Keloid
Keloid
Clinical features A keloid is a common reactive lesion that represents exuberant scar formation. It typically extends beyond the site of original injury.1–5 Although keloids occasionally appear to arise spontaneously, it is believed that most develop as a direct result of local trauma, even if minor or unnoticed (Figs 35.52–35.54).1–5 Keloids also develop as a result of inflammation in conditions such as acne vulgaris. The use of isotretinoin has also been linked to the development of keloids.6 Eruptive keloids associated with aromatase
Keloids usually occur on the head and neck (especially the ear), upper chest and arms, but may be seen at almost any cutaneous site although areas such as the hands and feet and the genitalia are very rarely affected.11 Characteristically, they present as raised, well-circumscribed, rather smooth lesions, becoming progressively more indurated as time passes. They are occasionally itchy or tender and may be multiple, again reflecting individual susceptibility to their development. Irrespective of the treatment used, local recurrence is very common.
Pathogenesis and histologic features The pathogenesis of keloids is not clear but seems to be multifactorial (see also under hypertrophic scar).12 Genetic predisposition and local tissue
1716 Connective tissue tumors
tension play an important role. Collagen synthesis is increased in keloids and the quality of the collagen produced is also different from that in normal skin. Apoptosis is reduced in fibroblasts in keloids.13 There is an increased production of collagen I and III as demonstrated by an increase in levels of mRNA.14 Transforming growth factor beta (TGF-β) seems to play an important role in wound healing and its increased production has been linked to the pathogenesis of keloids by activating the synthesis of collagen by fibroblasts.15,16 The Wnt/β-catenin pathway associated with fibrosis and normal wound healing is strongly up-regulated and epigenetic changes affecting multiple profibrotic pathways are noted.17–19
The interaction between keratinocytes and fibroblasts appears to play an important role in the formation of keloids.20 It has been demonstrated that when keloid fibroblasts are co-cultured with keloid keratinocytes there is increased production of soluble and insoluble collagen and procollagen III mRNA up-regulation.21
The histologic appearances are typified by a nodular fibroblastic proliferation and the presence of hypocellular, ‘glassy’, eosinophilic, thick hyalinized collagen fibers in the dermis (Figs 35.55 and 35.56). Early lesions may show a slight vascularity and foci of myxoid ground substance. Normal mitoses may occasionally be seen.

Fig. 35.52 Prominent keloid developing at the side of a tattoo. By courtesy of Dr J. Dayrit, Manila, The Philippines.
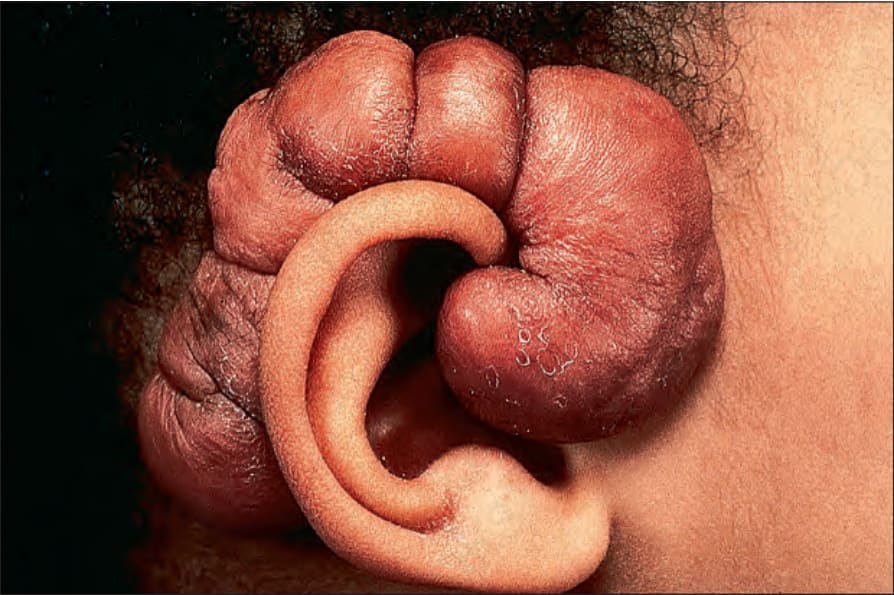
Fig. 35.53 Keloid: lesions commonly follow trauma and are a frequent complication of piercing. By courtesy of the Institute of Dermatology, London, UK.

Fig. 35.54 Keloid: extensive keloid formation can be very disfiguring. By courtesy of the Institute of Dermatology, London, UK.
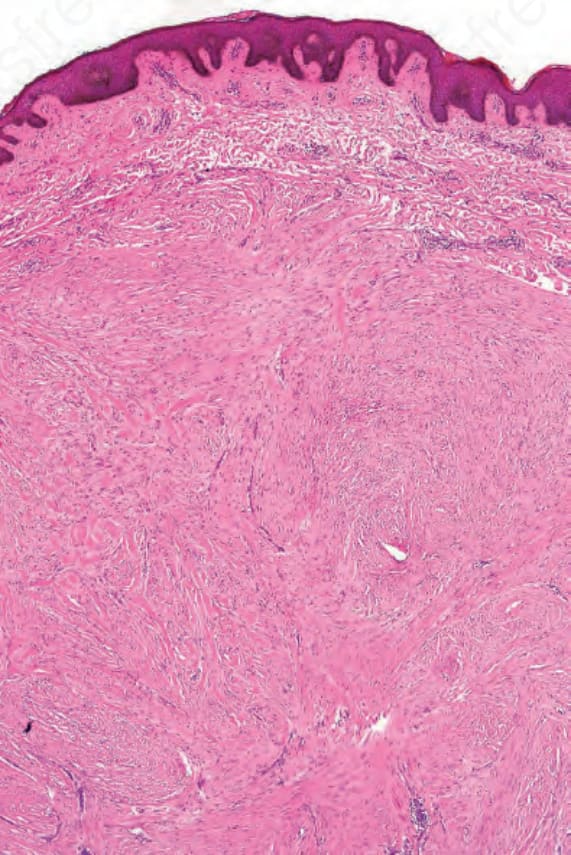
Fig. 35.55 Keloid: this lesion is distinguished from a hypertrophic scar by the presence of broad bundles of eosinophilic, hyalinized collagen.
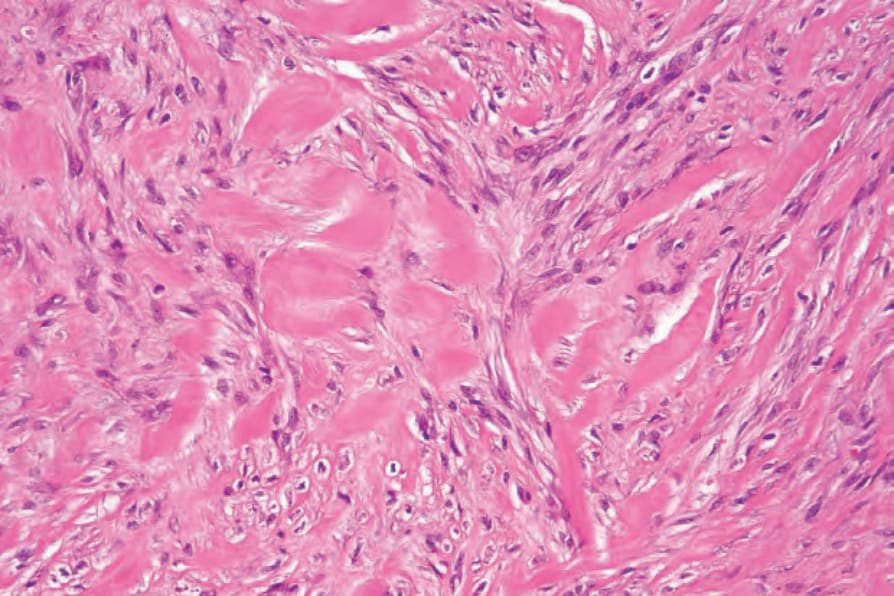
Fig. 35.56 Keloid: high-power view: note the swollen hyalinized collagen bundles admixed with bland spindled cells.