Superficial angiomyxoma
Superficial angiomyxoma
Clinical features Superficial angiomyxoma comprises a relatively uncommon group of lesions which present on the head, neck or trunk of adults as slowly growing,
1880 Connective tissue tumors
solitary, asymptomatic nodules or polyps ranging in size from 1 to 5 cm.1–3 Larger lesions rarely occur.4 Tumors also appear to be relatively common in the genital region and are very rare in the oral cavity and pharynx.5–15 Plantar lesions are exceptional.16,17 Three cases associated with pilomatricomas have been documented.18 Local recurrence is common and occurs in up to 25% of cases.
The myxomas described in the Carney complex are very similar, if not identical, to superficial angiomyxomas.2,3,7–19 This complex, described in 1985, is an autosomal dominant disorder associated with inactivating mutations in PRKAR1A which encodes a regulatory subunit of protein kinase A,20–23 consisting of myxomas, spotty pigmentation (lentigines on the face, especially the lips) and endocrine overactivity (Cushing syndrome, pituitary adenoma, and testicular tumors).20,24,25 Additional features of the complex include blue nevi and malignant melanotic schwannoma (previously known as psammomatous melanotic schwannoma). The myxomas can present in the skin, breast, and heart. Their recognition in the skin is important because they can be the first manifestation of the syndrome. They are usually multiple, present in young adults, and have a wide anatomical distribution, with a special preference for the eyelids, ears, and nipples.26,27
Histologic features Histologically, the lesions are dermal and subcutaneous, consisting of multiple, poorly circumscribed myxoid lobules containing bland spindle-shaped or stellate cells and abundant small blood vessels (Figs 35.647 and 35.648). Often, a sparse inflammatory cell infiltrate containing lymphocytes and neutrophils is also present. In about 30% of cases – either in the primary lesion or its recurrence – there is an epithelial component. The latter consists of epithelial strands, keratin cysts or nests of basaloid cells.1,2,28 It may mimic a follicular tumor such as a trichofolliculoma.29 In a single case of a vulvar tumor, necrotizing vasculitis was found within the lesion.30
Immunohistochemistry shows positivity of tumor cells for vimentin and variable focal positivity for CD34 and (less frequently) actin.
Differential diagnosis Nerve sheath myxoma is composed of discrete, well-defined nodules which contain S100 protein-positive cells. Low-grade myxofibrosarcoma is also a multilobular tumor but it is more deeply located and contains pleomorphic cells with mitotic activity. Superficial angiomyxoma hardly ever occurs in the fingers, and this, together with the presence of a more prominent vascular proliferation, more cellularity and a focal inflammatory cell infiltrate, allows distinction from a myxoid cyst.
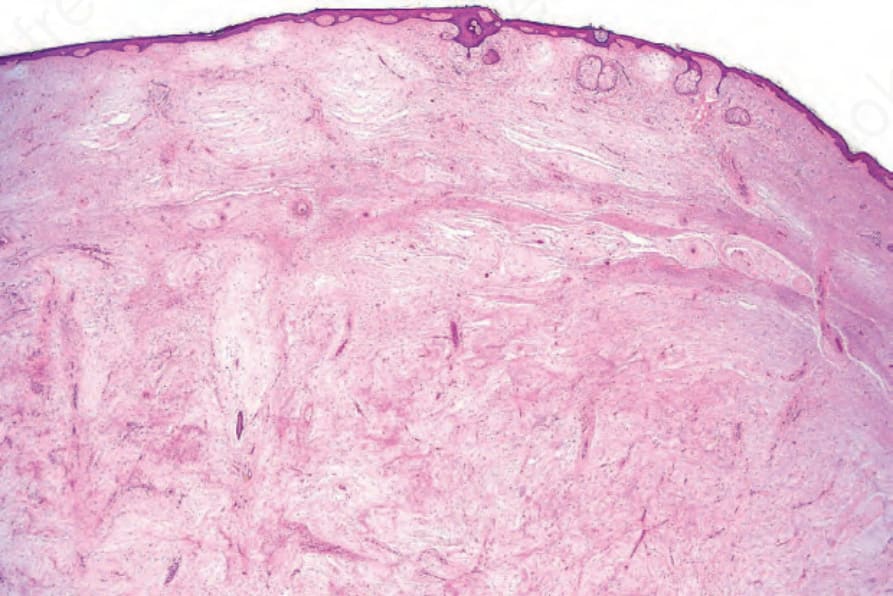
Fig. 35.647 Superficial angiomyxoma: there is massive myxoid change in the dermis associated with numerous small vessels.

Fig. 35.648 Superficial angiomyxoma: the myxoid deposits contain stellate cells and thinwalled vessels.