Myopericytoma
Myopericytoma
asymptomatic, and may be single or (less frequently) multiple. Rarely, tumors are painful. Recurrence is rare and frequently represents either persistence or the development of a new tumor. Very rare malignant examples of myopericytoma have been described; these appear to have an aggressive clinical behavior.8,15
An association with HIV/AIDS has been reported and in this setting tumor tend to occur at sites other than soft tissue and skin (including bronchus, larynx, tongue, liver, and brain), are often multiple, and are associated with Epstein-Barr virus.16,17 Two exceptional cases of glomangiopericytoma associated with oncogenic osteomalacia have been documented.18,19 In two cases, trauma was suggested as a possible factor in the development of the tumors.20
Pathogenesis and histologic features Recurrent PDGFRB alterations have been documented, similar to those seen in infantile myofibromatosis/myofibroma, supporting a close pathogenetic link between the entities.21,22 A small number of myopericytomas show BRAF(V600E) mutations and anti-BRAF(V600E) agents have been suggested as a treatment for multifocal, infiltrative and recurrent tumor bearing this mutation.23
Traditionally, tumors thought to differentiate towards perivascular myoid cells or pericytes have been divided into two main groups: infantile hemangiopericytoma and adult hemangiopericytoma.1,2 Both variants, however, appear to have very little in common except for the histologic presence of a pericytomatous vascular pattern. Moreover, with the combination of immunohistochemistry and electron microscopy, most tumors classified as adult hemangiopericytoma on light microscopy show other lines of differentiation including synovial sarcoma, mesenchymal chondrosarcoma, and solitary fibrous tumor.3 The handful of cases in which the line of differentiation remains obscure are the ‘true’ adult hemangiopericytomas, but it is likely that they arise from an undifferentiated mesenchymal cell. These rare examples of ‘true’ adult hemangiopericytomas do not usually occur in the skin and will not be discussed further in this chapter.
Tumors are dermal, dermal and subcutaneous, or purely subcutaneous and rarely arise in deeper soft tissues.8 The histologic spectrum of myopericytoma is very wide and varies from lesions that are very similar to myofibromatosis to those that closely resemble glomus tumors and even an angioleiomyoma (Figs 35.616 and 35.617). They are well circumscribed and are composed of a mixture of solid cellular areas intermixed with variable numbers of vascular channels. The latter are often elongated and display prominent branching, resulting in a stag-horn appearance (hemangiopericytoma-like). The cells in the solid areas are round or short and spindle-shaped with eosinophilic or amphophilic cytoplasm and vesicular nuclei. Cytologic atypia is not usually a feature and mitotic figures are very rare. A common and striking feature is the presence of concentric layers of tumor cells around vascular channels, resulting in a typical ‘onion-ring’ appearance (Fig. 35.618). Myxoid change may be focally prominent. Occasional findings include hyalinization/sclerosis, cystic degeneration and bone formation. Rare examples are entirely intravascular (within a vein or an artery).8,24–28 In some cases, tumor cells closely resemble glomus cells and are characterized by round, punched-out central nuclei and pale eosinophilic cytoplasm. These cases are referred to as glomangiopericytomas. Myopericytomatosis refers to a rare subset of tumors characterized by diffuse involvement of the dermis and subcutaneous tissue by nodules of pericytic cells.21
The concept of myopericytoma was introduced to describe a spectrum of tumors composed of short oval to spindle-shaped cells with a myoid appearance and a distinctive concentric perivascular growth.4 These tumors tend to occur mainly in the deep dermis and subcutaneous tissue and include lesions classified in the past as glomangiopericytoma, myopericytoma, myofibroma and myofibromatosis in adults. Infantile hemangiopericytoma and infantile myofibromatosis also represent part of the spectrum of tumors with true pericytic differentiation.5–8
Clinical features Myopericytoma most commonly occurs in middle-aged adults (mainly in the fifth decade) with a predilection for the limbs, particularly the distal lower limb followed by the head and neck (including the oral cavity).9 Exceptional tumors may occur in the kidney, lung, parotid gland, within the cranium, or in the thoracic spine.10–14 Males are more frequently affected than females. Lesions are small (less than 2 cm in diameter), long-standing, usually
Tumors regarded as malignant display cytologic atypia and increased mitotic activity.8,15
1871 Tumors of perivascular cells
Myopericytoma cells stain diffusely for SMA and calponin, are often positive for h-caldesmon and only very rarely focally positive for desmin (Fig. 35.619).8 Focal staining for CD34 may also be seen.
Differential diagnosis Most authors regard angioleiomyoma as part of the spectrum of myopericytoma.29 The coexistence of both tumors in the same patient and a number of morphological features support this theory. Angioleiomyoma, however, is composed of uniform smooth muscle cells, which stain diffusely for both SMA and desmin. Furthermore, concentric arrangement of tumor cells around vascular channels is less prominent than that seen in myopericytoma.
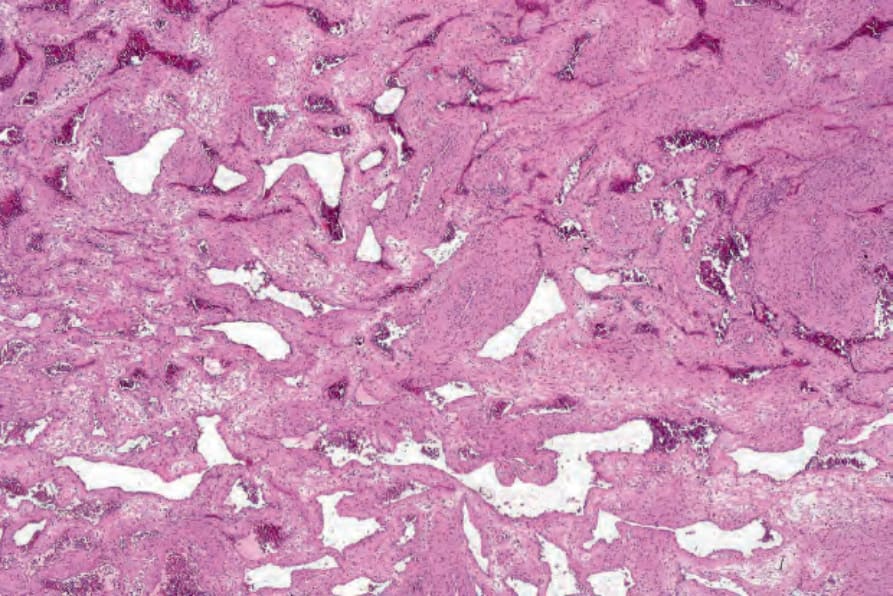
Fig. 35.616 Myopericytoma: low-power view showing dilated vessels and abundant smooth muscle.
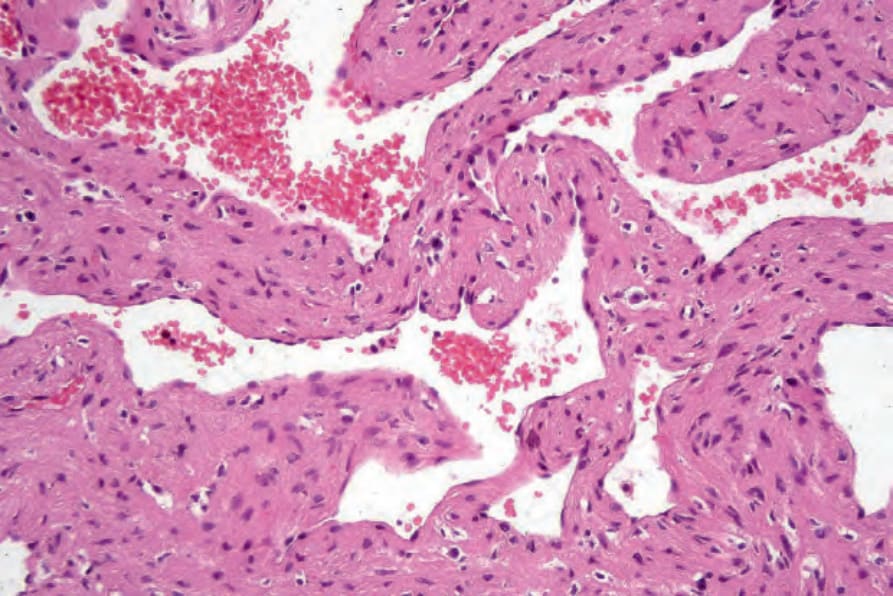
Fig. 35.617 Myopericytoma: high-power view.
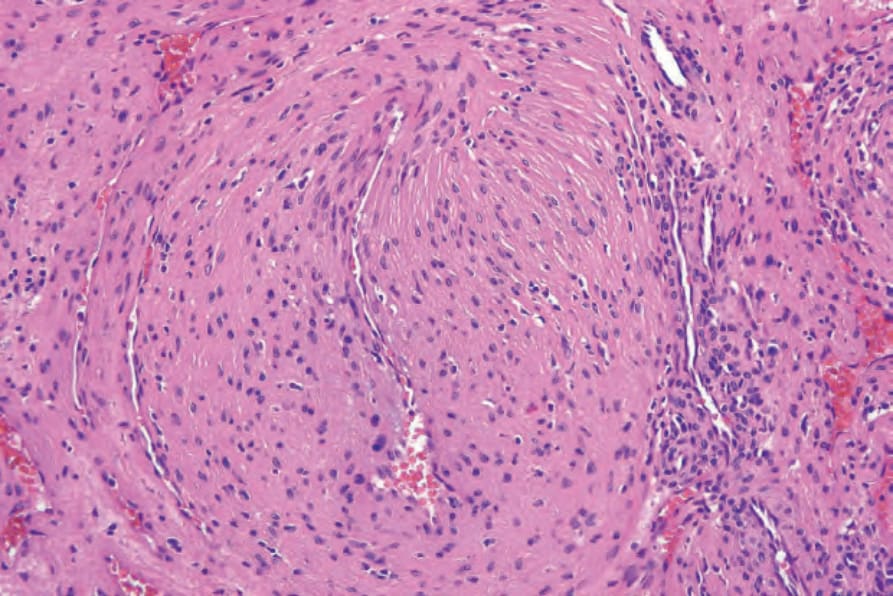
Fig. 35.618 Myopericytoma: this perivascular distribution of tumor cells in an onion ring-like appearance is characteristic.
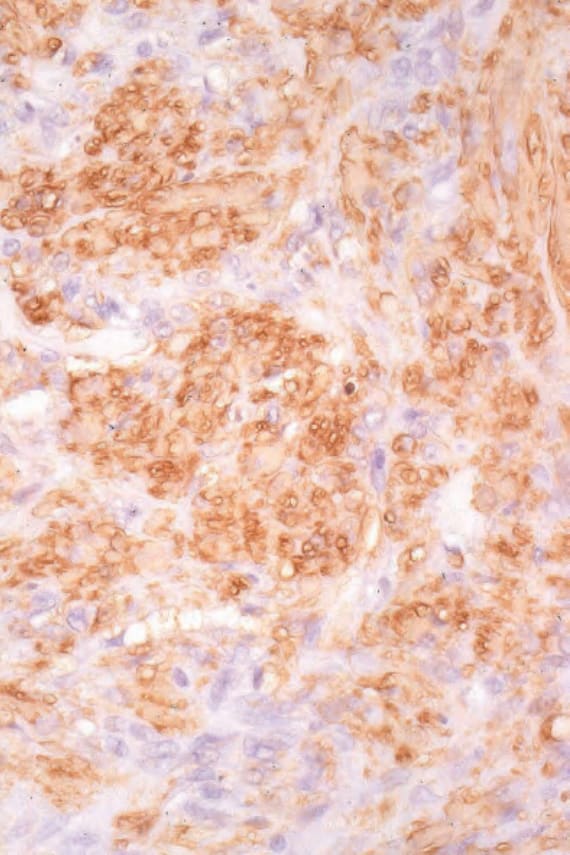
Fig. 35.619 Myopericytoma: the tumor cells express smooth muscle actin.

Fig. 35.620 Infantile myofibromatosis: multiple large tumor nodules are present. By courtesy of the Institute of Dermatology, London, UK.