Nodular fasciitis
Nodular fasciitis
Clinical features Nodular fasciitis is uncommon and represents a florid proliferative reactive process of unknown etiology.1–8 It is most often seen in young or middle-aged adults of either sex, particularly on the limbs (especially the forearms) or trunk. Cases in children including newborns are rare and tend to favor the head and neck area (including the external auditory canal and oral cavity).8–12 The lesion presents as a rapidly growing, subcutaneous nodule rarely exceeding 4–5 cm in diameter, and is typically painful or tender. Purely intramuscular lesions may rarely occur. The tumor develops with such speed that most patients present within 3 months of first becoming aware of a mass. Local recurrence may be a feature, but is sufficiently infrequent that its occurrence should raise the possibility of misdiagnosis. Recurrence seems to be more common in lesions of the head and neck mainly in
1717 Benign fibrous and myofibroblastic tumors and tumorlike lesions
children and in lesions presenting in the auricle.13 Spontaneous regression may occur.14 Intraneural and intra-articular lesions are very rare.15–17 A case of nodular fasciitis developing at the margin of a second stage Mohs excision of a dermatofibrosarcoma protuberans has been described.18 A case associated with etanercept therapy for psoriasis is probably coincidental.19
An exceptional case of nodular fasciitis with malignant behavior including multiple recurrences and metastatic spread and associated with PPP6R3-USP6 amplification has been described.20
Pathogenesis and histologic features Initial studies of nodular fasciitis showed evidence of clonality, suggesting that the lesion is neoplastic.21,22 Identification of an MYH9-USP6 gene fusion has firmly established its neoplastic nature, and the tumor has been regarded as an example of transient neoplasm.23–25 That is, the tumor has self-limiting growth followed by regression. Several additional novel fusion partners have been identified that use the promoters of genes other than MYH9 to drive USP6 overexpression.24
Nodular fasciitis is typified by a relatively well-circumscribed but unencapsulated mass composed of plump spindled cells set in a loose myxoid and collagenous stroma with a typically feathery, microcystic appearance (Figs 35.57–35.60). Numerous thin-walled blood vessels, often lined by rather prominent endothelial cells, ramify through the lesion, usually in a radial arrangement. Foci of hemorrhage and a sparse chronic inflammatory infiltrate composed largely of lymphocytes are usually present, and occasional cases contain foamy histiocytes and multinucleate osteoclast-type giant cells. The plump spindled cells (Figs 35.61–35.63) are mitotically active, but the mitoses are never atypical. The degree of cellularity and relative amounts of collagenous tissue and loose edematous stroma vary between lesions, probably reflecting the duration of the process. Extension into skeletal muscle is rare and mainly seen in lesions of the head and neck.11
Immunohistochemistry shows diffuse and strong positivity for smooth muscle actin and usually also calponin, but desmin and h-caldesmon are usually negative, in keeping with myofibroblastic differentiation (Fig. 35.64).26
Ultrastructurally, the tumor cells have abundant rough endoplasmic reticulum and contain aggregates of filaments with dense bodies deep to the plasma membrane (Fig. 35.65).
1718 Connective tissue tumors
Variants
• Intradermal fasciitis refers to a very rare variant of fasciitis that primarily arises in the dermis with only focal extension into the subcutaneous tissue.27–32 A polypoid architecture is exceptional.33 Lesions on the ear may rarely extend into the underlying cartilage.25 Histologic features are identical to those of the classic variant (Figs 35.66–35.68) and tumors display the same molecular abnormality as that seen in the soft tissue counterparts.24,25,32
• Fasciitis ossificans describes the small proportion of cases of nodular fasciitis that show metaplastic formation of osteoid, mature bone or even cartilage.5,34 A zoning pattern of maturation, as seen in myositis ossificans, is usually absent. In some cases, osteoid formation is only focal and calcification may be absent. Fibro-osseous pseudotumor of the digits is described below.
• Periosteal fasciitis arises from the periosteum and most often presents on the head of children (usually under the age of 2 years and with predilection for males). It is then known as cranial fasciitis when there is significant erosion of bone.35,36 While histologically related to nodular fasciitis, it is not clear that this entity harbors the same fusion gene in the authors’ experience.
• Proliferative fasciitis is described below.
1719 Benign fibrous and myofibroblastic tumors and tumorlike lesions
• Intravascular fasciitis is a very rare lesion seen most often in young adults. Intraoral cases have been described.37 Although histologically very similar to typical nodular fasciitis, it involves the full thickness and lumen of a peripheral blood vessel (usually a vein), and therefore simulates vascular invasion.7,37–39 To avoid a diagnosis of malignancy, careful attention should be paid to the bland histologic features. Ultrastructural studies show cells with features of fibroblasts and myofibroblasts.
Differential diagnosis Features that should raise the possibility of malignancy in diagnostically difficult lesions include abnormal mitotic figures, nuclear hyperchromasia or pleomorphism and necrosis. The dermal variant of nodular fasciitis can be distinguished from benign fibrous histiocytoma because the latter is more polymorphic and actin tends to be only focally positive or negative.
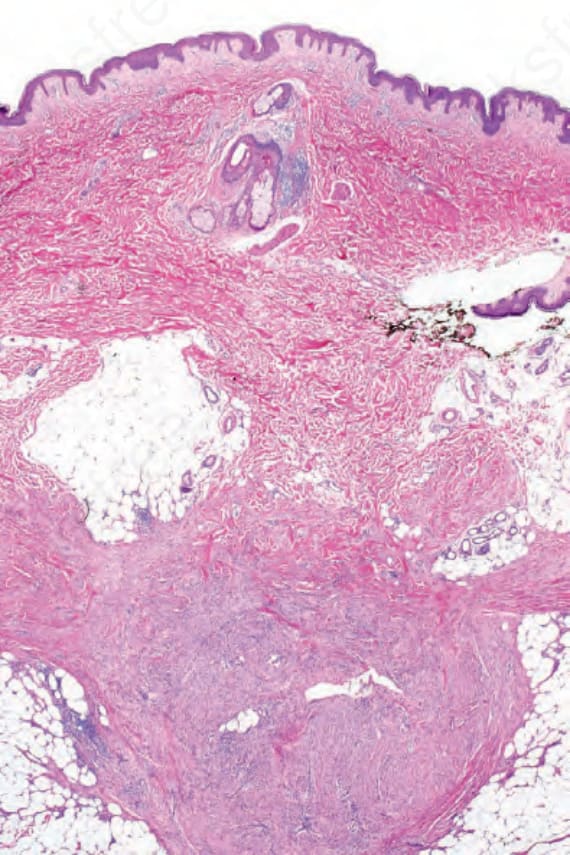
Fig. 35.57 Nodular fasciitis: lowpower view showing a well-circumscribed example.
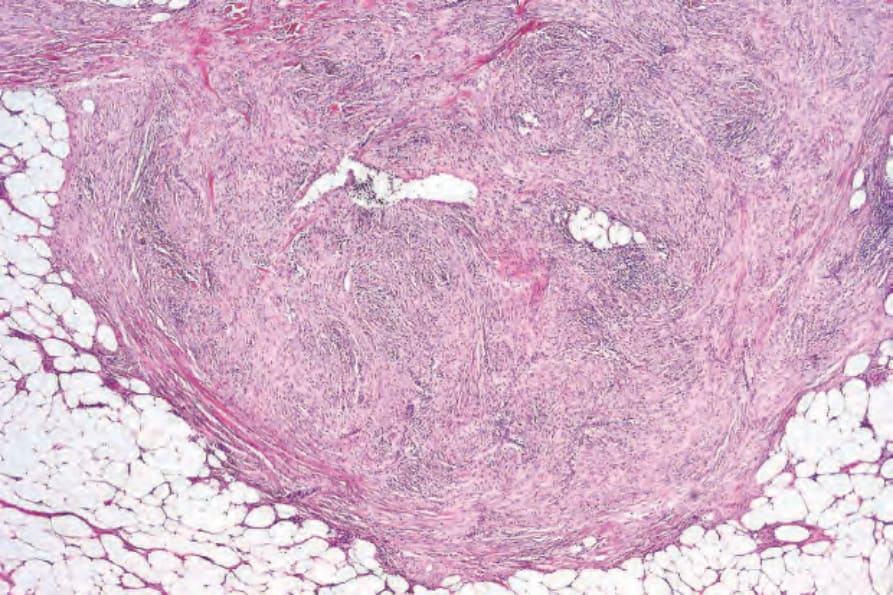
Fig. 35.58 Nodular fasciitis: this view highlights the circumscription.
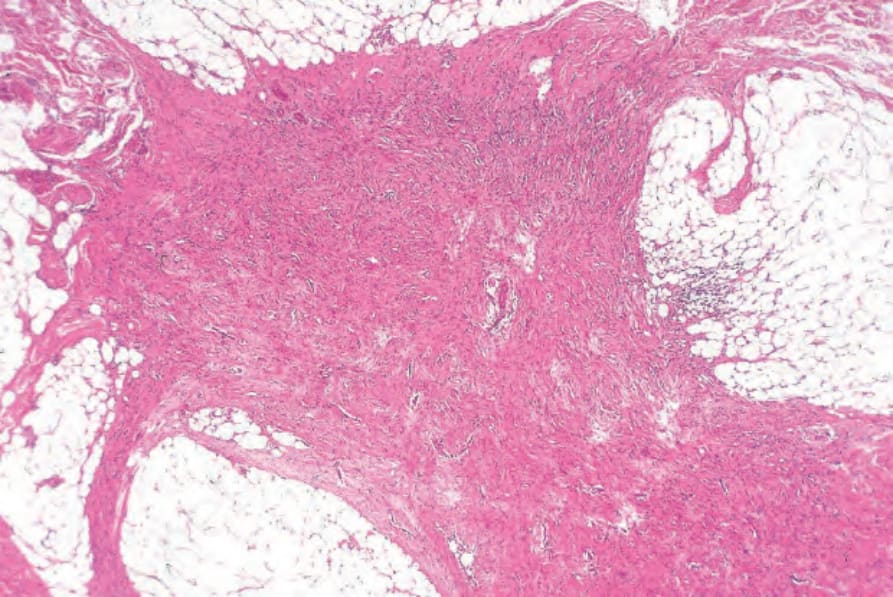
Fig. 35.59 Nodular fasciitis: in this lesion, there is a much more irregular border.
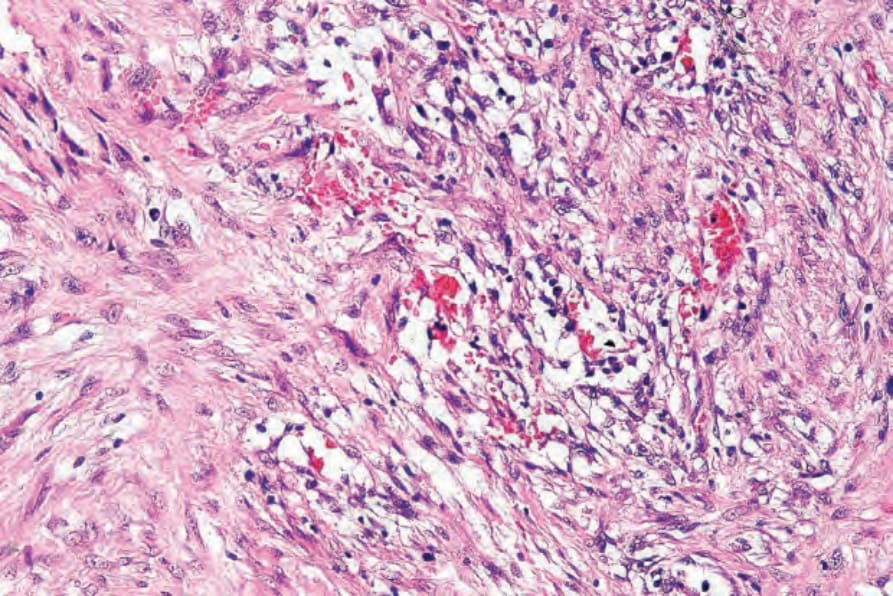
Fig. 35.60 Nodular fasciitis: the stroma is characteristically myxoid, which results in this feathery appearance.
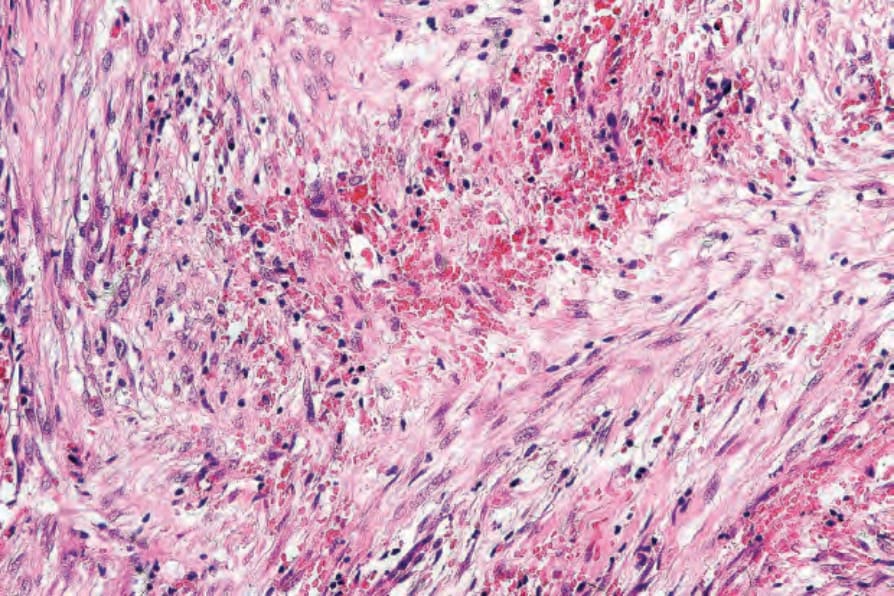
Fig. 35.61 Nodular fasciitis: foci of hemorrhage are commonly present.
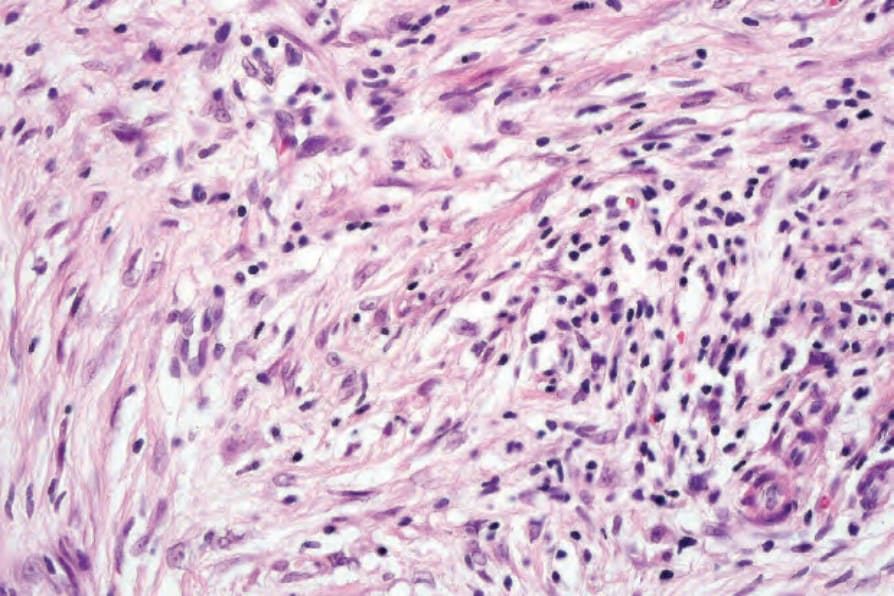
Fig. 35.62 Nodular fasciitis: small numbers of lymphocytes are usually evident.
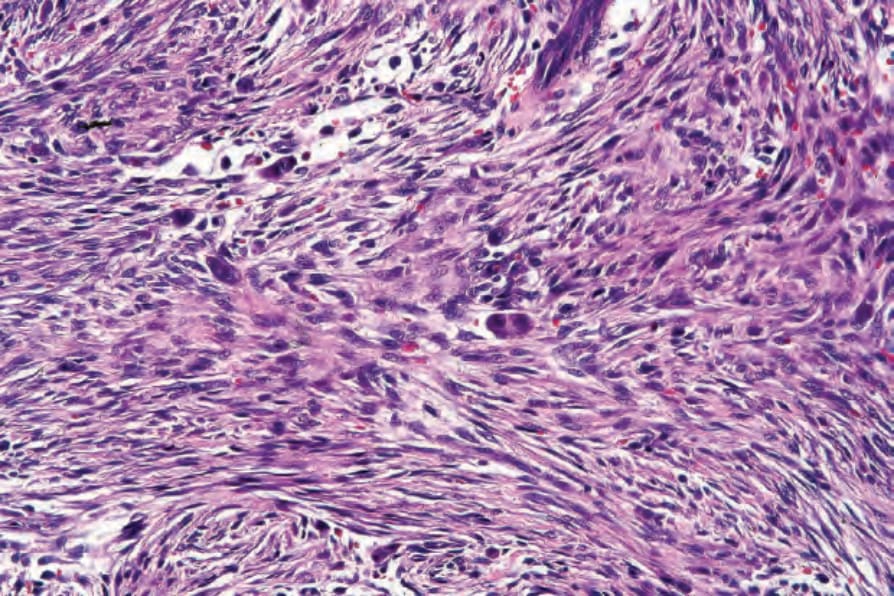
Fig. 35.63 Nodular fasciitis: in this example multiple giant cells are seen.
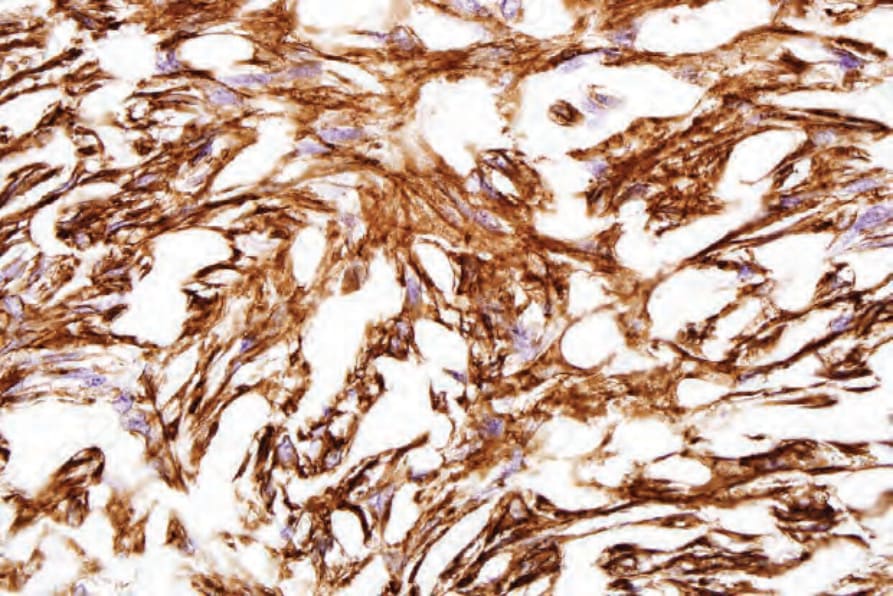
Fig. 35.64 Nodular fasciitis: the spindled cells show strong SMA expression.
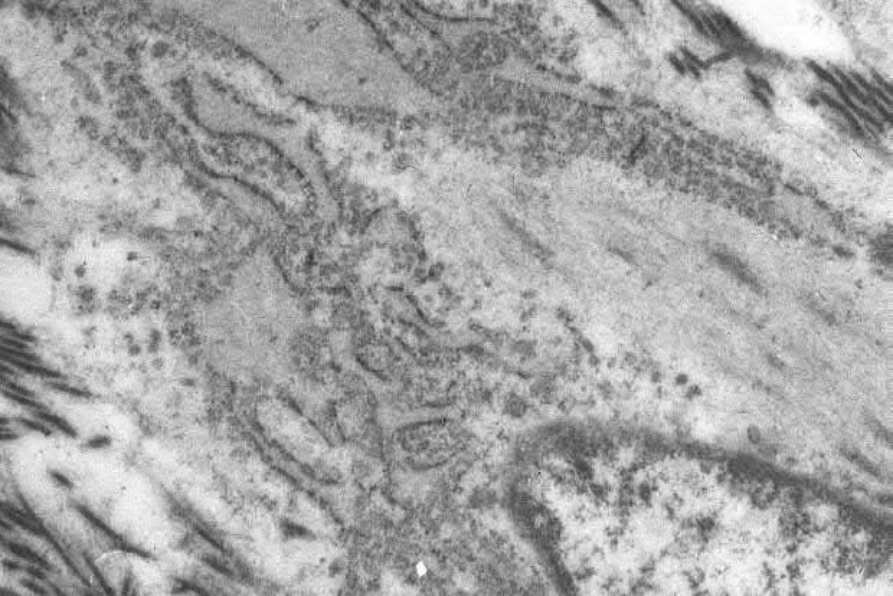
Fig. 35.65 Nodular fasciitis: ultrastructurally, the spindled cells show features of myofibroblasts. Note the conspicuous rough endoplasmic reticulum and filaments with dense bodies.
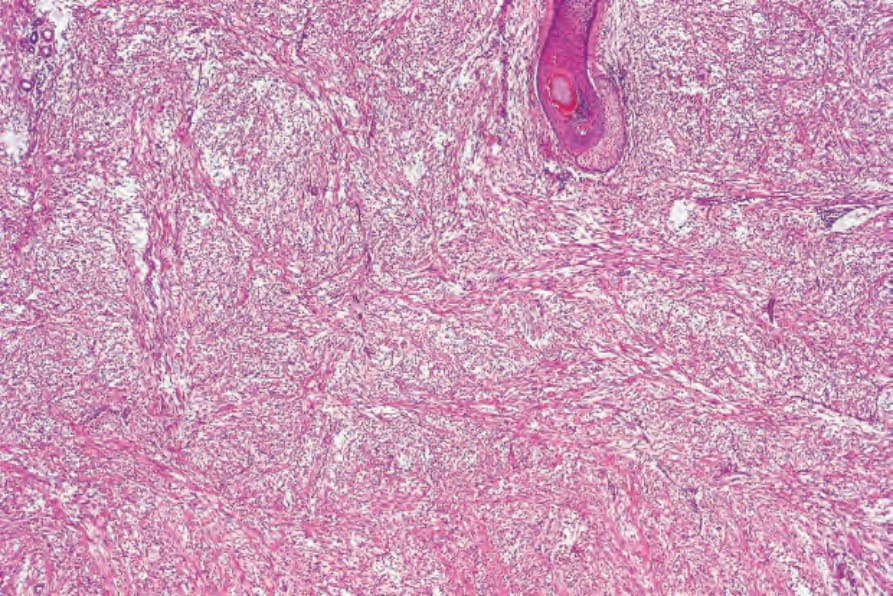
Fig. 35.66 Dermal fasciitis: low-power view showing a myxoid dermal spindled cell proliferation.