Myofibroma and myofibromatosis
Myofibroma and myofibromatosis
Clinical features Solitary and multicentric myofibromas are relatively rare tumors with marked predilection for children.1–8 Myofibroma forms part of the spectrum of myopericytoma.9,10 Myofibroma, myofibromatosis, and angioleiomyoma along glomus tumor and myopericytoma are currently classified as tumors of perivascular cells.11 The majority of tumors present before the age of 2 years and many of these are congenital. It appears as a usually solitary
dermal, subcutaneous, intramuscular nodule or rarely intraosseous tumor, and is more frequently seen in males.12,13 In the solitary form, the head and neck (including the oral cavity and rarely the pharynx) are most often involved, followed by the trunk and extremities.1–8,14–17 A lesion involving the sclera has been documented.18 Individual lesions are firm or rubbery, somewhat nodular, and rarely exceed 3–4 cm in diameter. Although most tumors are single, multiple lesions may occur in children and occasionally in adults.19,20 Multicentric tumors in children have also been referred to as congenital generalized fibromatosis and infantile myofibromatosis (Fig. 35.620).4–8,21–23, In these cases, patients are more often female and are found to have multiple soft tissue lesions with associated bony, oral or (rarely) visceral tumors of a similar nature.24 Organs involved include the kidney, lung, pancreas, gastrointestinal tract, liver and rarely the central nervous system.1,25–27
A few cases appear to be inherited, most often in an autosomal dominant pattern.5,28–30 A single case associated with porencephaly, hemiatrophy and
1872 Connective tissue tumors
cutis marmorata telangiectatica congenita has been documented.32 A case associated with thrombocytopenia has been reported.33
Myofibroma in adults is almost always solitary and superficial, only exceptionally presenting as multiple lesions. A patient with multiple acral lesions had generalized morphea.34 Usually, they affect the skin or oral mucosa, and no familial cases have been reported. Most patients are young to middle-aged adults of either sex who present with a firm superficial nodule up to 3 cm in diameter.1–3 Lesions may be painful. Local recurrence is very rare.35
Solitary soft tissue or associated bony lesions may recur locally if excised; however, if these lesions are left untreated, spontaneous regression is very common. In contrast, if there is visceral involvement the course is often fatal, being associated with progressive impairment of respiratory or gastrointestinal function.
Pathogenesis and histologic features Recurrent PDGFRB alterations have been documented, similar to those seen in myopericytoma, supporting a close pathogenetic link between the entities.36,37
Lesions tend to be reasonably well circumscribed, but unencapsulated. A distinctive biphasic pattern is commonly produced by the presence of varying proportions of two populations of cells. These comprise:
• fascicles of bland eosinophilic myofibroblasts with tapering or vesicular nuclei,
• more primitive, smaller, round and spindle-shaped cells with scanty cytoplasm and round or oval nuclei (Figs 35.621–35.624). The latter cells tend to be arranged around branching blood vessels in a hemangiopericytomatous pattern (Fig. 35.625). Small foci of necrosis and vascular invasion are often present. Mitotic figures may be readily found, but are never abnormal. Tumor cells in both components are usually focally smooth muscle actin positive.6 Calponin tends to be more diffusely positive and h-caldesmon is focally positive.38 CD34 positivity has been reported.39
In some cases, especially those with multicentric disease, the primitive areas with a hemangiopericytoma-like pattern predominate. These lesions are almost identical clinically and histologically to tumors classified in the past as infantile hemangiopericytoma and it has been proposed that the latter belong to the spectrum of infantile myofibromatosis.40
The histologic features of myofibroma are identical to those of infantile myofibromatosis, but the more primitive hemangiopericytomatous component is often not prominent and can be almost absent (Figs 35.626 and 35.627). The myofibroblastic nodules may undergo hyalinization with a pseudochondroid appearance. Some tumor nodules appear to be in intravascular locations but this mainly represents subendothelial growth. This is seen in up to 30% of cases.1 Tumor cells are positive for muscle actin.
1873 Tumors of perivascular cells
Differential diagnosis The presence of a biphasic pattern allows distinction from cutaneous smooth muscle tumors, which are also consistently actin and desmin positive, and from fibrous histiocytoma, which is more polymorphic and less well circumscribed.

Fig. 35.620 Infantile myofibromatosis: multiple large tumor nodules are present. By courtesy of the Institute of Dermatology, London, UK.
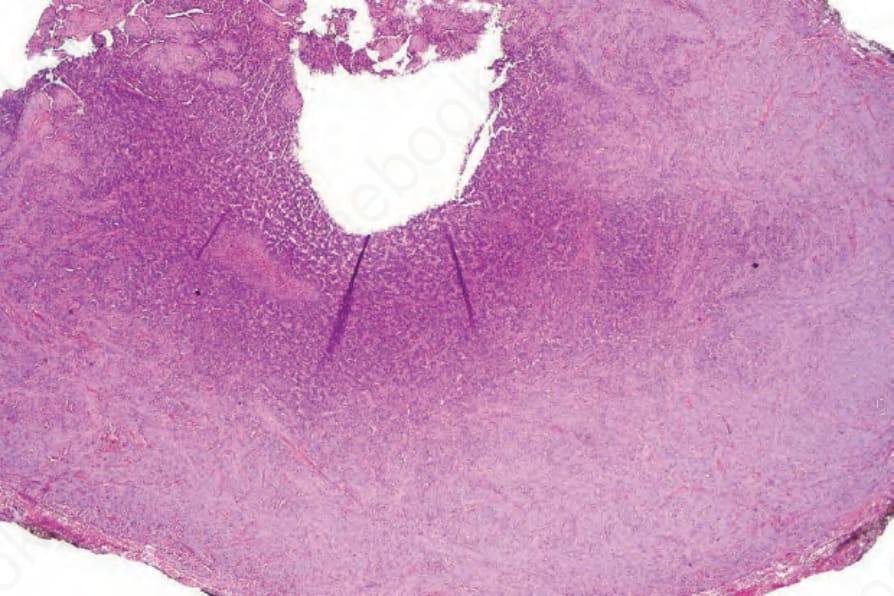
Fig. 35.621 Infantile myofibromatosis: scanning view of a circumscribed tumor showing a hemangiopericytomatous central component.
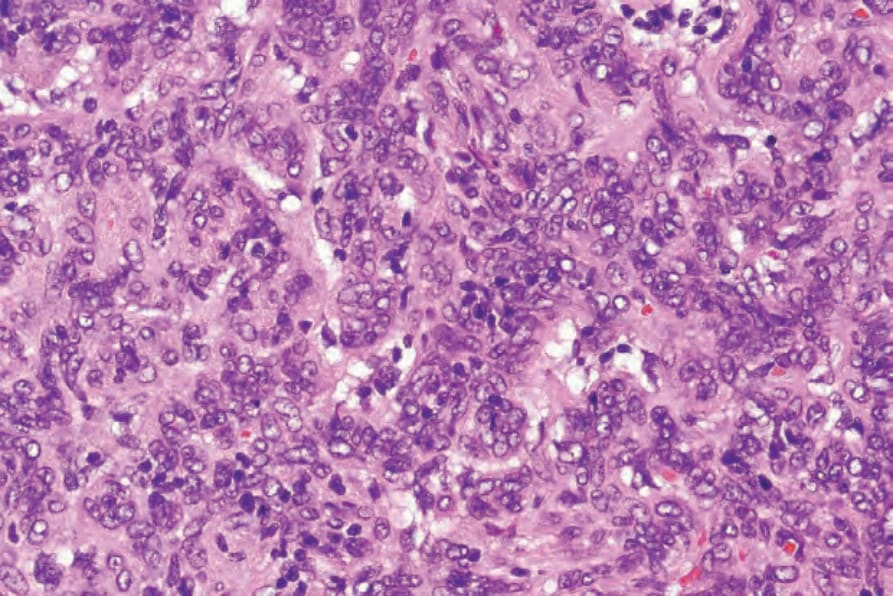
Fig. 35.622 Infantile myofibromatosis: high-power view showing primitive cells with basophilic vesicular nuclei.
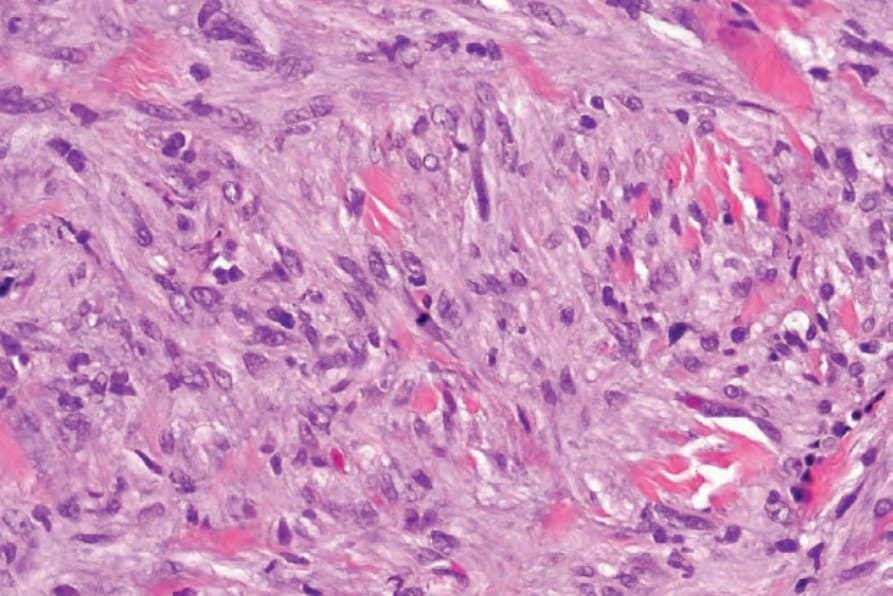
Fig. 35.623 Infantile myofibromatosis: this field highlights the myofibroblastic component.
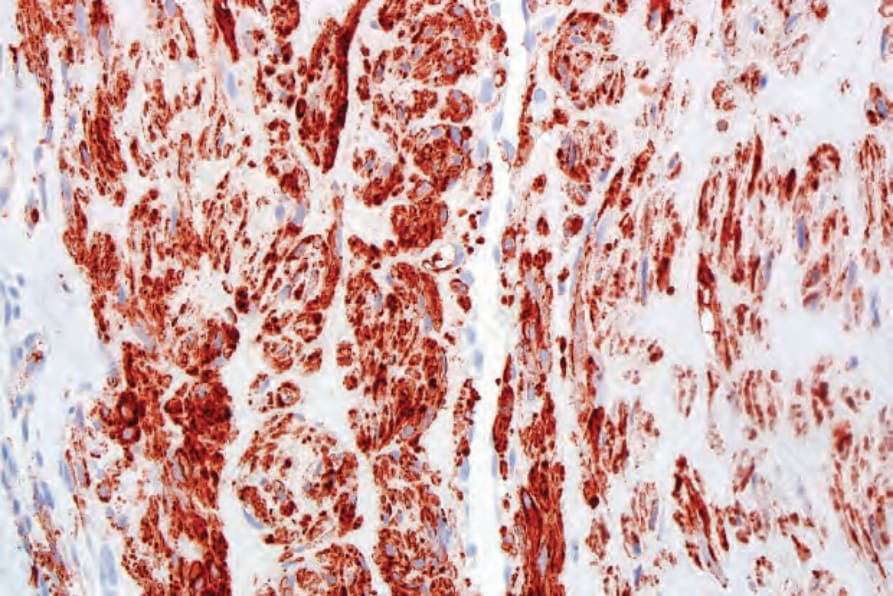
Fig. 35.624 Infantile myofibromatosis: the tumor cells express smooth muscle actin.
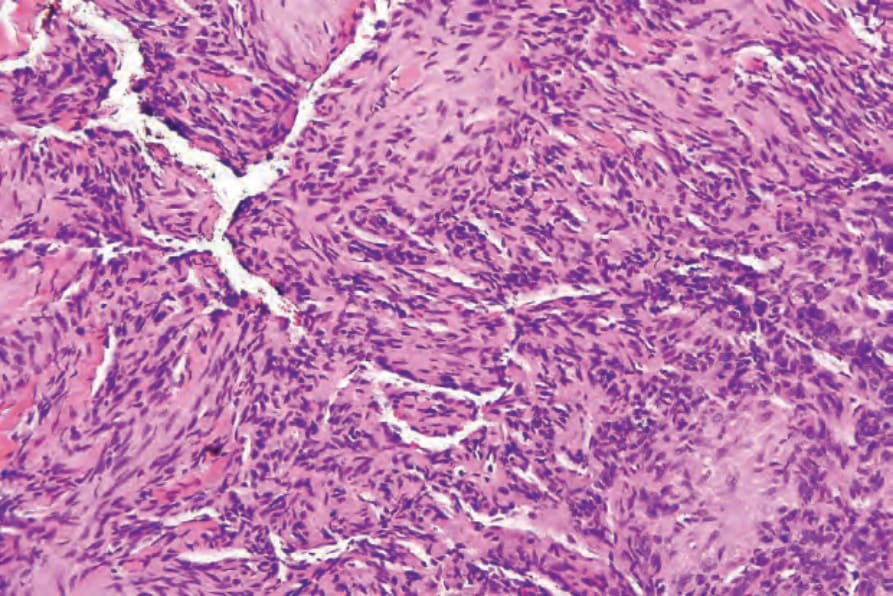
Fig. 35.625 Infantile myofibromatosis: high-power view of the center of the lesion shown in Fig. 35.102, highlighting the hemangiopericytomatous vascular network.
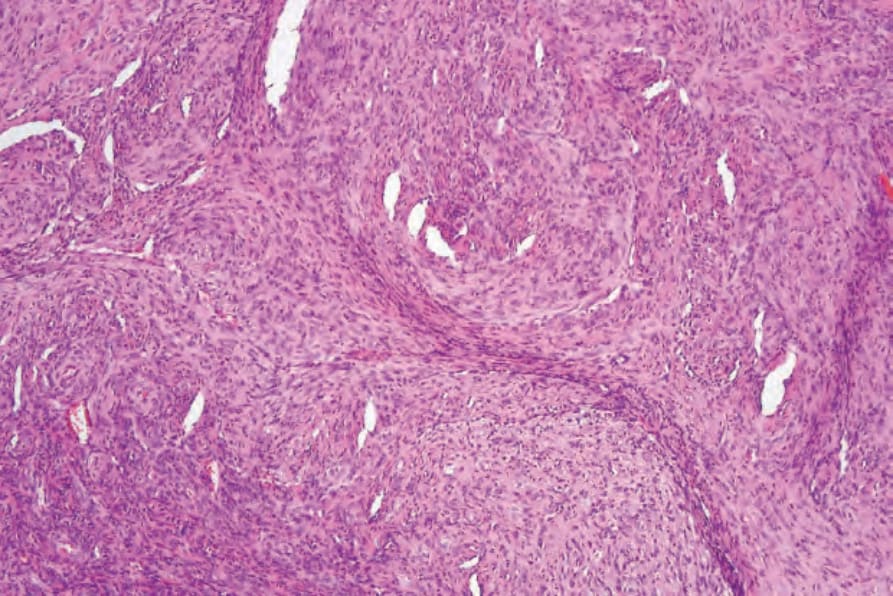
Fig. 35.626 Myofibroma: low-power view of a dermal nodule. Even at this magnification, the biphasic nature of the tumor is apparent.

Fig. 35.628 Angioleiomyoma: lesions are very rarely superficial, as in this example which presented as a vascular papule. By courtesy of the Institute of Dermatology, London, UK.