Lymphangiomatosis
Lymphangiomatosis
Clinical features Lymphangiomatosis (generalized lymphatic anomaly) is a congenital abnormality characterized by diffuse involvement of soft tissues, skin, bone, lymph nodes and (often) parenchymal organs.1–4 The disease can be localized to the thorax or abdomen, with predilection for some organs including the kidney and spleen.5–9 Involvement of the colon can result in protein-losing enteropathy.10 Multifocal lymphangiomatosis has been described in association with protein-losing enteropathy in patients after palliation of complex congenital heart disease with total cavopulmonary connection.11 An exceptional association with disseminated intravascular coagulation has been reported.12 Extensive involvement may be associated with mortality.13 Most cases present in children and there is no sex predilection. In rare cases, the disease affects only a limb, with or without concomitant bone involvement.2,14 Coexistence with a cystic hygroma is exceptional.15 Overlap with angiomatosis can occur and accurate diagnosis requires lymphangiography. Rare cases are associated with kaposiform hemangioendothelioma.16 Gorham-Stout syndrome refers to the proliferation of lymphatic and vascular channels associated with prominent osteolytic lesions.17 It has been suggested that this disease is mediated by monocytes that secrete cytokines, inducing angiogenesis and proliferation of osteoclasts.18 A case of acquired lymphangiomatosis in an HIV positive patient has been reported.19
Pathogenesis and histologic features A somatic mutation in NRAS has been reported in lymphangiomatosis.20
Histologically, lesions resemble a benign lymphangioendothelioma except that there is very extensive diffuse dissection of dermal structures (the ‘hair-dryer effect’) (Figs 35.604 and 35.605).2 Long-standing lesions may show stromal sclerosis, and extramedullary hemopoiesis is evident in some cases.
The endothelial cells lining the vascular channels in lymphangiomatosis display increased expression of epidermal growth-factor receptor suggesting that this may be used therapeutically.21
particularly the fingers, and especially the subungual region. Lesions can, however, occur with a wide anatomic distribution, not only in the skin but also rarely in mucosae (including oral cavity) and internal organs.4 The latter include the esophagus, stomach, lung, trachea, bone, small bowel, colon, rectum, mesentery, pterygoid fossa, mediastinum, liver, pancreas, vagina, cervix, ovary and kidney.5–23 A glomus tumor arising in an ovarian teratoma has been documented.24 Typically, the tumors are small (less than 1 cm in diameter), reddish-blue nodules and classically present with paroxysmal severe pain, which is often precipitated by cold, pressure or dependency. Pain appears to be more frequent in histologically solid tumors in contrast to the more common glomangiomas.
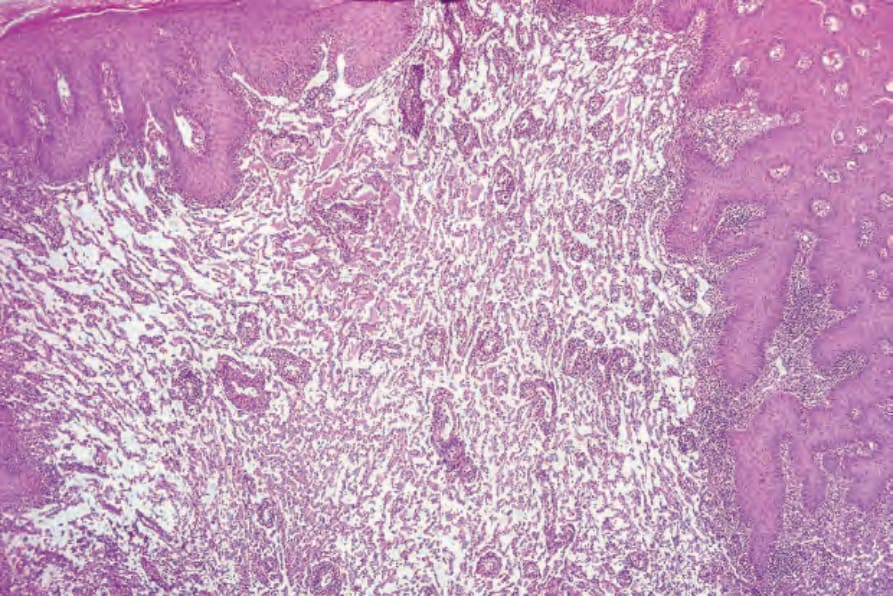
Fig. 35.604 Lymphangiomatosis: this condition shows massive dissection of the dermal collagen and is always clinically extensive.
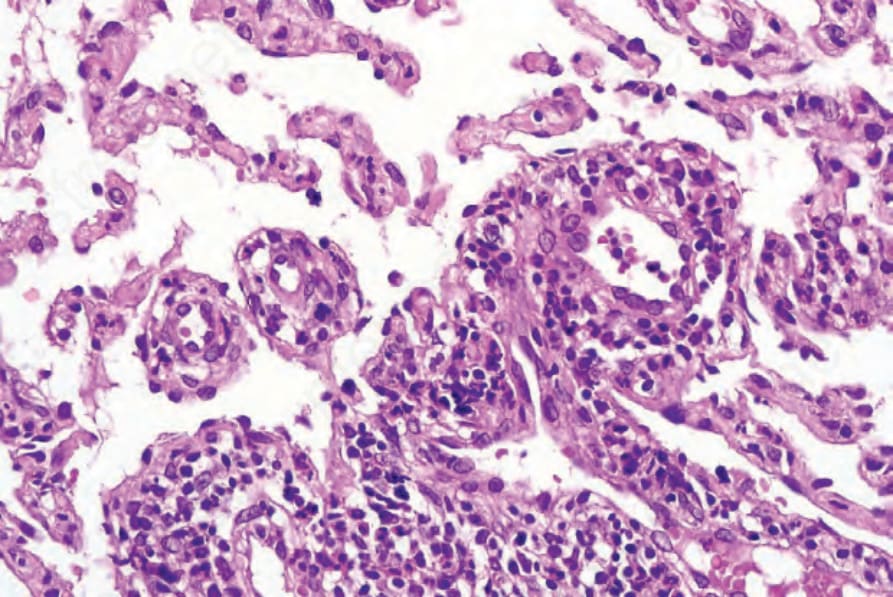
Fig. 35.605 Lymphangiomatosis: high-power view.