Superficial acral fibromyxoma
Superficial acral fibromyxoma
Clinical features Superficial acral fibromyxoma (digital fibromyxoma) is a distinctive, relatively rare benign tumor with predilection for the fingers and toes, followed by the palm.1–25 Identical lesions have been described under the rubric cellular digital fibroma.6,7,20 Involvement of the nail region is very common. Lesions on the heel are rare.5 Patients are usually young to middle-aged
1883 Superficial acral fibromyxoma
adults and there is predilection for males. Tumors are small, slowly growing and asymptomatic. Local recurrence after excision is rare.8
Pathogenesis and histologic features RB1 gene deletions have been recently documented, suggesting a possible relationship to other RB1-deleted neoplasms such as spindle cell/pleomorphic lipoma, mammary-type myofibroblastoma, and cellular angiofibroma.23
Histology shows a fairly circumscribed dermal and/or subcutaneous tumor composed of bland, spindle-shaped or stellate cells with a focal storiform or fascicular pattern in a myxoid or collagenous stroma (Fig. 35.660). Lesions contain scattered small vascular channels. Some tumors are more cellular than others and in these, myxoid change tends to be very focal (Fig. 35.661).3 An adipocytic component is exceptional.9
Mitotic figures are rare and cytologic atypia is mild or absent. Mast cells are often present.
By immunohistochemistry, tumor cells are usually positive for CD34 and may be focally positive for EMA, SMA, CD99, CD10, and nestin.1–5,17,24 Desmin positivity has only been reported in one case.17 There is loss of expression of RB1.23 Ultrastructurally, tumor cells show cytoplasmic intermediate filaments and rough endoplasmic reticulum, indicating fibroblastic differentiation.10
1884 Connective tissue tumors
Differential diagnosis
The differential diagnosis includes neurofibroma, onychomatricoma, dermatofibrosarcoma protuberans, minute synovial sarcoma and low-grade fibromyxoid sarcoma. Neurofibroma is rare in acral sites and, although tumor cells may be focally positive for CD34, they are also positive for S100 protein. The stromal component in onychomatricoma may be identical to that seen in superficial acral fibromyxoma with CD34-positive cells. Distinction is based in the presence of distinctive epithelial changes in onychomatricoma.11 A focal storiform pattern may mimic dermatofibrosarcoma protuberans. However, the latter is vanishingly rare in the distal extremities, infiltrates the subcutaneous tissue diffusely and is positive for apolipoprotein D.12 Minute synovial sarcoma of the hands and feet can have similar appearances to superficial acral fibromyxoma with myxoid stroma and bland spindle-shaped cells.13 However, in the former there are focal areas of calcification, tumor cells are at least focally positive for keratin and cytogenetic analysis shows a tX;18 translocation. Negativity for MUC4 rules out low-grade fibromyxoid sarcoma.
Hemosiderotic fibrolipomatous tumor/hemosiderotic fibrohistiocytic lipomatous lesion
Clinical features Hemosiderotic fibrolipomatous tumor (hemosiderotic fibrohistiocytic lipomatous lesion) develops almost exclusively on the foot, particularly the ankle, with predilection for females.1–3 Most patients are adults but children may rarely be affected. It grows slowly and is asymptomatic. Simple excision is the treatment of choice. Local recurrence may occur.
studies is that although there is a pathogenetic link between hemosiderotic fibrohistiocytic lipomatous tumor and pleomorphic hyalinizing angiectatic tumor, it is unlikely that these tumors are related to pure cases myxoinflammatory fibroblastic sarcoma.5–24
Pathogenesis and histologic features Hemosiderotic fibrohistiocytic lipomatous lesion was thought to be the result of trauma. It has also been suggested that the lesion may develop as a result of stasis.4 However, it is now clear that it represents a neoplastic process of unkown histogenesis.5,6 A consistent t(1;10) with rearrangements of TGFBR3 and MGEA5 have been described.7 The same translocation is seen in a subset of myxoinflammatory fibroblastic sarcoma. It has been suggested that there is a histogenetic link between this tumor, pleomorphic hyalinizing angiectatic and myxoinflammatory fibroblastic sarcoma. This has been discussed under the latter entity. The conclusion based on a number of
Histology shows a fairly well-circumscribed mass composed of abundant mature adipose tissue admixed with focal bundles of plump spindle-shaped cells with vesicular nuclei and a small inconspicuous nucleolus. Cytologic atypia is mild and mitotic figures are very rare. A striking feature is the presence of prominent hemosiderin deposition, particularly in the spindle cell areas (Figs 35.662 and 35.663). Focal areas of the tumor may display features reminiscent of myxoinflammatory fibroblastic sarcoma. Early lesions display histologic features that are identical to those seen in pleomorphic hyalizing angiectatic tumor.
By immunohistochemistry, the spindle cells are positive for vimentin, calponin and CD34, and focally positive for KP1.
1885 Myoepithelioma of soft tissue
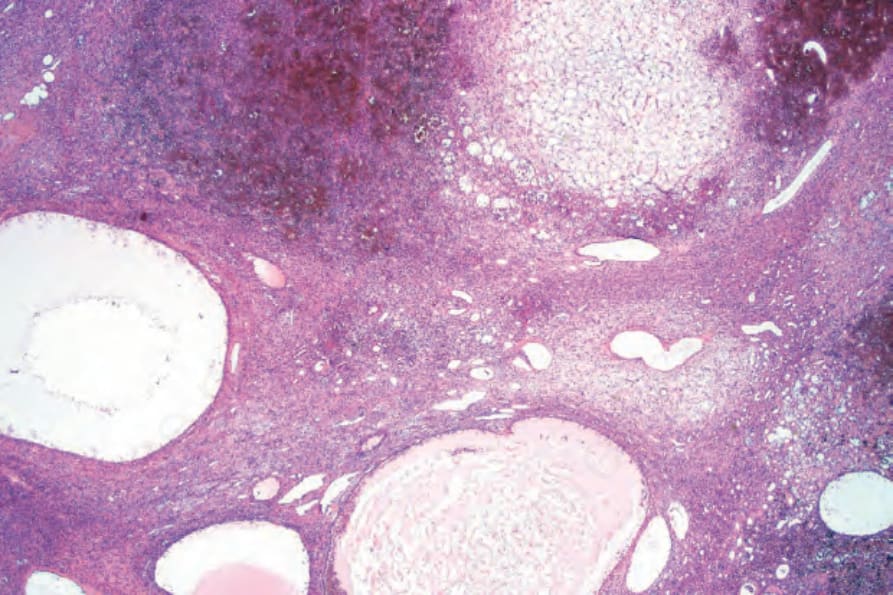
Fig. 35.656 Phosphaturic mesenchymal tumor: scanning view showing cysts, blood vessels, focal hemorrhage and a myxoid stroma.
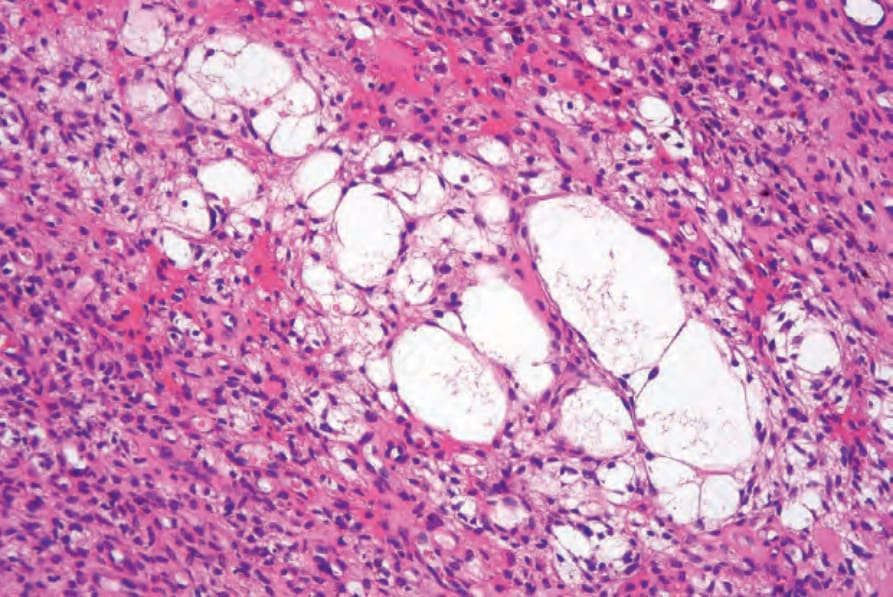
Fig. 35.657 Phosphaturic mesenchymal tumor: the tumor cells have eosinophilic cytoplasm and hyperchromatic spindled nuclei. Microcysts are present.
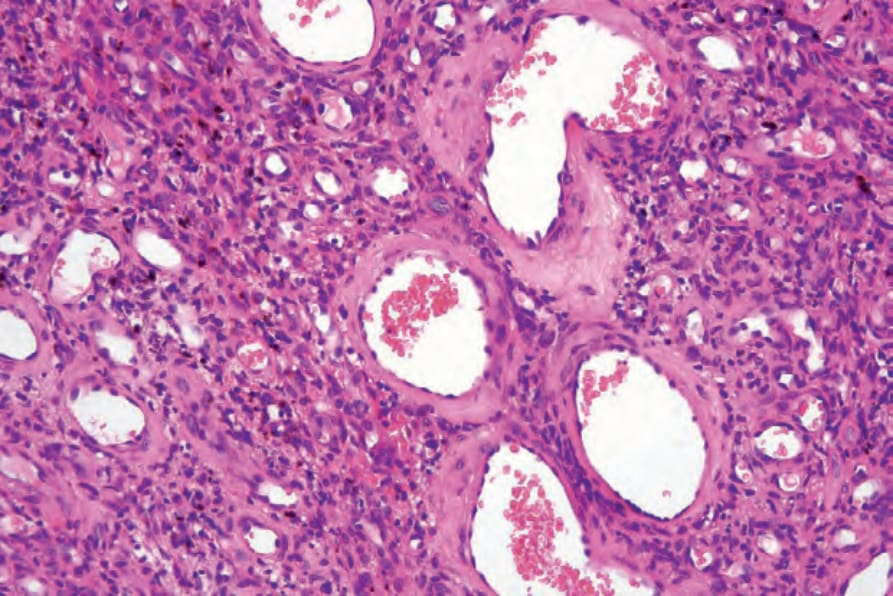
Fig. 35.658 Phosphaturic mesenchymal tumor: higher-power view showing tumor cells and blood vessels.
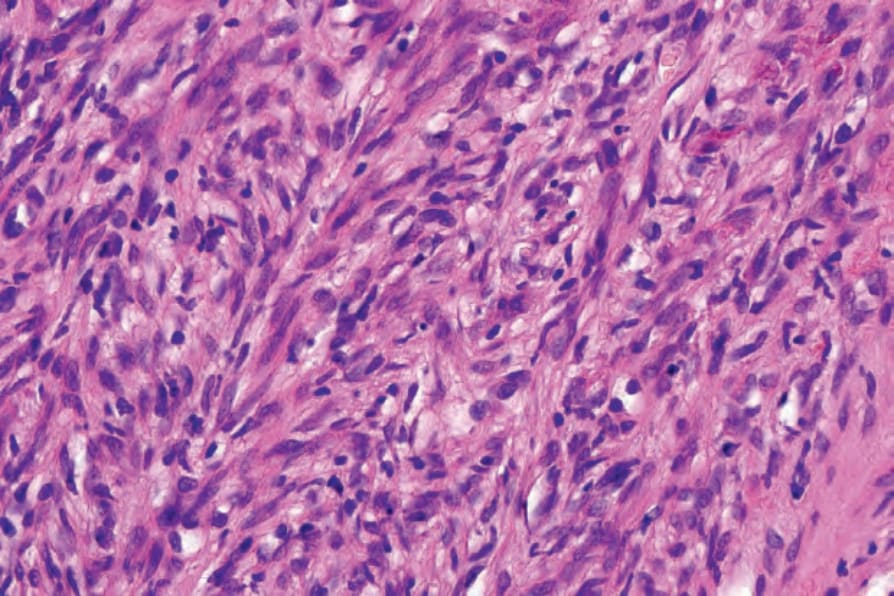
Fig. 35.659 Phosphaturic mesenchymal tumor: high-power view of spindled cells showing a vaguely fascicular growth pattern.
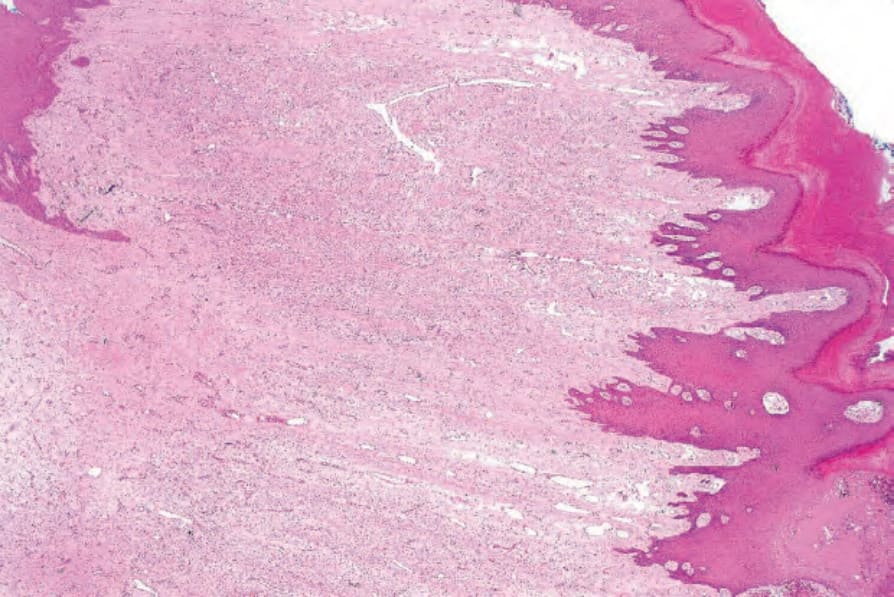
Fig. 35.660 Superficial acral fibromyxoma: low-power view of a vascular spindle cell tumor with a myxoid stroma.
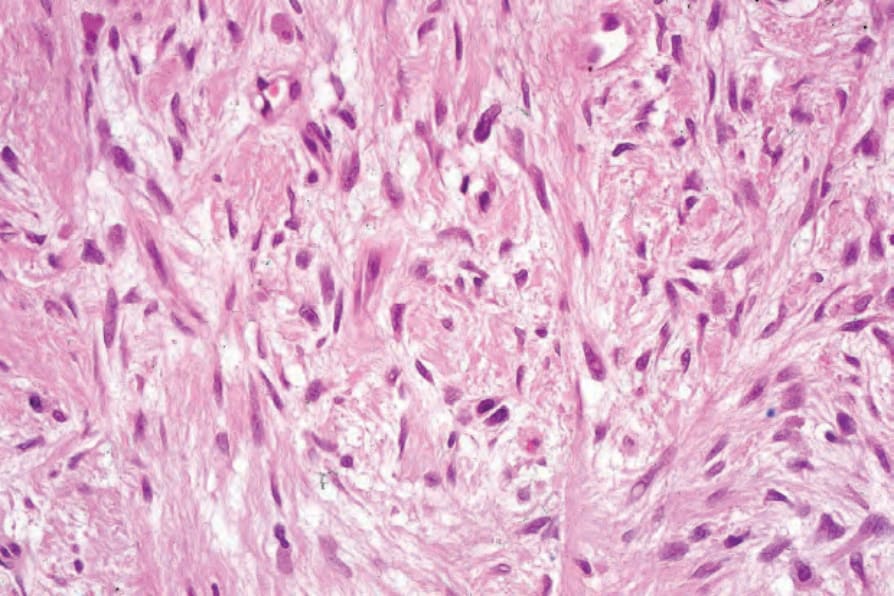
Fig. 35.661 Superficial acral fibromyxoma: high-power view of bland spindled cells in a myxoid stroma.
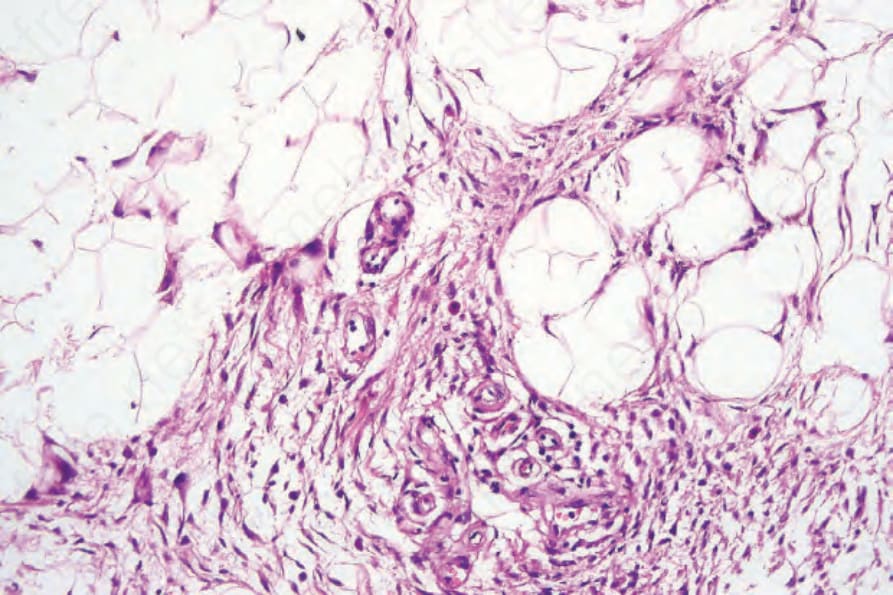
Fig. 35.662 Hemosiderotic fibrohistiocytic lipomatous lesion: there are lobules of mature adipocytes containing scattered areas of spindled cells and histiocytes.
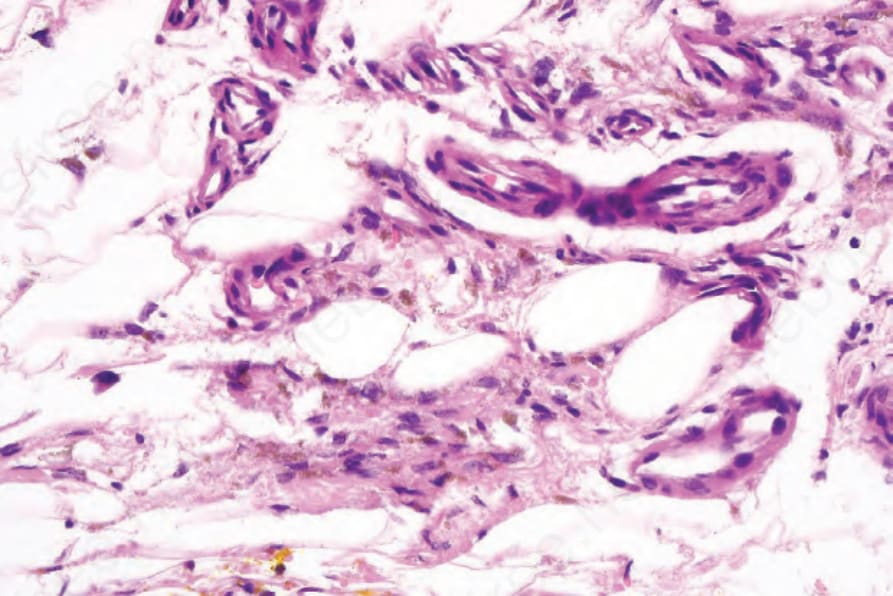
Fig. 35.663 Hemosiderotic fibrohistiocytic lipomatous lesions: there are bland spindle-shaped cells and prominent hemosiderin.