Ischemic fasciitis
Ischemic fasciitis
The spindle-shaped proliferating cells are positive for actins (SMA and MSA) but negative for desmin, whereas the ganglion-like cells may be negative for actins and are negative for neural and epithelial markers.
Electron microscopy studies indicate that these cells have features of fibroblasts.15,16 The flow cytometry profile of these lesions is diploid.17
Differential diagnosis Distinction from a sarcoma may be difficult in small lesions, especially if close clinicopathological correlation is lacking. Most sarcomas have a larger size and although a ‘checkerboard’ appearance may be present in sarcomas or metastatic carcinomas, this is usually only focal and there is more tendency towards destruction of the surrounding muscle. A desmoid tumor lacks ganglion-like cells and usually replaces the muscle completely.
Clinical features Ischemic fasciitis (also known as atypical decubital fibroplasia) is a relatively rare pseudosarcomatous fibroblastic/myofibroblastic condition that occurs over bony prominences.1–3 The great majority of patients are elderly (between the sixth and ninth decades of life) and immobilized. However, cases in ambulatory and even in young patients have been described.4–7 Lesions consist of an asymptomatic, subcutaneous, ill-defined mass only occasionally associated with ulceration. The majority of lesions arise in the deep subcutaneous tissue but involvement of the dermis and deeper soft tissues including skeletal muscle and tendons may also be seen.4 Exclusive involvement of skeletal muscle is very rare.4 Most tumors are less than 4 cm in diameter but larger lesions also occur. The usual sites are the shoulders, thighs, buttocks, sacral area and chest wall. Local excision is generally curative and recurrences are only seen in patients where the predisposing factor persists. A case of ischemic fasciitis associated with bizarre parosteal osteochondromatous proliferation has been documented.8
1721 Benign fibrous and myofibroblastic tumors and tumorlike lesions
Pathogenesis and histologic features
The proliferation is thought to be due to ischemia induced by pressure resulting from prolonged immobilization. However, a recent study has not consistently found immobility or debilitation.4 Some cases are triggered by trauma.4
Histologically, lesions are multilobular and characterized by replacement of the subcutaneous tissue by areas of fibrinoid necrosis and granulation tissue (Figs 35.77 and 35.78). Myxoid change, hemorrhage and edema are usually prominent. In the areas of necrosis there is marked fibrinoid change and ghosts of necrotic adipocytes are seen. At the periphery there is vascular proliferation accompanied by variable numbers of spindle-shaped and more round cells with irregular hyperchromatic nuclei and a single prominent basophilic nucleolus. Ganglion-like cells similar to those present in proliferative fasciitis are also found and in these the nuclei contain smudged chromatin (Fig. 35.79). Mitotic figures may be found but atypical forms are generally not seen. Thrombosis of blood vessels is also a feature.
Immunohistochemistry shows that the cells in the proliferation are variably positive for smooth muscle actin (SMA), calponin and desmin.4 In rare cases positivity for MDM2, CDK4 and p16 can be seen.5
1722 Connective tissue tumors
Differential diagnosis As already discussed, this lesion closely resembles proliferative fasciitis and many regard it as a variant of nodular fasciitis. However, the MYH9-USP6 fusion characteristic of nodular fasciitis has not been documented in this condition. Distinction between ischemic fasciitis and a sarcoma is based on the relatively low mitotic count, the absence of atypical mitotic figures, and the low cellularity in the former lesion.

Fig. 35.73 Fibro-osseous pseudotumor of the digits: this lesion presented as a rapidly growing nodule. Note the prominent calcification. By courtesy of the Institute of Dermatology, London, UK.
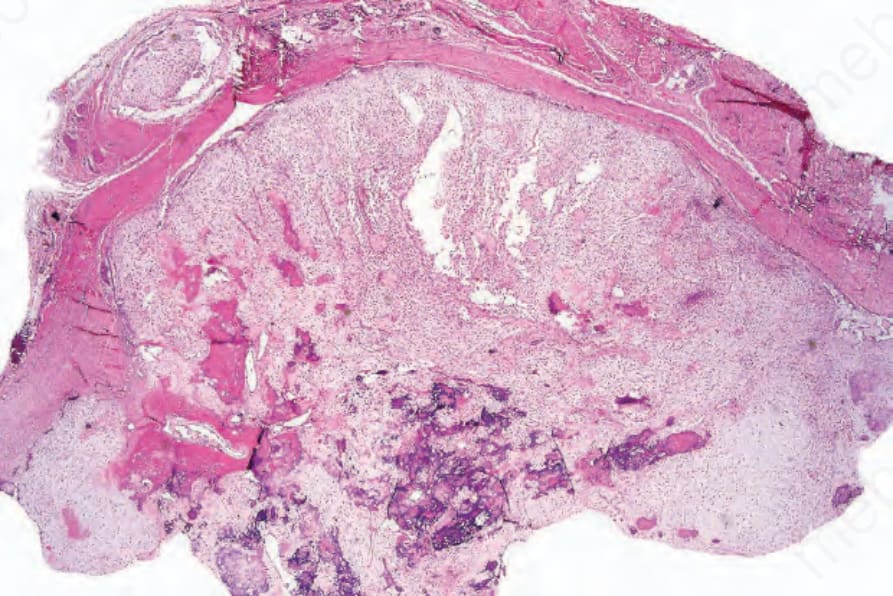
Fig. 35.74 Fibro-osseous pseudotumor of the digits: scanning view showing osteoid, foci of calcification and a myxoid spindle cell tumor.
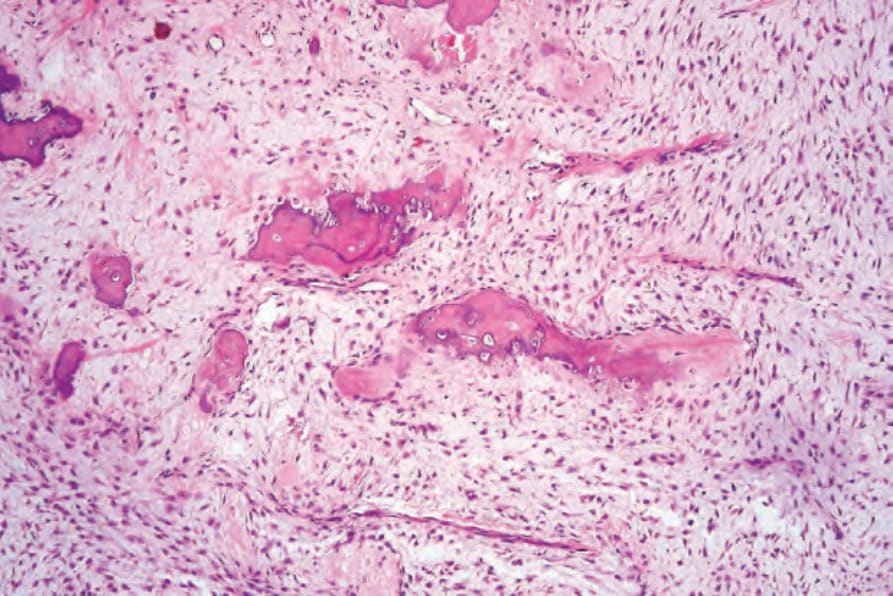
Fig. 35.75 Fibro-osseous pseudotumor of the digits: medium-power view showing calcified osteoid and spindled cells within a myxoid matrix.
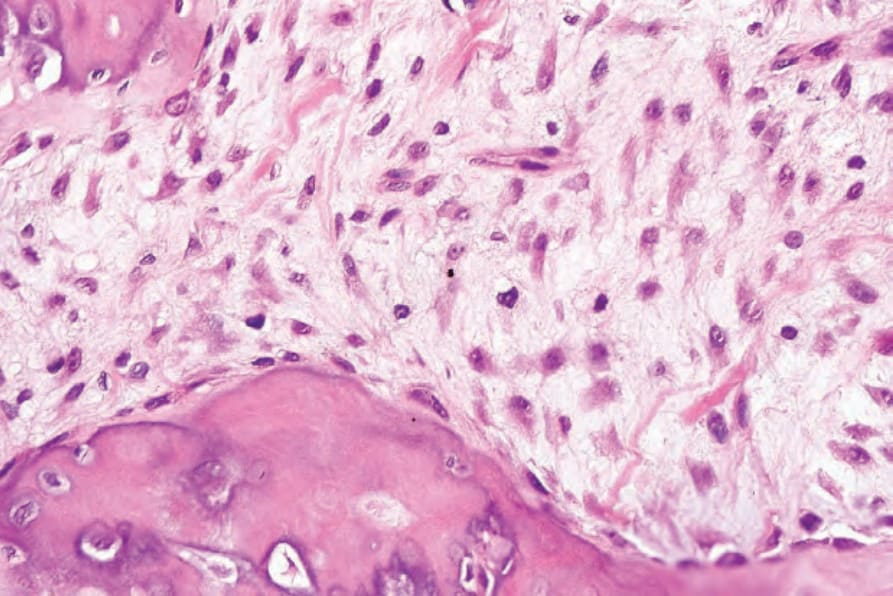
Fig. 35.76 Fibro-osseous pseudotumor of the digits: high-power view of tumor myofibroblasts.
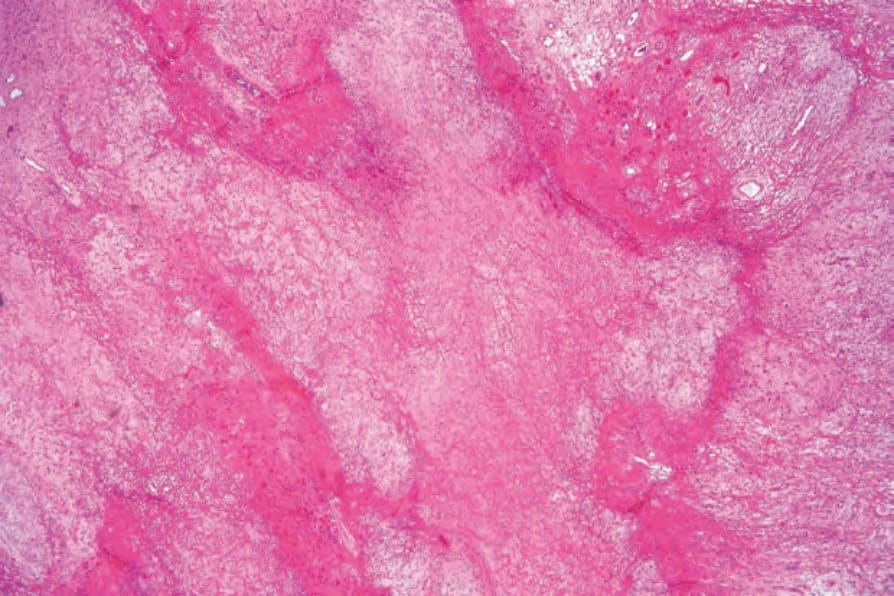
Fig. 35.77 Ischemic fasciitis: scanning view showing massive fibrin deposition with adjacent granulation tissue.
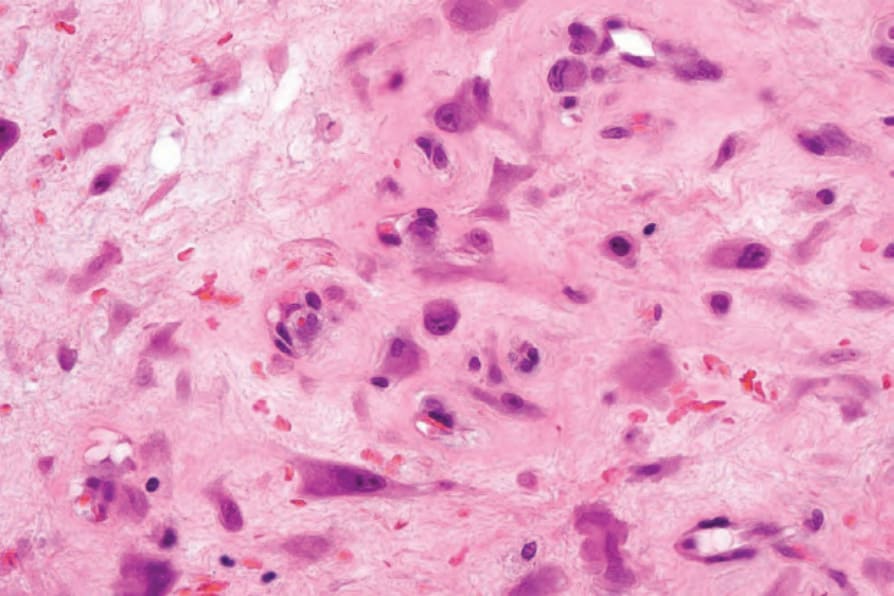
Fig. 35.79 Ischemic fasciitis: there are atypical spindled cells and histiocyte-like cells, some with a ganglion-like appearance.