Epithelioid sarcoma
Epithelioid sarcoma
Clinical features Epithelioid sarcoma is a comparatively rare tumor arising most often on the distal extremities (particularly the hand and wrist) of young adults, especially males.1–5 Occurrence in children is uncommon.6 The overall age range and the anatomical distribution are wide. Rare cases present in the head and even in the oral cavity and parotid gland (Figs 35.676 and 35.677).7–10 It is predominantly a dermal or subcutaneous tumor that presents as a slow-growing, elevated, often tender nodule(s) measuring less than 5 cm in diameter. Ulceration is a common feature. Due to the distinctive tendency for extensive spread of the tumor along blood vessels, nerves, and fascia, the presence of satellite nodules at a distance from the main tumor is common. The tumor may mimic other diseases including perforating granuloma annulare and Dupuytren disease.11,12
nuclear expression encoded by SMARCB1 (INI1) at 22q11.23 is characteristic and likely critical for the pathogenesis.23–26 Other abnormalities have been found in 8q and monosomy 21 has also been documented.21 Overall, there are complex genomic cases and loss of CDKN2A is common, in contradistinction to the simple genomic profile of rhabdoid tumor with SMARCB1 loss.27 Abnormalities of chromosomes 8 and 22 have also been found to be involved in the proximal-type of epithelioid sarcoma.28
Indolent and repeated locoregional recurrence is common. Metastasis to the lymph nodes, an unusual feature in other sarcomas, is quite common, followed by metastasis to the lungs. Although the overall 5-year survival is about 70%, the 20-year survival is no more than 20–25%.2,3 Improved prognosis appears to be related to smaller tumor size.3
A group of epithelioid sarcomas arising in pelvi-perineal locations (including the vulva) have a very aggressive clinical course, more so than the ordinary variant, and have been described as proximal-type epithelioid sarcoma.13–17 Similar cases exceptionally occur in other locations.18 Independent indicators of worse biological behavior are early metastases and large tumor size.19
Pathogenesis and histologic features The most consistent cytogenetic abnormality in cases studied so far has been loss of heterozygosity of chromosome 22q.20–22 Loss of INI1 (BAF47)
An NRAS oncogene mutation has been described in a case of metastatic epithelioid sarcoma.29
The microscopic appearances are distinctive (Figs 35.678–35.680). The tumor is composed of multiple nodules of polygonal, epithelioid, or spindle-shaped cells with eosinophilic cytoplasm which show variable pleomorphism. Mitoses are often scanty. Giant cell forms are occasionally seen. At the center of these nodules, focal necrosis is a prominent feature in around 50% of cases, producing an appearance reminiscent of a granulomatous process (Fig. 35.681). Other cases show a vague fibrinoid or myxoid pattern of degeneration. The latter may predominate in rare cases. At the periphery of the nodules, the tumor cells tend to be more spindle shaped, and in rare cases this feature can be prominent (see below).18,30 Vascular and perineural invasion is often present (Fig. 35.682). In a small number of
1889 Epithelioid sarcoma
cases, spindle-shaped cells predominate, they are arranged in bundles and necrosis is minimal or absent. This variant is known as fibroma-like.30,31 In a few cases, an angiomatoid pattern is seen.31 Heterotopic bone formation is exceptional.32
Immunohistochemically, more than 90% of cases are positive for vimentin, cytokeratin and EMA (Figs 35.683 and 35.684) and up to 60% are positive for CD34.33–36 SMA is also often focally positive. The combination of vimentin, CD34 and keratin positivity is very useful in the diagnosis of epithelioid sarcoma. The immunohistochemical profile of proximal-type epithelioid sarcoma is similar to that of classic epithelioid sarcoma. Both forms show loss of nuclear INI1 expression in greater than 90 % of cases, a relatively specific finding within the reasonable differential diagnoses.37–39 GLUT-1 is not a useful marker in the diagnosis of epithelioid sarcoma.40 CA125 has been reportedly often positive in epithelioid sarcoma and negative in reactive and neoplastic conditions that can mimic this tumor.41 Proximal epithelioid sarcoma is characterized by a diffuse growth pattern (Figs 35.685 and 35.686). Tumor cells are mainly epithelioid and mitotic activity is often brisk (Fig. 35.687). Focal or extensive rhabdoid change is often present (Figs 35.688–35.690).17 Necrosis seems to be less common than in the ordinary variant.
1890 Connective tissue tumors
1891 Synovial sarcoma
Ultrastructural studies show that the epithelioid tumor cells contain well-formed desmosome-like junctions and aggregates of intermediate filaments, often in a paranuclear location.35 In a case of proximal-type epithelioid sarcoma immunoelectron microscopy demonstrated keratin filaments but not vimentin, suggesting a closer relation to epithelial cells than to mesenchymal cells.42
Differential diagnosis The distinctive histologic features in an appropriate clinical setting usually prevent diagnostic confusion. Lack of awareness of this entity may lead to the mistaken diagnosis of necrotic metastatic carcinoma or a granulomatous inflammatory lesion. Distinction from epithelioid hemangioendothelioma or angiosarcoma can be difficult because often in epithelioid sarcoma there are pseudovascular clefts and focal cytoplasmic vacuolation. However, cells in the former tend to grow in cords, at least focally, and are often larger; they stain positively for endothelial markers and are frequently keratin positive. Malignant rhabdoid tumor shows many cells with intracytoplasmic inclusions, and although immunohistochemically the tumor cells are positive for epithelial markers, they also usually show positivity for other markers, indicating divergent differentiation. Furthermore, rhabdoid tumors have distinctive vesicular nuclei with macronucleoli. Deep granuloma annulare and rheumatoid nodule can mimic epithelioid sarcoma, particularly on low-power examination.43 However, the former entities show neither cytologic atypia nor mitotic activity, there is absence of necrosis and presence of necrobiosis with either fibrin or mucin deposition, and histiocytes are positive for CD68 and negative for keratin and CD34.44
Factors that seem to correlate with prognosis include age, size of the tumor, histologic features, stage, tumor grade, and molecular alterations.10–21 Children and adolescents have better prognosis than adults, and tumors presenting on the limbs have better behavior than those arising on the head and neck. Histologic features associated with better prognosis proportion of poorly differentiated tumor (more than 20%), size less than 5 cm in diameter (minute synovial sarcomas have excellent prognosis), less than 5 mitoses in 1.7 mm2 and absence of necrosis.7,10 NY-ESO-1expression is useful to identify cases for immunotherapy targeted therapy.11,12
Pathogenesis and histologic features Most cases of synovial sarcoma including monophasic and biphasic variants show a balanced t(X;18)(p11;q11) which fuses either SSX1, SSX2 or very rarely SSX4, situated together on the X chromosome, with SS18 (previously termed SYT). A t(X;20)(p11;q13) resulting in SS18L1-SSX1 fusion has also been documented.22–24 Involvement of SSX1 is more common in biphasic tumors while any of the three can be involved in the monophasic form.25 The prognostic value of the different fusion types is debated, but is likely small.26–29

Fig. 35.676 Epithelioid sarcoma: the hand is a commonly affected site. By courtesy of Dr. Yi-Guo Feng, Xian, China.
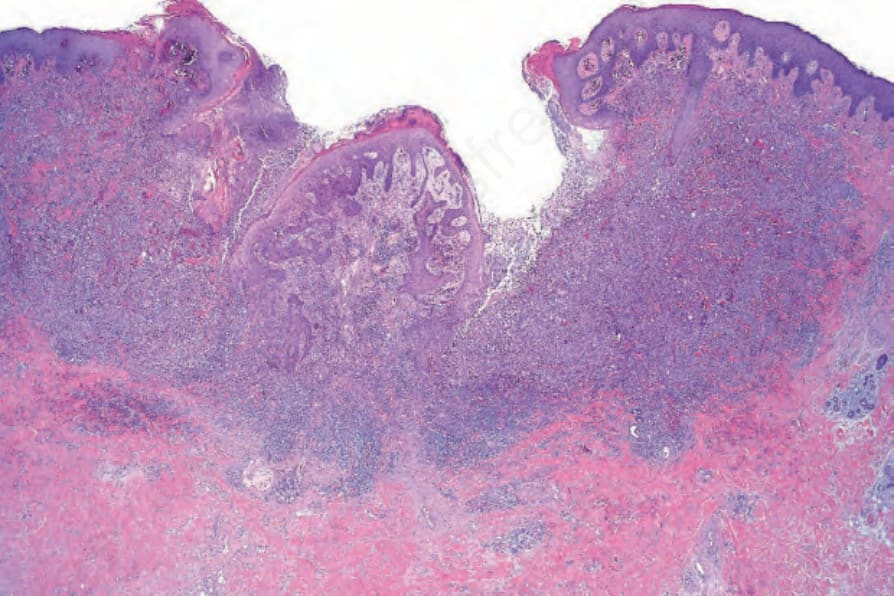
Fig. 35.678 Epithelioid sarcoma: the upper dermis is diffusely infiltrated by an ulcerated tumor.
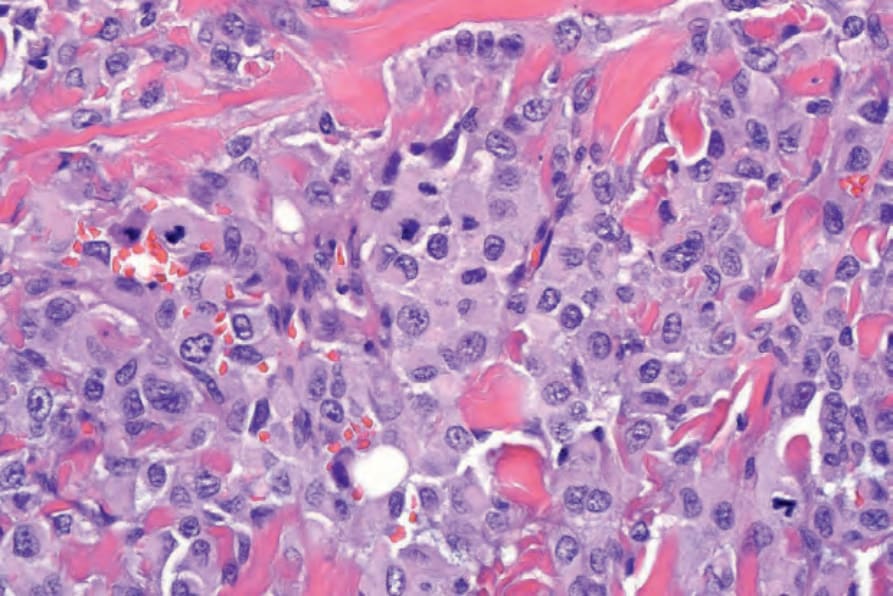
Fig. 35.679 Epithelioid sarcoma: in this field the tumor cells are epithelioid with abundant eosinophilic cytoplasm and large vesicular nuclei.
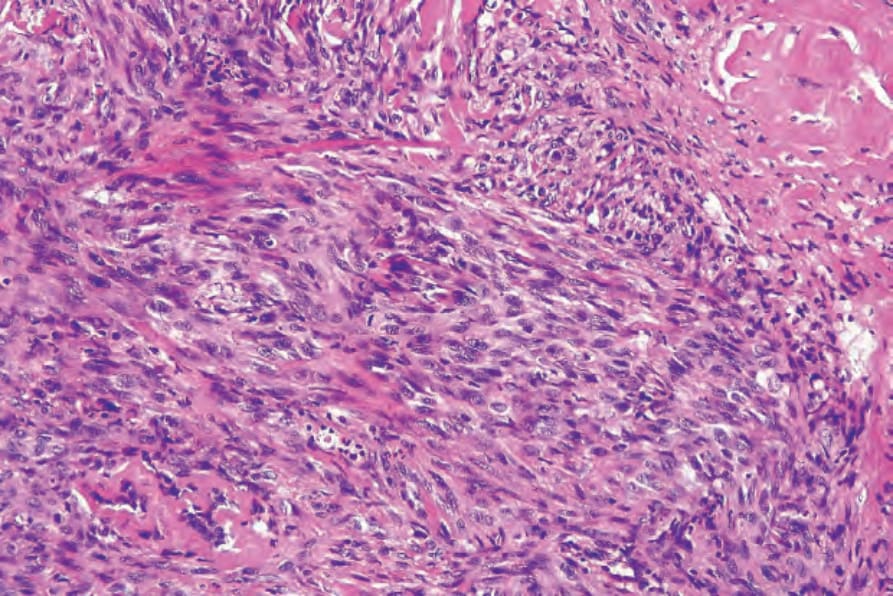
Fig. 35.680 Epithelioid sarcoma: elsewhere the tumor cells have a spindled morphology.
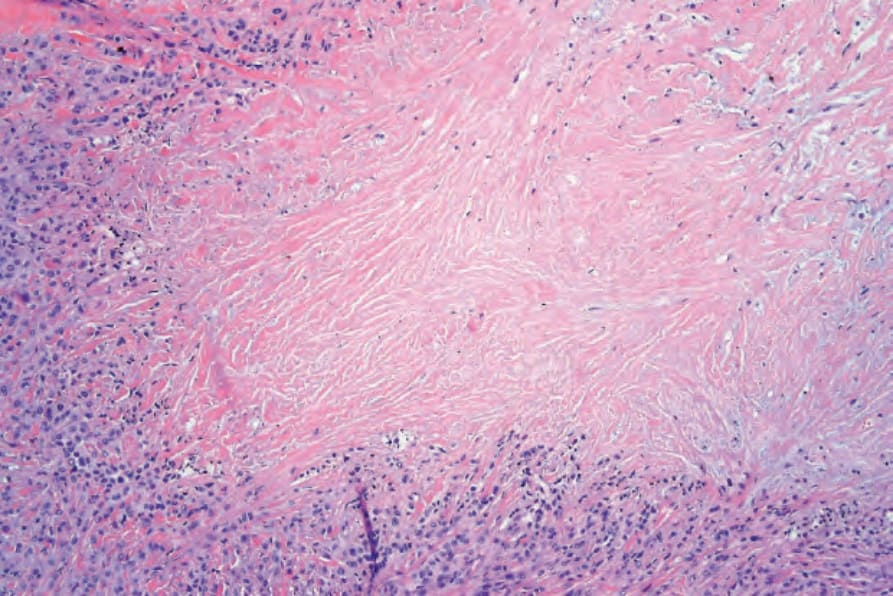
Fig. 35.681 Epithelioid sarcoma: geographical necrosis seen at low-power examination may result in diagnostic confusion with a granulomatous process.
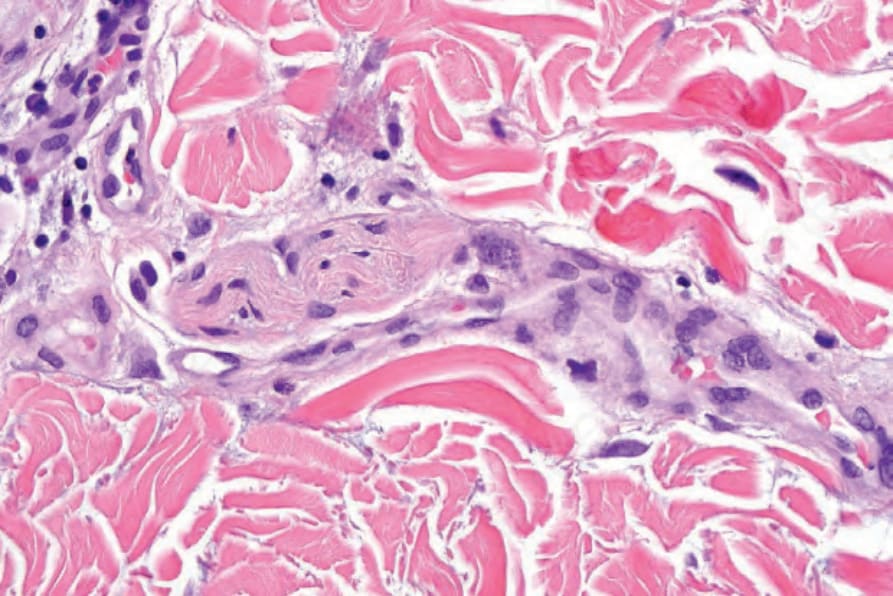
Fig. 35.682 Epithelioid sarcoma: the tumor commonly extends along nerve trunks, in part accounting for its high recurrence rate.
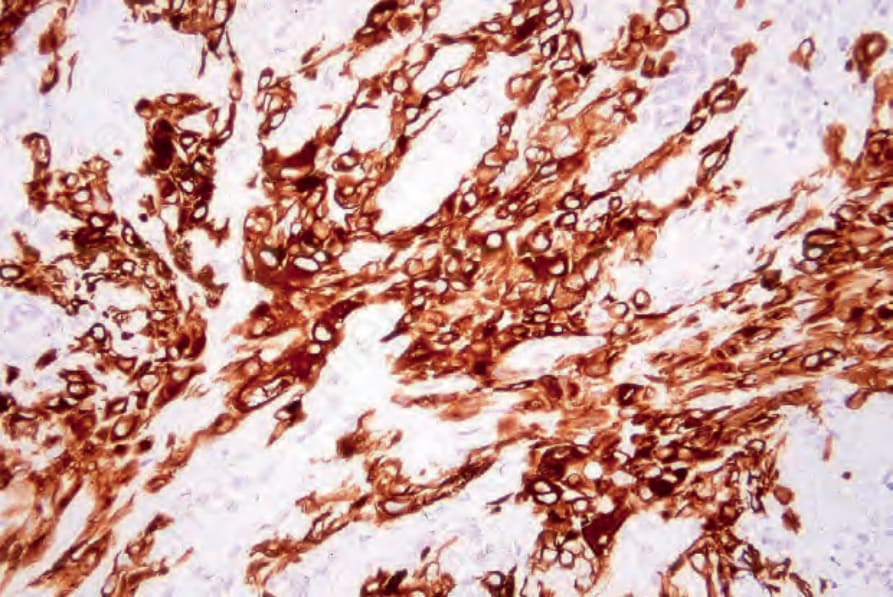
Fig. 35.683 Epithelioid sarcoma: the tumor cells characteristically express keratin, as shown in this field.
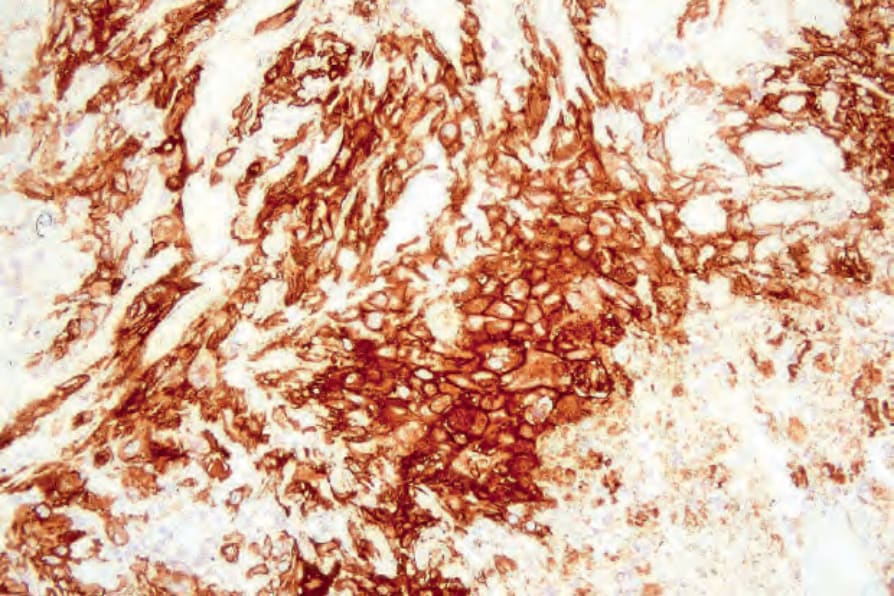
Fig. 35.684 Epithelioid sarcoma: epithelial membrane antigen positivity is usually evident.
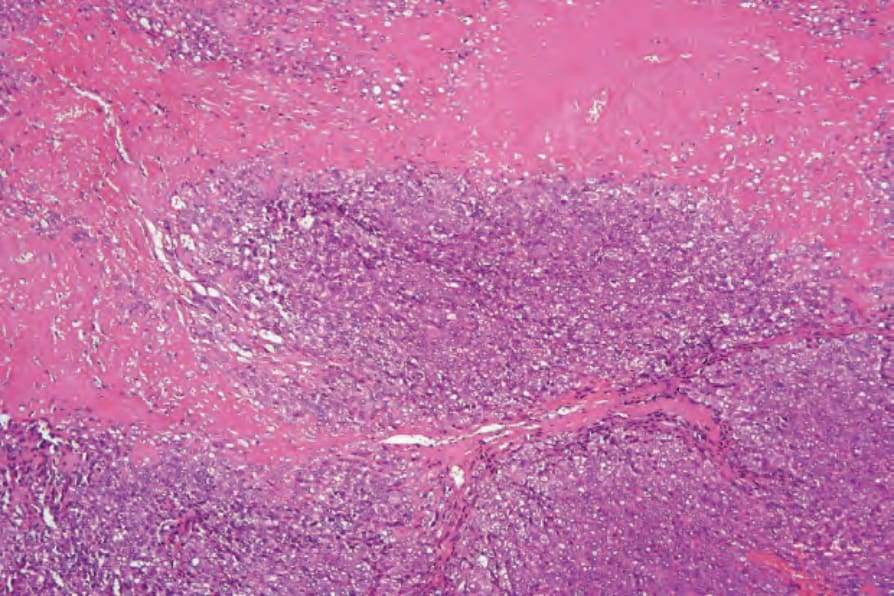
Fig. 35.685 Proximal epithelioid sarcoma: the tumor is characterized by a diffuse cellular infiltrate with widespread necrosis.
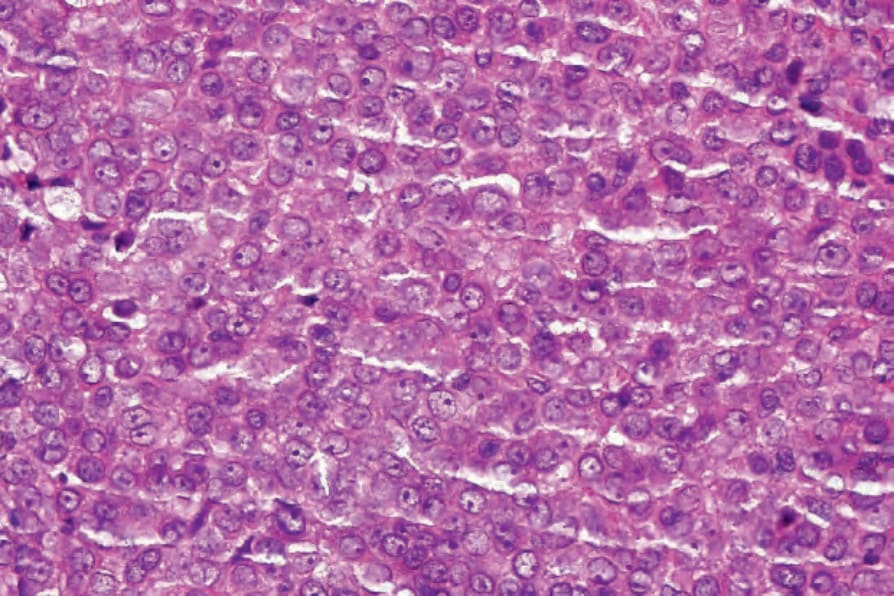
Fig. 35.686 Proximal epithelioid sarcoma: the tumor cells are epithelioid with eosinophilic cytoplasm and round vesicular nuclei containing conspicuous nucleoli.
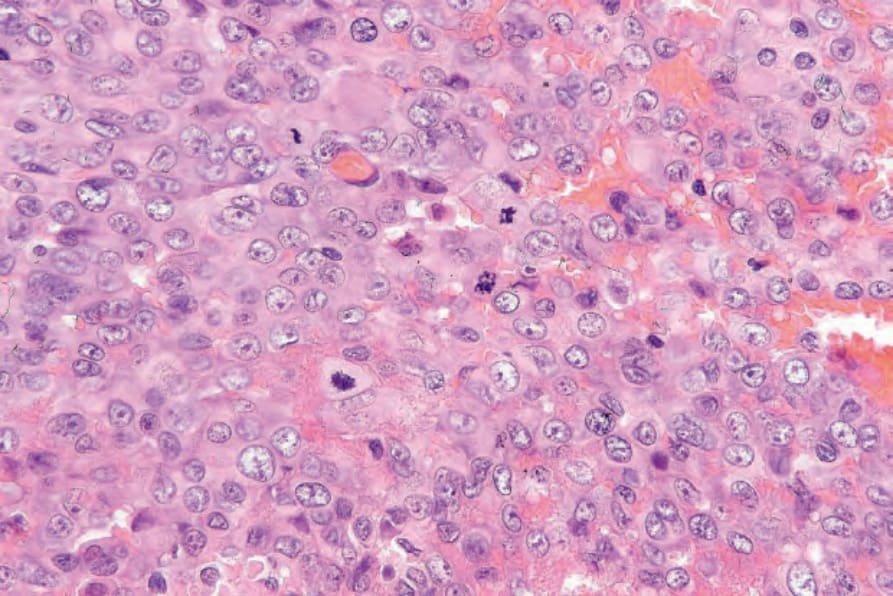
Fig. 35.687 Proximal epithelioid sarcoma: in this example, there is marked mitotic activity.
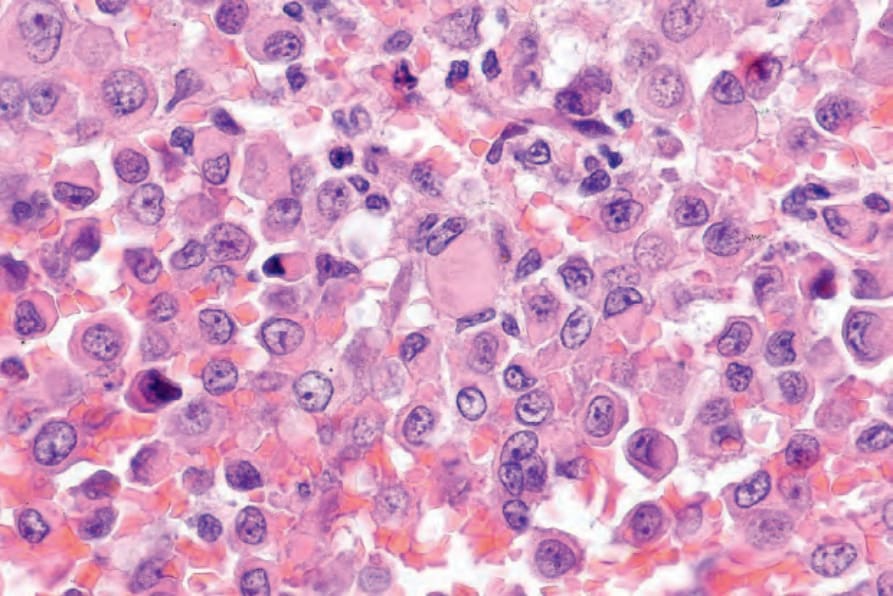
Fig. 35.688 Proximal epithelioid sarcoma: rhabdoid inclusions, as seen in the center of the field, are often present.
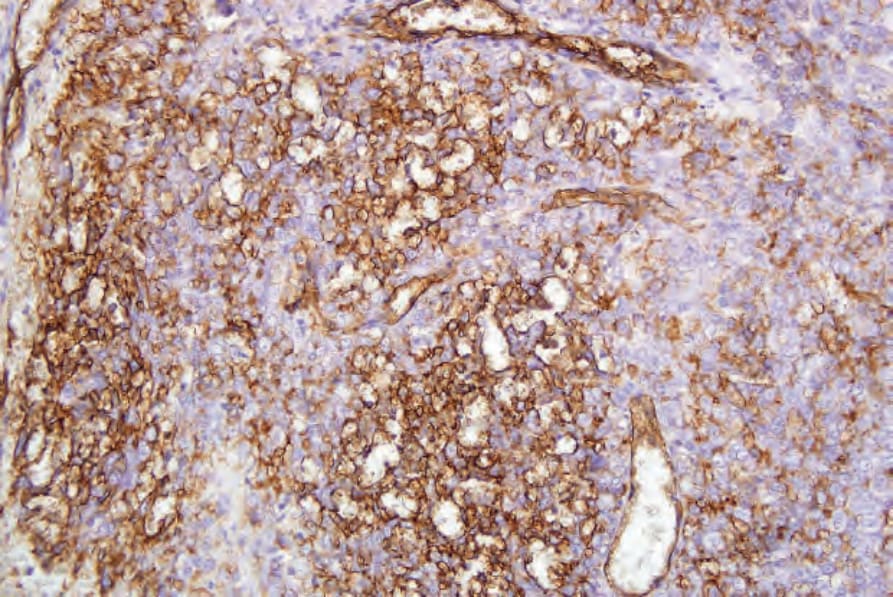
Fig. 35.689 Proximal epithelioid sarcoma: the tumor cells are positive for keratin (AE1/AE3).
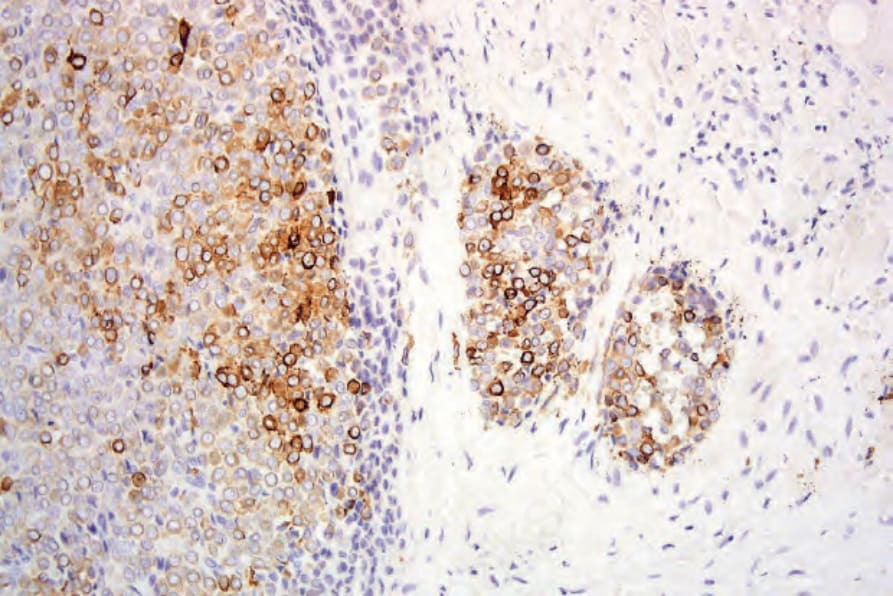
Fig. 35.690 Proximal epithelioid sarcoma: CD34 is also expressed in this example.
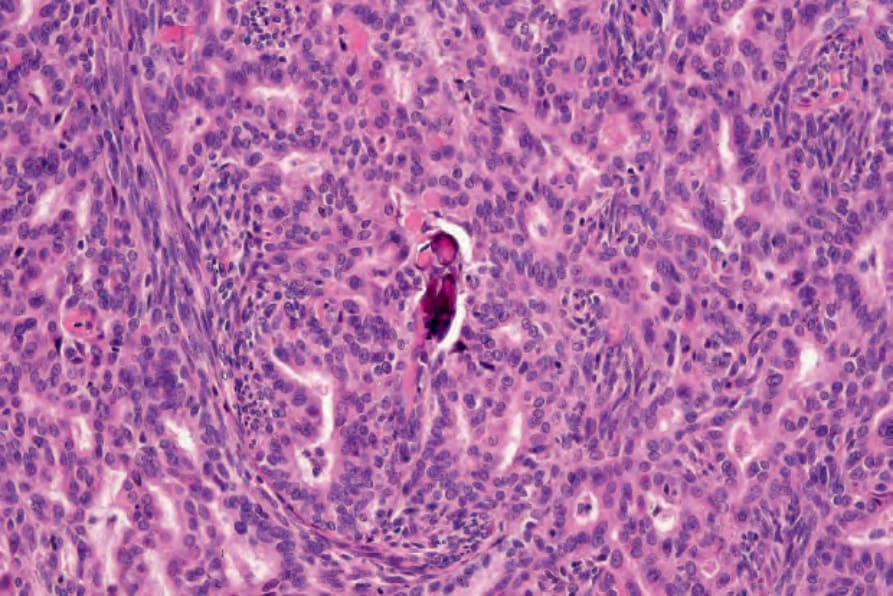
Fig. 35.691 Synovial sarcoma: this field shows the characteristic biphasic population of spindle cells and glandular spaces.