Lymphangioma
Lymphangioma
Lymphangiomas take four principal forms:
• cavernous lymphangioma,
• cystic hygroma,
• lymphangioma circumscriptum,
• acquired progressive lymphangioma (benign lymphangioendothelioma). The existence of a true capillary lymphangioma is highly questionable.
1864 Connective tissue tumors
Clinical features Cavernous lymphangioma Cavernous lymphangioma is a congenital or infantile lesion of equal sex incidence that arises most often in the head and neck region (particularly the tongue) and extremities.1–5 It presents as a large diffuse, rather doughy mass and is very prone to local recurrence after simple excision. Rare cases present for the first time in adults. Coexistence with a lymphangioma circumscriptum is very rare.6
Cystic hygroma Cystic hygroma is also a lesion of infancy, and presents as a large cystic mass, most often in the neck, axillae or inguinal region.1,2,5 Scrotal lesions have also been reported.7 Intra-abdominal and intrathoracic lesions also occur.8,9 It is also prone to local recurrence unless widely excised, although this tendency is much less marked than with cavernous tumors. Coexistence with a port-wine stain is exceptional.10 Lesions have been reported in adults.11. Cystic hygromas have been associated with trisomy 21, 13, and 18, and Turner and Noonan syndrome.12
limbs, although the anatomical distribution is wide. It presents as a solitary, well-defined erythematous macule or plaque that gradually increases in size. Simple excision is usually curative, with only exceptional local recurrences.22 Occasional partial spontaneous regression is rarely seen. A case has been documented after radiotherapy, a further case developed following femoral arteriography and one has been reported in an HIV-positive patient.23–25
Pathogenesis and histologic features Recently, a number of lymphatic tumors presenting in isolation or as part of complex vascular malformations have been shown display somatic mutations in PIK3CA.26
Cavernous lymphangioma is typically an ill-defined lesion in the dermis or subcutaneous fat, composed of numerous dilated lymphatic channels without endothelial atypia (Fig. 35.596). The surrounding stroma may be inconspicuous or composed of prominent adventitial-type reticulin fibers with a chronic inflammatory cell infiltrate.
Lymphangioma circumscriptum Lymphangioma circumscriptum also presents most often in infancy, but may arise at any age and shows an equal sex distribution.3–5 Although it develops at any cutaneous site, the proximal portions of the limbs and limb girdles are usually affected. The lesion occurs as a localized collection of numerous small vesicles or blebs which may sometimes form larger confluent masses, filled with clear fluid or blood (Fig. 35.595). Occasionally, solitary lesions are present. They are typically asymptomatic unless irritated by the patient.
Cystic hygroma is histologically almost indistinguishable from the cavernous lesions except that its thin-walled lymphatic spaces show gross cystic dilatation. As well as a lymphocytic infiltrate, scattered lymphoid follicles are common.
In both lesions, the vascular lumina often contain proteinaceous, pale, eosinophilic lymph, and the vessel walls may contain an incomplete layer of smooth muscle.
Lymphangioma circumscriptum is usually situated in the superficial dermis. It is composed of multiple dilated lymphatic channels which often have fairly thick walls and commonly appear to extend into the overlying epidermis (Fig. 35.597). The latter is frequently acanthotic and a stromal lymphocytic infiltrate is sometimes evident. Cavernous spaces may be seen in the deeper dermis and occasionally a muscular lymphatic channel (often regarded as the feeding vessel) is present (Fig. 35.598).
Although the majority of these tumors probably represent developmental malformations, a small proportion are acquired, usually following block dissection of regional lymph nodes or radiotherapy.13 Similarly, a small number of cases are associated with an underlying cavernous or cystic lymphangioma. Vulval lesions are idiopathic or have been associated with Crohn disease and radiation therapy.14 Rare vulvar lesions associated with malignancy and hidradenitis suppurativa have been described.15 Recurrence after excision is quite common.
Acquired progressive lymphangioma (Benign Lymphangioendothelioma) Acquired progressive lymphangioma is a rare tumor that was originally described as more frequently seen in children.16–22 However, the more recent literature suggests that it is more common in adults.22 It has an equal sex incidence and particularly involves the extremities, especially the upper
In progressive lymphangioma, involvement of the superficial dermis is usually prominent, but extension into the deep dermis and superficial subcutis is not uncommon (Fig. 35.599). Horizontal, irregular, thin-walled vascular channels lined by a single layer of flat attenuated endothelial cells are seen dissecting the collagen bundles (Fig. 35.600). The channels appear empty but occasionally proteinaceous material or red blood cells are seen. Focal papillary projections are sometimes present. Some vascular spaces may have a layer of smooth muscle. Stromal inflammation is not a feature.
Differential diagnosis Progressive lymphangioma may mimic low-grade angiosarcoma and patch-stage Kaposi sarcoma. The former has at least focal cytologic atypia and multilayering and the clinical setting is different. In the latter there are
1865 Malignant vascular tumors
usually multiple lesions and histologically there is hemosiderin deposition with extravasated erythrocytes and adjacent inflammatory cells, including plasma cells. Distinction from lymphangiomatosis is afforded mainly by the clinical extent of the lesion.

Fig. 35.595 Lymphangioma circumscriptum: the lesion presents as variable numbers of superficial fluid-filled blebs. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
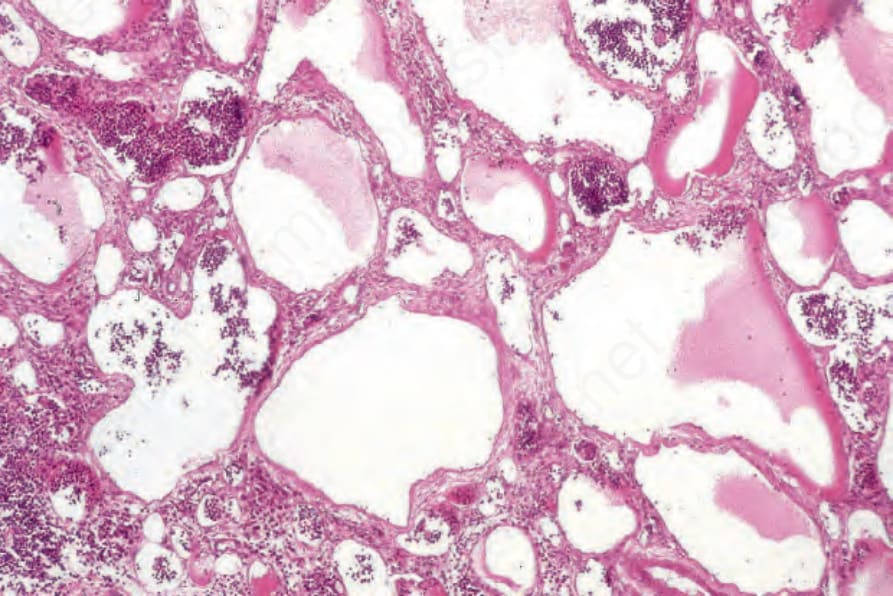
Fig. 35.596 Cavernous lymphangioma: widely dilated lymph-filled channels are characteristic.
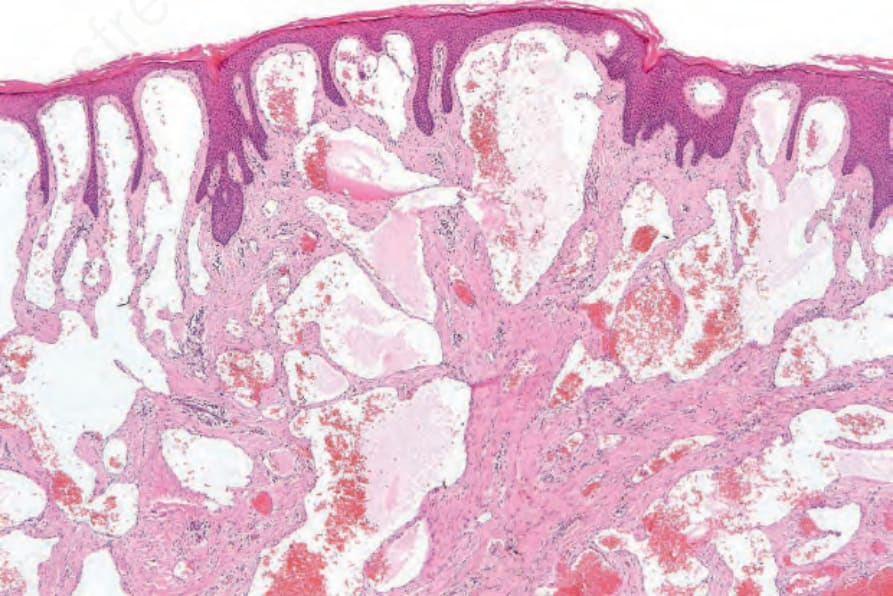
Fig. 35.597 Lymphangioma circumscriptum: thin-walled lymphatic channels are present in both the reticular and papillary dermis.
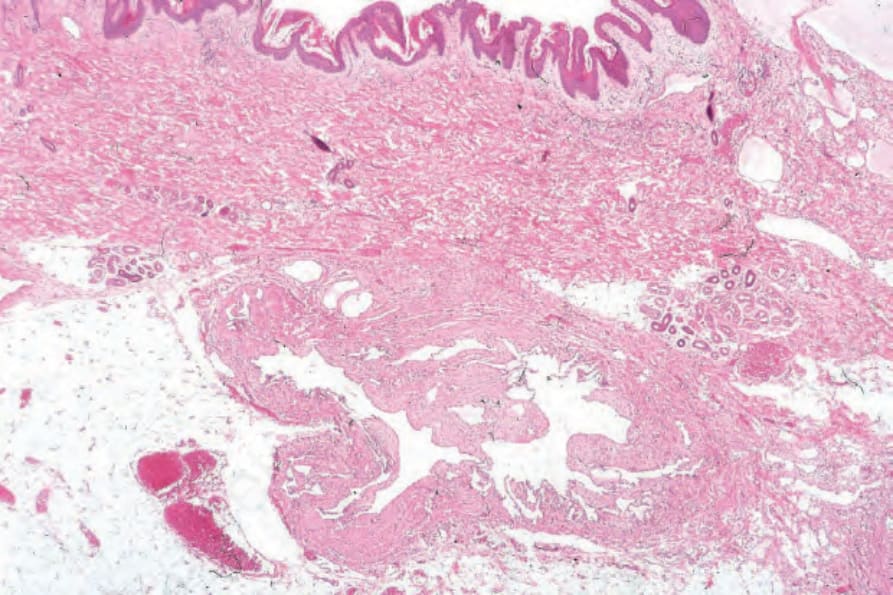
Fig. 35.598 Lymphangioma circumscriptum: within the subcutaneous fat is a large muscular ‘feeder’ lymphatic trunk. If this is not ligated at surgery, there is a high risk of recurrence.
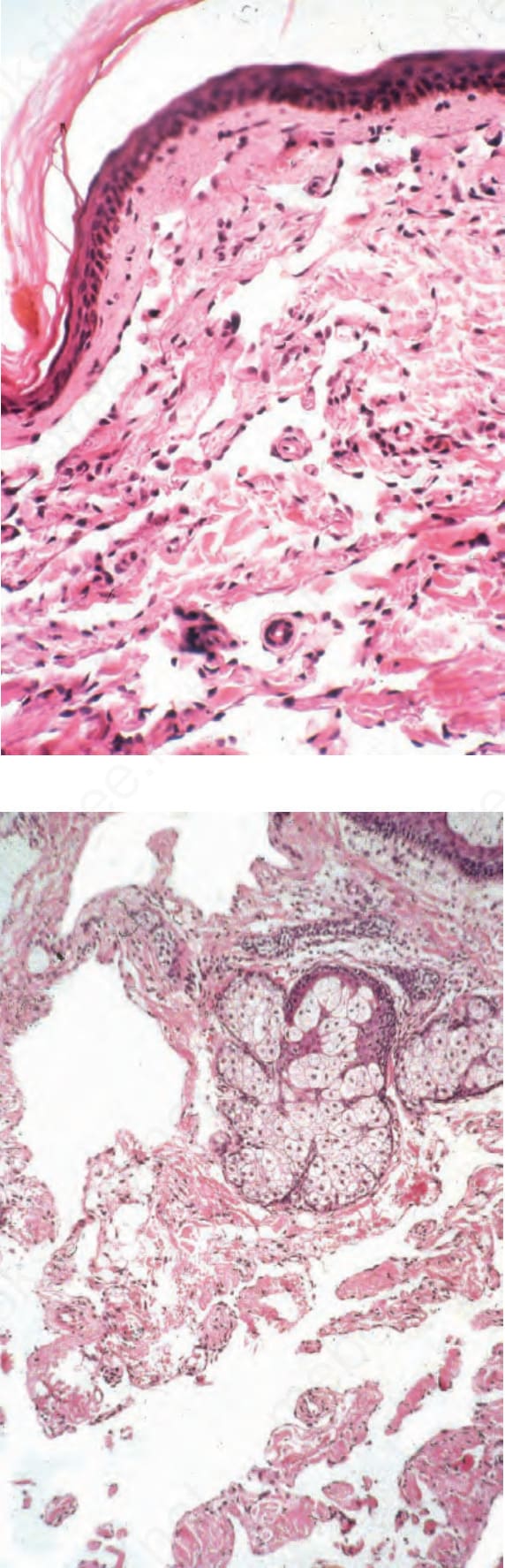
Fig. 35.599 Progressive lymphangioma: despite the architectural resemblance to angiosarcoma, there is a complete absence of endothelial multilayering or nuclear atypia.
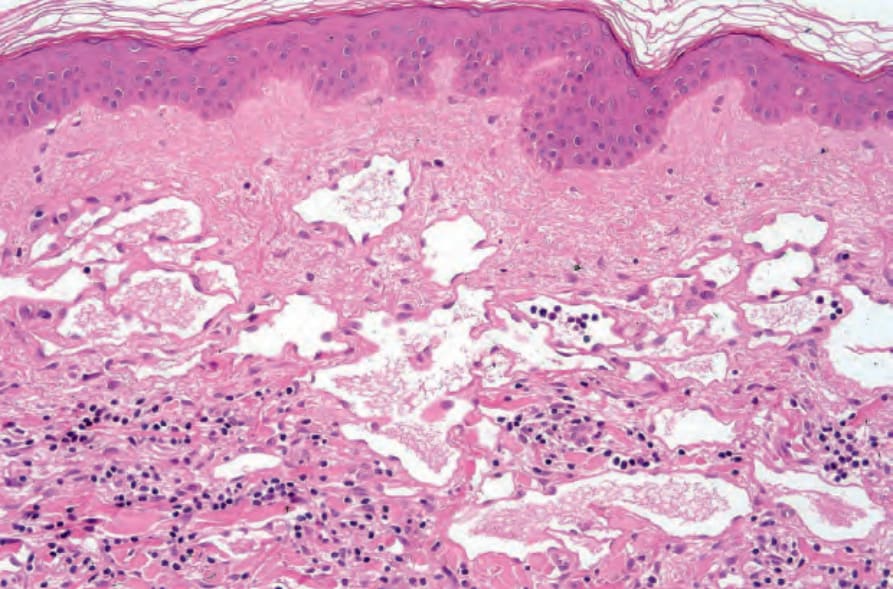
Fig. 35.600 Progressive lymphangioma: some cases show more dissection of dermal structures by the dilated lymphatic spaces.