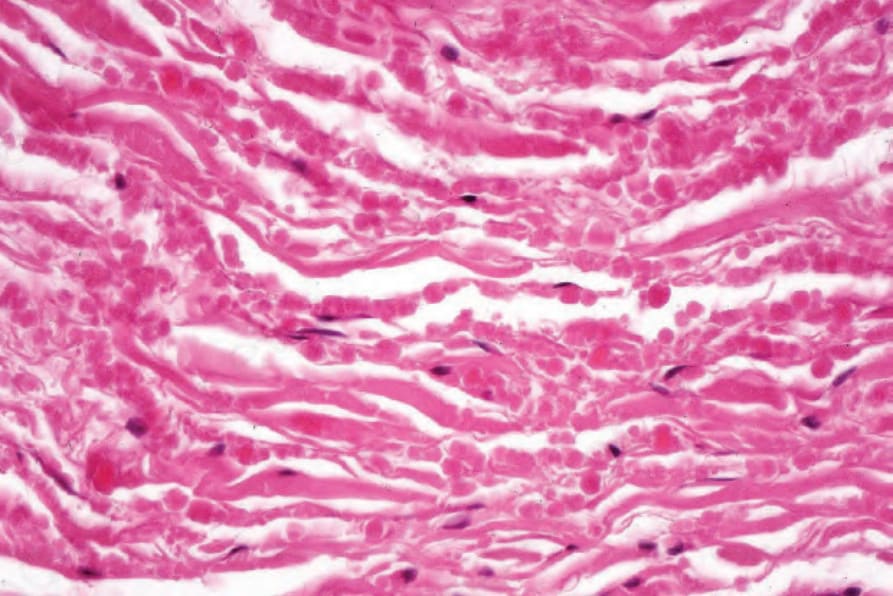
Fig. 35.81 Elastofibroma: the elastic fibers are fragmented and appear beaded.
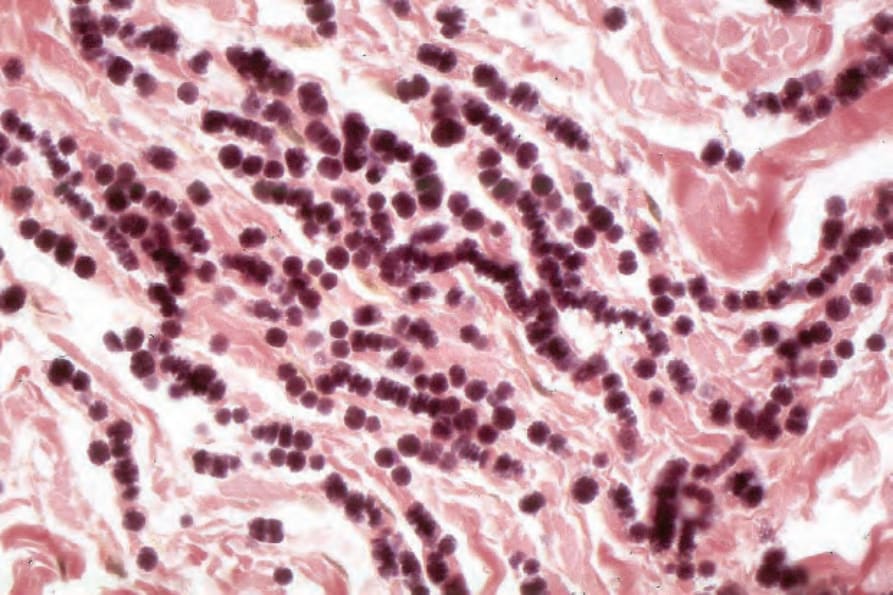
Fig. 35.82 Elastofibroma: the serrated edge so characteristic of this condition is seen in this elastic–van Gieson stained section.

Fig. 35.83 Acrochordon: also known as a skin tag or fibroepithelial polyp, this soft polyp is exceedingly common. By courtesy of the Institute of Dermatology, London, UK.
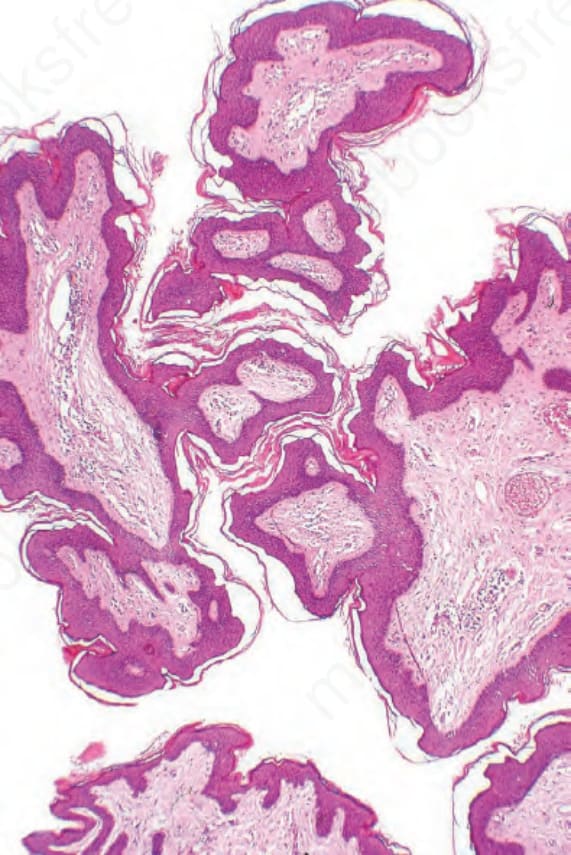
Fig. 35.84 Acrochordon: histologically, it consists of connective tissue covered by squamous epithelium.