Synovial sarcoma
Synovial sarcoma
When biphasic, these tumors usually have a distinctive appearance typified by an undifferentiated spindled cell component with tapering nuclei admixed with well-formed glandular spaces lined by tall columnar PAS-positive, mucin-secreting epithelium (Figs 35.691–35.693). The glandular component very rarely shows apocrine differentiation, and in superficial tumors, this may lead to a diagnosis of carcinosarcoma.6 The relative proportions of the spindled cell and glandular components vary from tumor to tumor and most cases have a monophasic spindle cell appearance (Figs 35.694–35.696). A hemangiopericytoma-like vascular pattern and calcification are common findings, as is the presence of wiry stromal collagen and mast cells.
Clinical features Synovial sarcoma is a relatively common, deep-seated tumor that characteristically arises in the limbs (particularly the legs) of young adults and shows a predilection for males.1–3 Overall age and anatomical distribution is wide, including truncal and head and neck lesions. The dermis is only exceptionally involved by deep-seated tumors. Primary cutaneous synovial sarcoma is vanishingly rare.4,5 Cutaneous metastasis of synovial sarcoma are vanishingly rare.6 A subset of more superficial, minute synovial sarcomas measuring less than 1 cm and with predilection for the hands and feet has been described.7,8 Histologic features are similar to those of ordinary synovial sarcoma. They seem to have a better prognosis than deep-seated lesions.7 The name is misleading as cases show no evidence of a tenosynovial origin.
In general, the prognosis is poor, with eventual metastatic spread and death in at least 50% of patients. The tumor tends to metastasize late, and long follow-up is therefore necessary.9
The glandular spaces and some of the adjacent spindled cells stain positively for epithelial markers, including keratin and EMA (Fig. 35.697).30,31 The markers, especially EMA, are also usually positive, albeit focally, in the monophasic variant. These findings usually allow distinction from malignant schwannoma and fibrosarcoma, the latter now being regarded as extremely rare. Focal positivity for S100 protein and CD99 may also be seen.32,33 Nuclear expression of the immunohistochemical marker TLE1 identified in a synovial sarcoma gene expression study appears to be specific and can be helpful.34–37 Reduced immunohistochemical expression of INI1 (encoded by SMARCB1) is a helpful diagnostic feature.38–40 This results from the SS18-SSX fusion protein perturbing the SWI/SNF BAF complex, a multiprotein complex that includes INI1.41,42
1892 Connective tissue tumors
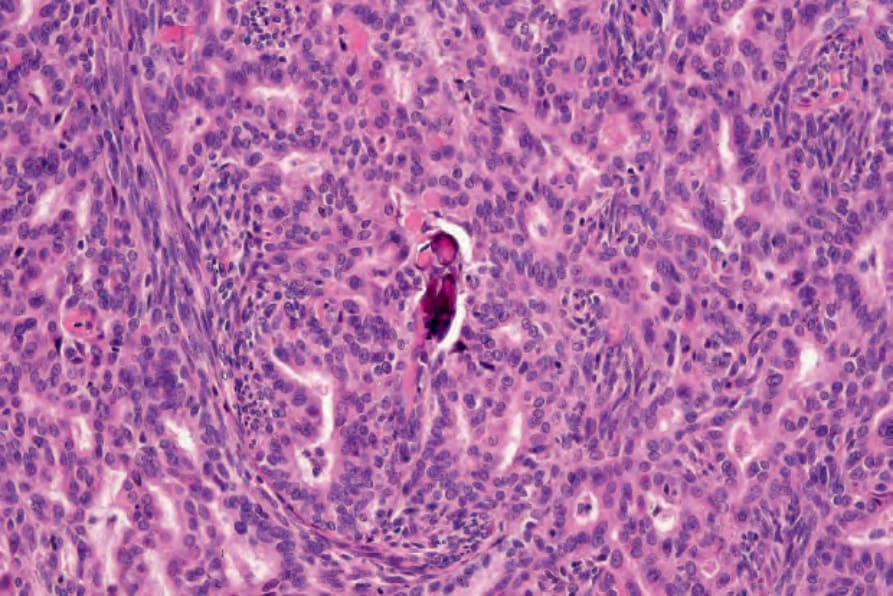
Fig. 35.691 Synovial sarcoma: this field shows the characteristic biphasic population of spindle cells and glandular spaces.
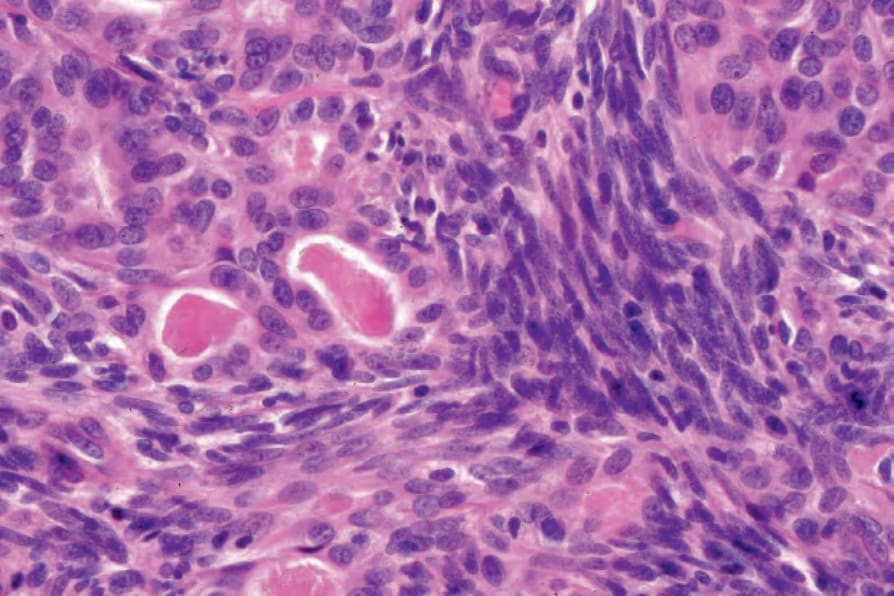
Fig. 35.692 Synovial sarcoma: the glandular spaces contain eosinophilic material.
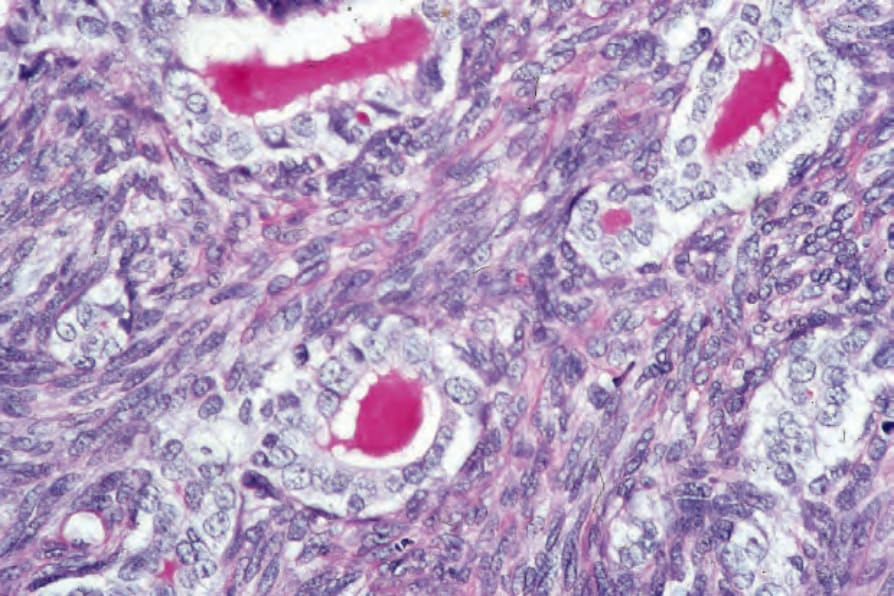
Fig. 35.693 Synovial sarcoma: the secretion is diastase–PAS positive.
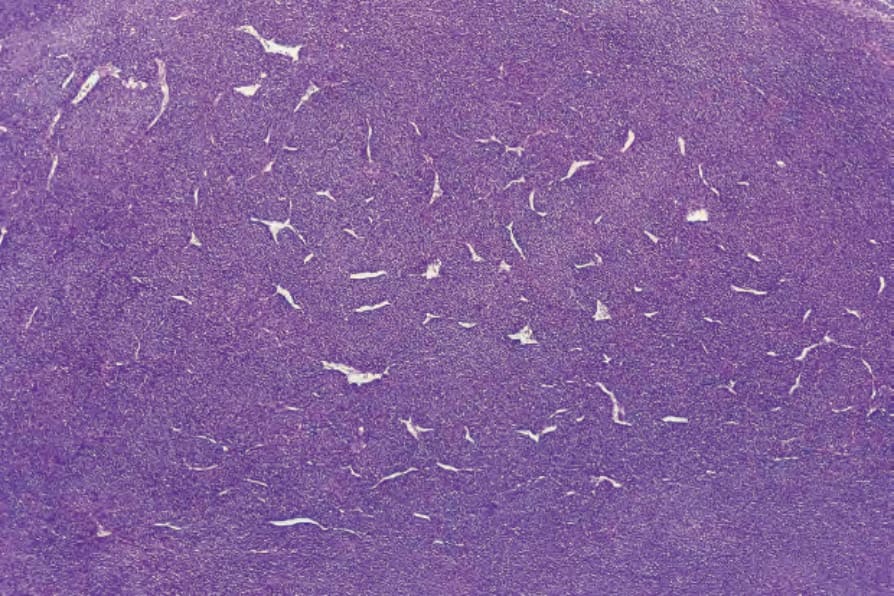
Fig. 35.694 Synovial sarcoma: low-power view of a monophasic example showing the characteristic hemangiopericytomatous blood vessels.
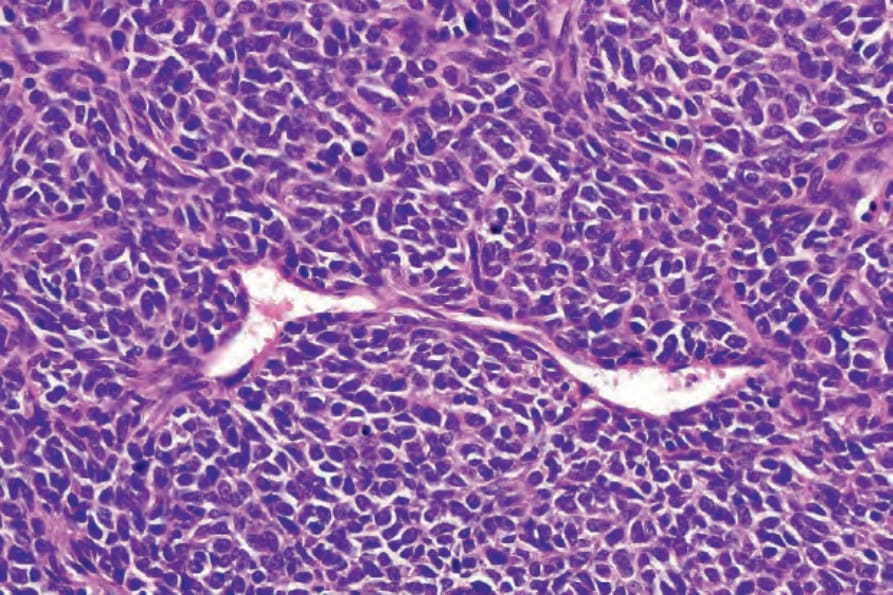
Fig. 35.695 Synovial sarcoma: high-power view showing hyperchromatic tumor cells with indistinct cytoplasm.
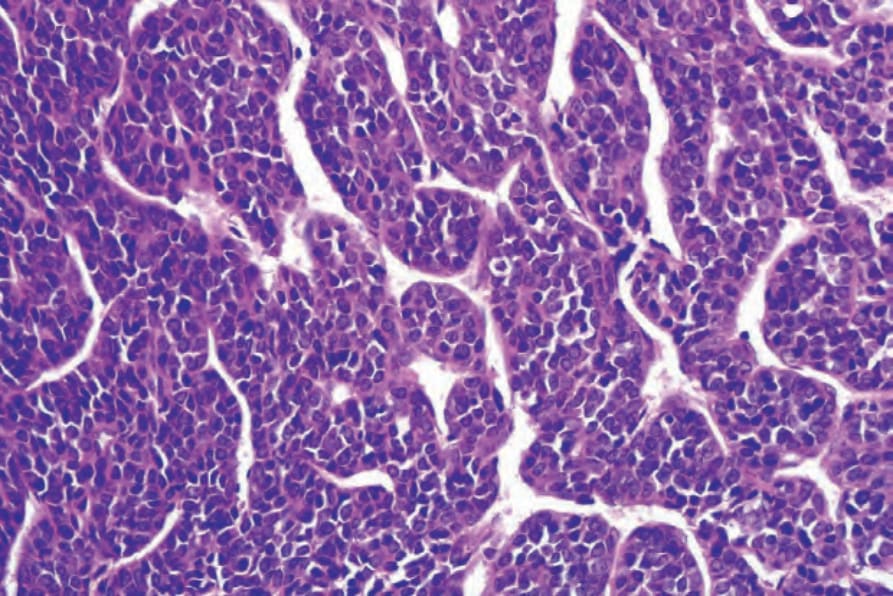
Fig. 35.696 Synovial sarcoma: this example highlights the vascular pattern.
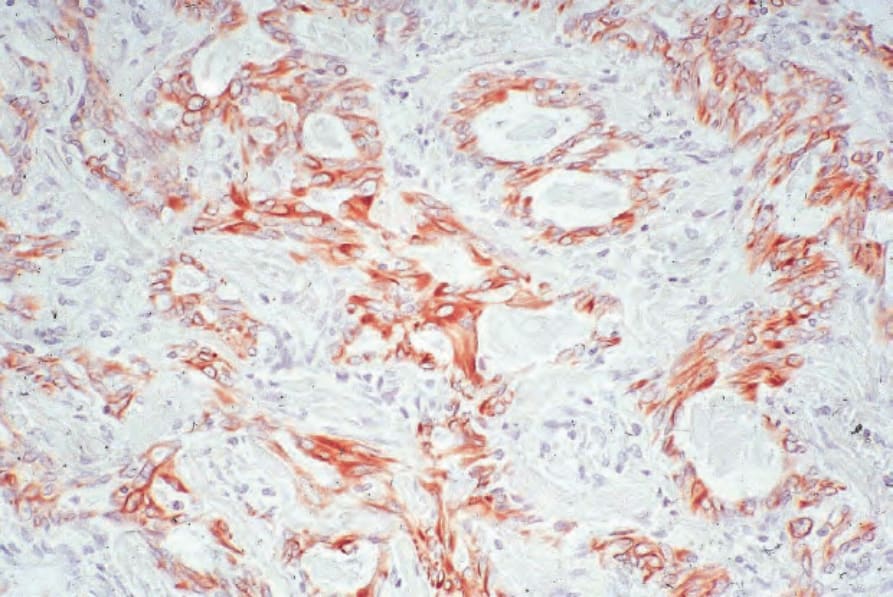
Fig. 35.697 Synovial sarcoma: the glandular component expresses keratin.