Hypertrophic scar
Hypertrophic scar
Clinical features
Hypertrophic scars occur most frequently on the head and neck, chest, knees and shoulders and show no racial predilection.1–3 Clinically, they may be distinguished from keloids by being less raised and not extending beyond the boundaries of the initiating injury. Unlike keloids, hypertrophic scars are far less prone to recur after treatment, but, in fact, precise distinction
between these two lesions is not always possible and they represent a continuous spectrum.4
Pathogenesis and histologic features Hypertrophic scar appears to be induced by over-activation of dermal wound healing pathways, in some ways similar to that of keloids below.5–9 Transforming growth factor beta 1 has been associated with the induction of both hypertrophic scars and keloids by inducing production of collagen by fibroblasts particularly in early stages.10 It has been proposed that abnormal blood vessel regulation may predispose to keloid and hypertrophic scar formation.11 The Wnt pathway is activated as well, particularly in the proliferative phase.12
1715 Benign fibrous and myofibroblastic tumors and tumorlike lesions
The appearances are typified by a somewhat non-specific dermal fibroblastic proliferation, which is often associated with epidermal atrophy (Figs 35.49–35.51). They tend to be more cellular than keloids, and hyalinized collagen fibers are far less prominent. Mitoses are sometimes noted. A nodular growth pattern is common. Evidence of a foreign body granulomatous reaction may sometimes be present.
inhibitor therapy, after chickenpox and as a paraneoplastic phenomenon, have been reported.7–10 Although these lesions may arise at any age, they are most common in adolescents and young adults; they occur at least four times more frequently in patients of African descent and show a slight predilection for females. A positive family history is not uncommon and probably reflects a genetic predisposition to keloid formation.
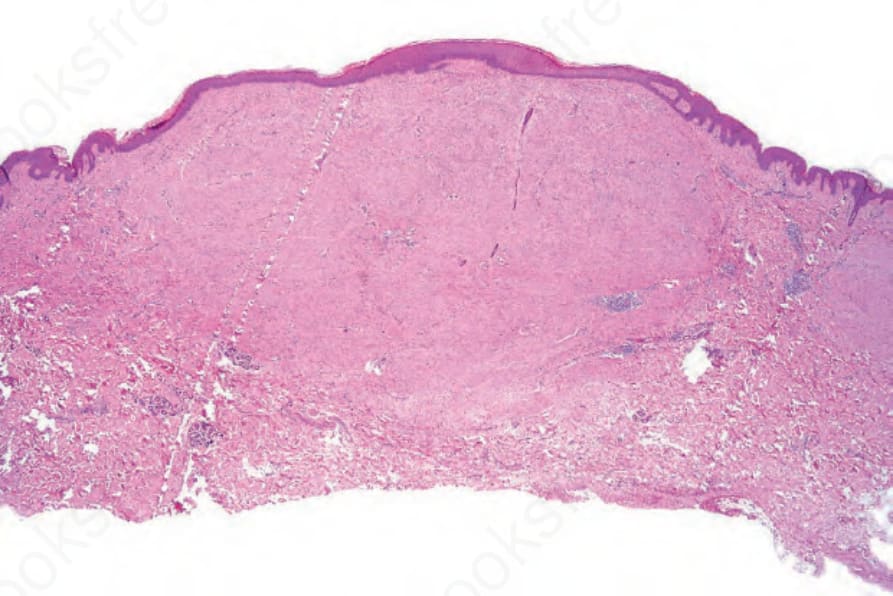
Fig. 35.49 Hypertrophic scar: within the dermis is a nodular fibrous lesion.
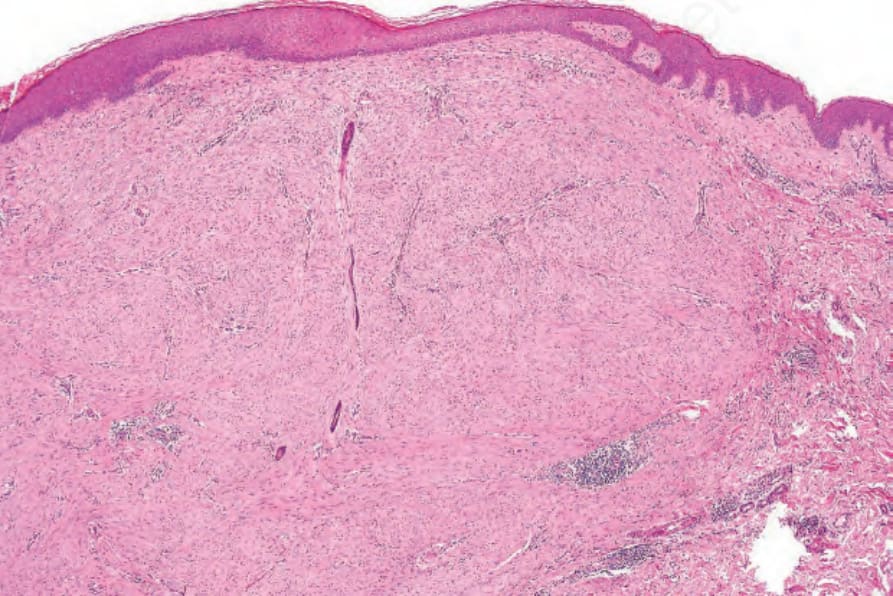
Fig. 35.50 Hypertrophic scar: the lesion is composed of banal fibroblasts with a variably collagenous stroma.
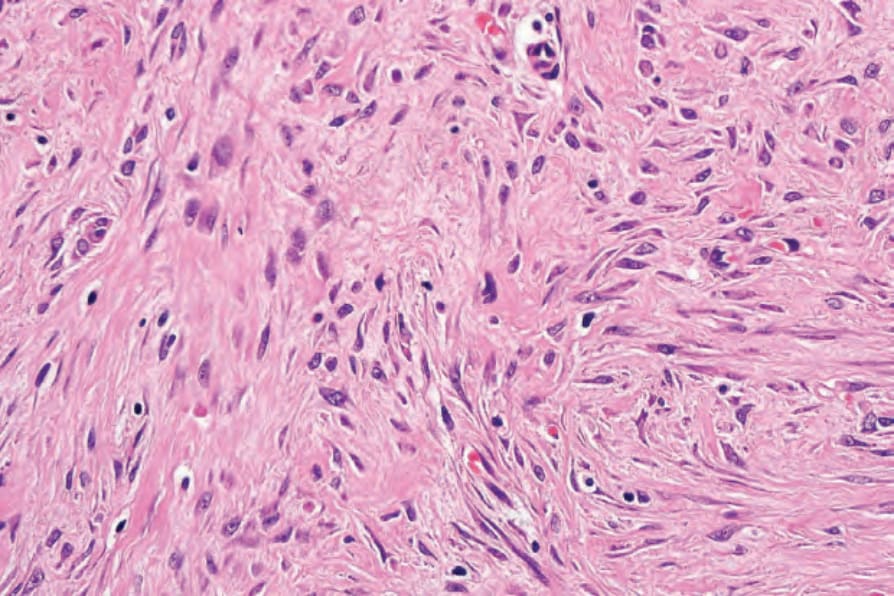
Fig. 35.51 Hypertrophic scar: note the spindled cells and collagenous stroma.

Fig. 35.52 Prominent keloid developing at the side of a tattoo. By courtesy of Dr J. Dayrit, Manila, The Philippines.