Extraskeletal myxoid chondrosarcoma
Extraskeletal myxoid chondrosarcoma
Clinical features Extraskeletal myxoid chondrosarcoma is an uncommon tumor that usually arises in adulthood, shows a slight predilection for males, and occurs most often in the limbs (particularly the legs); pediatric occurrence is rare.1–12 Although frequently of deep origin, up to 20% of cases arise subcutaneously. It presents as a slowly growing, usually painless, large mass. Unusual sites include the oral cavity and the vulva.8,13-18 Interestingly two cases reported in the vulva showed a PLAG1 gene activation suggesting a different molecular entity for tumors arising on the site.19 Cases on the foot mimicking planter fibromatosis or fibroma have been described 20,21 A spontaneous regression and a combined synovial sarcoma with extraskeletal myxoid chondrosarcoma have been documented.22,23
Lesions, which present as a slowly growing mass usually less than 3 cm in diameter, sometimes show calcification on radiological examination. Giant lesions are rarely seen.21–23
Up to 10% of cases recur locally after excision, but malignant change has never been reported. Bilateral chondromas have been reported, one of them occurring in association with chronic renal failure.24,25
Histologic features 12q 13-15 rearrangements resulting in expression of HMGA2 gene have been documented, as well as monosomy 5 and trisomy 6.26,27
The tumor, which may be intradermal or subcutaneous, is composed of a well-circumscribed, lobulated mass of mature hyaline cartilage (Figs 35.635 and 35.636). Dystrophic or degenerative features – such as myxoid change, hemorrhage, calcification, or ossification – are commonly seen, particularly
Although it was formerly believed that only 10–15% of cases recur or metastasize, it appears that most patients die of metastatic disease after long follow-up of 10–20 years.3,4 However, in a recent study the overall 5-, 10-, and 15-year survival rates were 82%, 65%, and 58%, respectively, after combined treatment with surgery and chemotherapy.24 Radiation therapy may be beneficial especially in localized cases.6
1877 Malignant tumors of cartilage
more central portion of each tumor lobule comprises a loose myxoid stroma within which are ovoid to spindle-shaped cells arranged in interlacing cords and strands (Fig. 35.639). Occasional cases show obvious chondroblastic differentiation. Mitotic figures tend to be sparse. Infrequently, there are foci of metaplastic bone formation, most often at the periphery of the lesion, and rare cases exhibit intracytoplasmic eosinophilic (rhabdoid) inclusions.
Tumor cells usually have abundant intracytoplasmic glycogen, and up to 20% of cases are positive for S100 protein; SOX 10 may also be positive.48–50 Rarely, there may be focal positivity for EMA and keratin.49
Differential diagnosis The most important differential diagnosis includes myxoid liposarcoma and malignant mixed tumors. The former has a distinctive branching vascular pattern and lipoblasts are evident, whereas the latter tumor shows epithelial elements with ductal differentiation and, often, more differentiated cartilage. In addition, it expresses keratin and actin.
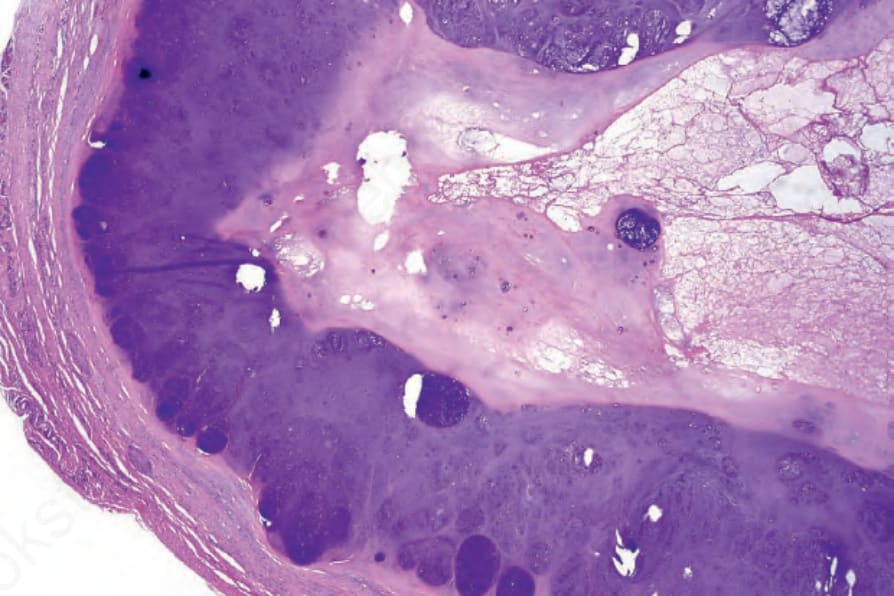
Fig. 35.635 Soft tissue chondroma: the tumor is encapsulated and composed of well-defined lobules of mature cartilage.
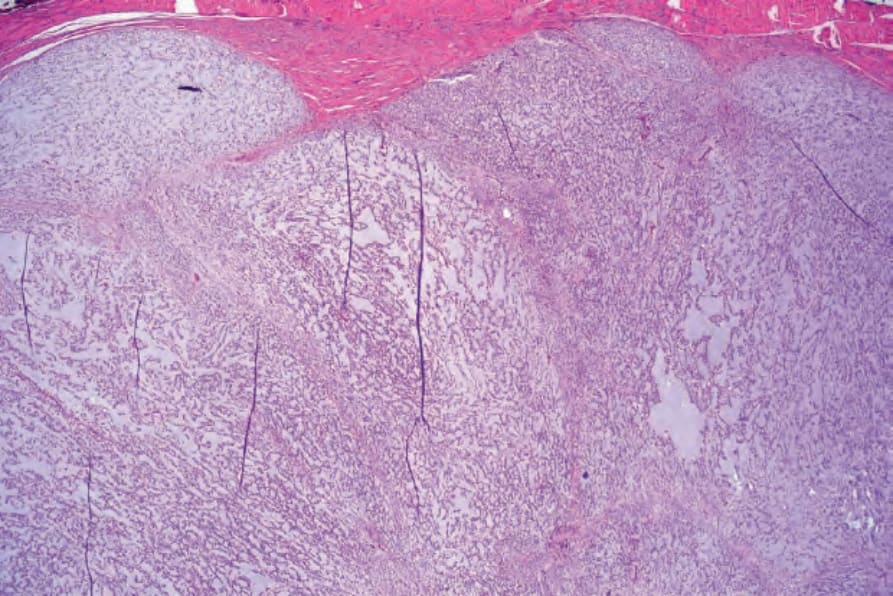
Fig. 35.637 Extraskeletal myxoid chondrosarcoma: the tumor is lobulated and shows a biphasic population. Small hyperchromatic cells at the periphery merge with a central myxoid component.
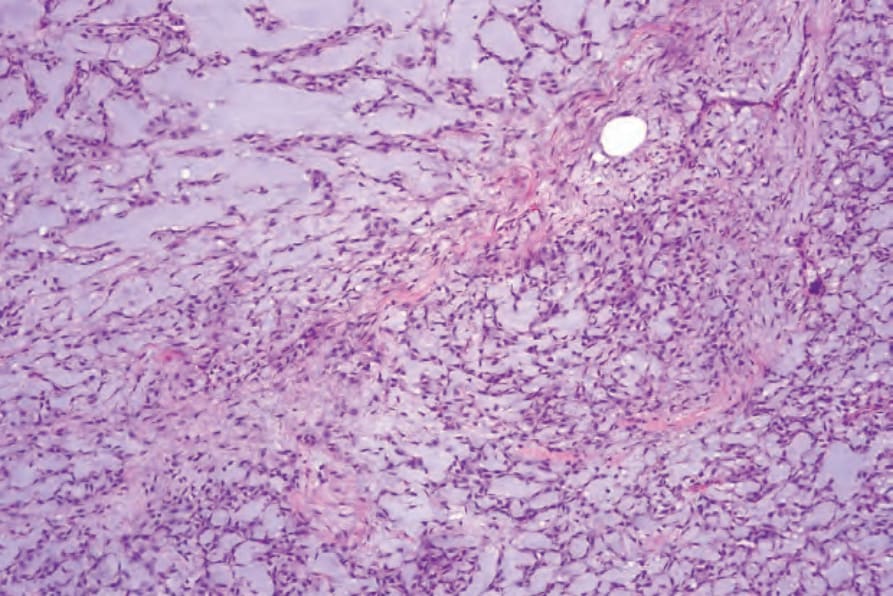
Fig. 35.638 Extraskeletal myxoid chondrosarcoma: medium-power view.
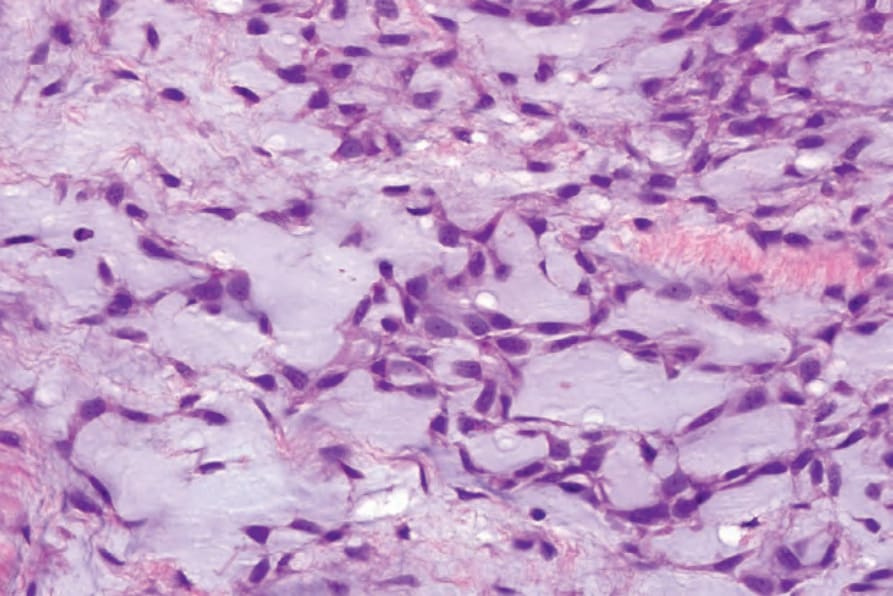
Fig. 35.639 Extraskeletal myxoid chondrosarcoma: the tumor cells are pleomorphic and hyperchromatic.