Angioleiomyoma
Angioleiomyoma
Clinical features Angioleiomyomas are common, deep dermal or subcutaneous, benign, smooth muscle tumors that originate from vascular smooth muscle. They are currently classified as tumors of pericytic lineage.1 They arise most often in adults between 30 and 60 years of age, particularly on the limbs (especially the lower legs).2–5 Females are affected at least twice as often as males, except in the head and neck regions where the ratio is reversed.6 Congenital tumors have been described.7 Rare cases of digital (and subungual) angioleiomyoma have been documented, one with bone destruction.8–11 Involvement of the palm is exceptional.12 Tumors occurring on the cheek, nasal tip and the auricle as well as a case on the scalp mimicking a dermoid cyst have been reported.12–16 Lesions can rarely occur in the oral cavity.17–19 Tumors are typically solitary, slowly growing lesions less than 2 cm in diameter, and may be painful or tender when compressed (Fig. 35.628). Recurrence after simple excision is very rare and malignant change has never been convincingly documented. An association with multiple pilar leiomyomas is extremely rare.20 In an HIV-positive patient, multiple lesions developed and EBV was demonstrated by in situ hybridization within the nuclei of the tumor cells; these likely represent cases of EBV-associated smooth muscle tumors.21–23
Pathogenesis and histologic features Cytogenetic studies vary and have revealed chromosomal imbalances and a few nonrecurring translocations, with the most consistent loss being found in chromosome 22.24–26
Histologically, in contrast to pilar leiomyoma, these are rounded, encapsulated lesions. They are composed of interlacing bundles of uniform
1874 Connective tissue tumors
smooth muscle cells, distributed around numerous small vessels with walls of variable thickness (Figs 35.629 and 35.630). Hyaline or myxoid degeneration, thrombosis and dystrophic calcification are frequently encountered.27 Calcification can be very prominent and seems to be more common in acral lesions.28–31 Some cases contain collections of mature adipocytes (angiomyolipoma, angiolipoleiomyoma) and, although they probably represent metaplastic change, it has been proposed that such variants are hamartomatous.32–36 Such tumors are negative for HMB-45 and are not associated with tuberous sclerosis.37 In a small proportion of cases, the vascular spaces may show marked, almost sinusoidal, dilatation. Occasionally, scattered cells with enlarged hyperchromatic nuclei are seen.38–41 This
change is not associated with increased mitotic activity, does not indicate malignancy and is probably secondary to degeneration. Unusual findings in angioleiomyoma include epithelioid cell change, clear cell change, and prominent palisading mimicking Verocay bodies.42–44 A case reported as intravascular angioleiomyoma overlaps with a myopericytoma giving support to the accepted proposal of the former having been part of the spectrum of tumors of perivascular cells.1,45,46 However, tumor cells in myopericytoma are positive for actin and usually negative for desmin.
Immunohistochemical findings are identical to those for pilar leiomyoma and consist of diffuse staining of tumor cells for SMA, calponin, desmin and h-caldesmon.47 Myosin 1B, a newly identified human pericyte marker, is negative.48
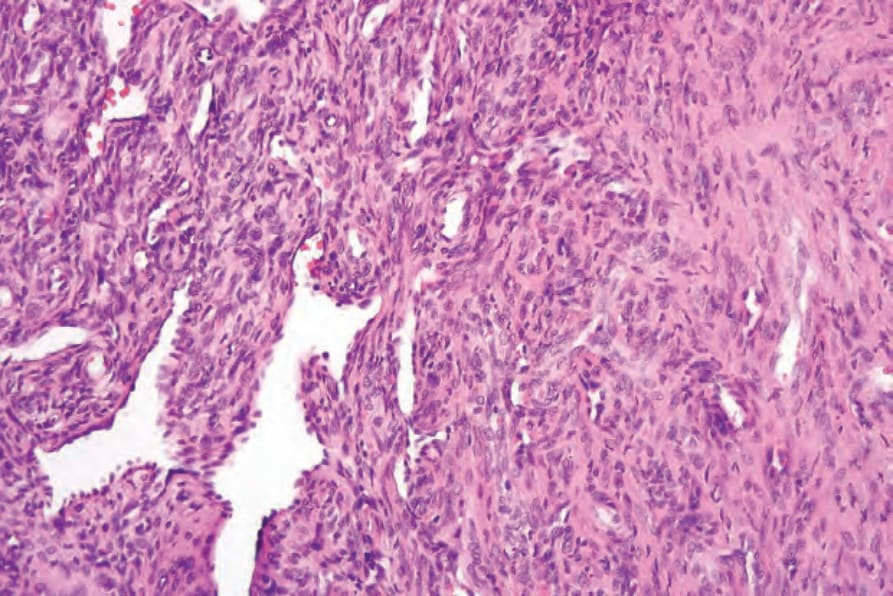
Fig. 35.627 Myofibroma: high-power view.

Fig. 35.628 Angioleiomyoma: lesions are very rarely superficial, as in this example which presented as a vascular papule. By courtesy of the Institute of Dermatology, London, UK.
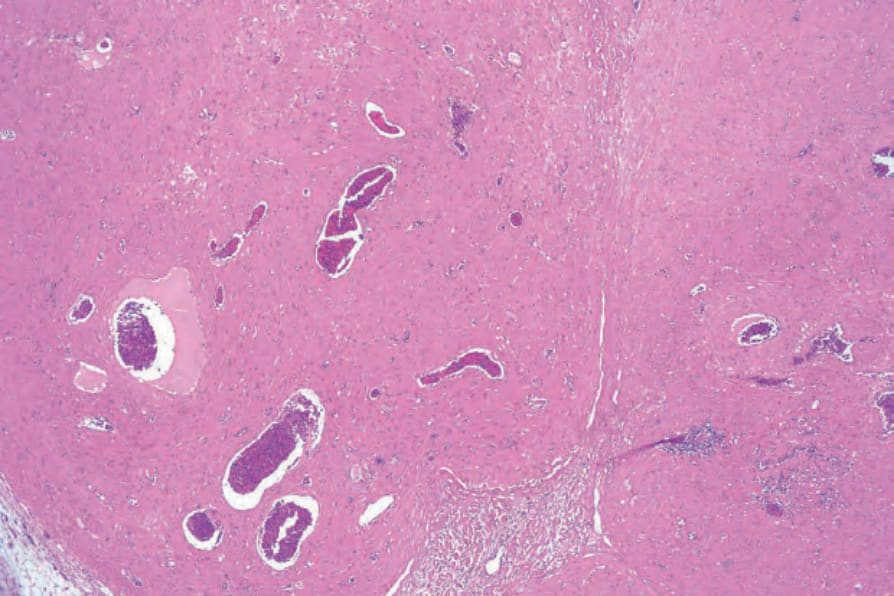
Fig. 35.629 Angioleiomyoma: the tumor is well circumscribed and shows an admixture of bundles of smooth muscle cells surrounding thick-walled blood vessels.
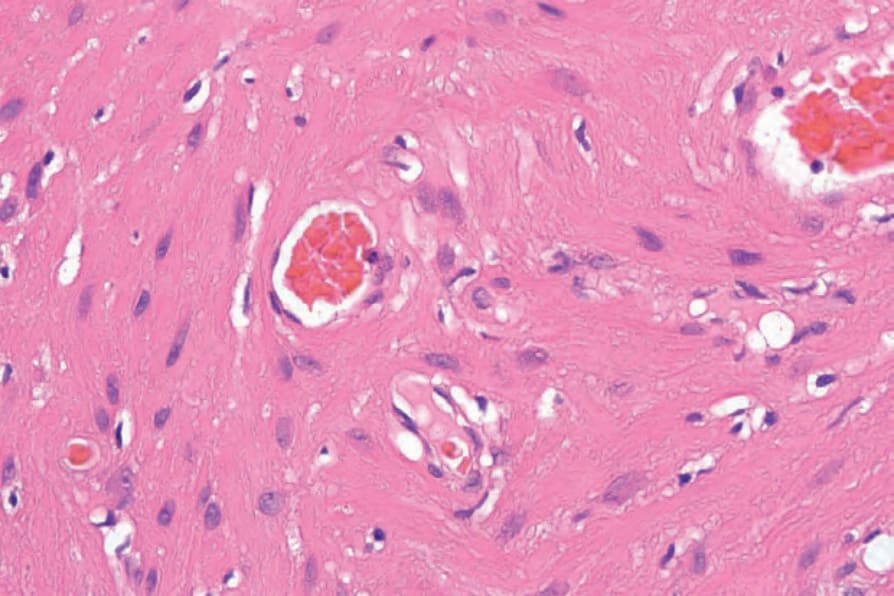
Fig. 35.630 Angioleiomyoma: high-power view.