Angiosarcoma
Angiosarcoma
The term angiosarcoma is synonymous with hemangiosarcoma and lymphangiosarcoma.
Clinical features Cutaneous angiosarcoma predominantly occurs in one of three clinical settings:
• idiopathic angiosarcoma of the head and neck,
• lymphedema-associated angiosarcoma,
• postirradiation angiosarcoma.1–9
Sporadic cases in the limbs (unassociated with lymphedema) may occur at any age. Very rare cases have been reported in association with vinyl chloride exposure, xeroderma pigmentosum, epidermolysis bullosa, stasis ulceration, a gouty tophus, as a complication of morbid obesity and in association with arthroplasty.10–17 It has been suggested that angiosarcomas developing in the setting of xeroderma pigmentosum may not be as aggressive as other angiosarcomas.18 A patient with Klippel-Trenaunay-Weber syndrome developed an angiosarcoma and a malignant peripheral nerve sheath tumor in the same involved limb.19 Development of angiosarcoma in a teratoma and a congenital example have also been documented.20,21 Angiosarcoma arising in other organs may metastasize to the skin.22,23 Rare cases in association with chronic immunosuppression in renal transplant patients and in HIV have been reported.24–27 Angiosarcoma in children is exceptional and tends to occur mainly in the soft tissues and internal organs, particularly the head and neck and mediastinum.28–32 Associated conditions in children other than the ones mentioned before, include congenital lymphedema, Aicardi syndrome and congenital hemangioma.33 The tumor may occasionally occur within a blood vessel, a hemangioma, nerve and in benign or malignant nerve sheath tumors.34–38 A case of multiple cutaneous and visceral vascular malformations associated with hepatic disseminated angiosarcoma has been reported.39
1858 Connective tissue tumors
Idiopathic angiosarcoma of the head and neck Idiopathic angiosarcoma of the head and neck is predominantly a tumor of late adulthood, with an equal sex incidence and a predilection for the scalp and central face.1,2,8,9 Involvement confined to the eyelid has been documented.40 It presents as single or multiple raised reddish or purple plaques, papules or nodules which may show a variable growth rate. High-grade lesions tend to ulcerate and bleed readily (Figs 35.569–35.574). The tumor is typically much more extensive than is clinically apparent. Spontaneous regression exceptionally occurs.41,42 Rare cases may mimic other diseases including rosacea and rhinophyma.43,44 Thrombocytopenia may rarely occur, probably as a result of platelet consumption and destruction within the tumor.45,46 Alopecia is an uncommon manifestation.47
Lymphedema-associated angiosarcoma Lymphedema-associated angiosarcoma (traditionally known as lymphangiosarcoma) classically arises on the arms of elderly females who have
undergone mastectomy with axillary lymph node dissection or radiotherapy many years previously (Stewart-Treves syndrome) (Fig. 35.575).48–51 It may also develop in other forms of iatrogenic lymphedema, congenital lymphedema, very rarely in a lymphangiomatous malformation, in association with elephantiasis, filariasis and even in areas of lymphedema secondary to morbid obesity.52–55 A case developing in an area of lipodermatosclerosis in a lower limb with changes of stasis has been reported.56 Lesions typically present as numerous purplish nodules or vesicles, often distributed over a wide area.
Postirradiation angiosarcoma Postirradiation angiosarcoma is the rarest of the three variants and can develop many years after radiotherapy for benign (hemangiomas, tinea capitis) or malignant conditions.57–62 Most cases are associated with radiotherapy from breast and gynecological cancer.63 In cutaneous postirradiation angiosarcoma of the breast there is usually no associated lymphedema
1859 Malignant vascular tumors
and the latency period is shorter than that in Stewart-Treves syndrome.64 Some cases of postirradiation angiosarcoma of the breast may be associated with chronic lymphedema and this may contribute to the development of the disease.65 A case following treatment of metastatic melanoma has been reported.66
All postirradiation angiosarcomas show high-level amplification of MYC, reflecting gains in chromosome 8q24 and this is regarded as an early necessary alteration in the development of the tumor.67,68 In about 25% of these cases there is co-amplification of FLT4, which encodes VEGFR3. Interestingly, these alterations are not found in atypical vascular proliferations associated with radiotherapy. Other types of cutaneous angiosarcomas also show MYC amplification.68–70
All forms of angiosarcoma carry a very poor prognosis, with repeated local recurrences, rapid dissemination and death in up to 80% of cases, often within a fairly short time.71–75 A retrospective study of angiosarcoma of the scalp and face found an improved 43% 5-year survival attributed to combined modality therapy.76 A further study including all sporadic cutaneous angiosarcomas, including those from the scalp and face and those with pure epithelioid morphology, found poor prognosis to be associated with necrosis, epithelioid morphology and old age (over 70 years).77 Local recurrence was associated with tumor depth. This study confirms findings of a previous study in which adverse prognosis correlated with size of the tumor, depth of invasion and mitotic rate.78 We regard pure cutaneous epithelioid angiosarcomas occurring outside the usual three clinical settings of angiosarcoma as a distinctive category of neoplasms with very poor prognosis (see below). Younger patients appear to have a better prognosis and radiation therapy appears to improve survival.79,80 It has been suggested that increased number of CD8 positive tumor-infiltrating correlate with better prognosis.81
Among metastatic sites, lymph nodes and lungs are the commonest. Interestingly, complete remission of a radioresistant, an inoperable and a metastatic angiosarcoma after treatment with liposomal doxorubicin, paclitaxel or a combination of the latter and sorefenib, respectively, have been reported.82–84
Pathogenesis and histologic features Cytogenetic analysis in a small number of superficial and deep angiosarcomas has shown complex chromosomal abnormalities mainly involving chromosomes 5, 7, 8, 13, 15, 20, 22, and Y.85 Activating mutations in KDR and other genes which may be amenable to therapeutic targeting have been documented.86 Mutations in PTPRB, PLCG1 and the ERK/MAPK pathway have been recently described.87,88 The genetic anomalies involving the ERK/MAPK pathway included mutations in KRAS, HRAS, NRAS, BRAF, MAPK1 and NF1 or amplifications in MAPK1/CRKL, CRAF or BRAF. Mutations in TP53 and losses of CDKN2A were also found in a smaller number of cases.88
Microscopically, all clinical variants are largely indistinguishable other than by the presence of coexistent lymphedema and are therefore considered together. The appearances are of an ill-defined infiltrative intradermal mass of numerous anastomosing vascular channels of varying caliber (Figs 35.576–35.579). The endothelium, which may be single or multilayered, is typically plump, pleomorphic and mitotically active (abnormal mitoses being quite common), and may form papillae or solid nests within vascular lumina. The vascular proliferation tends to ramify through the dermis, ‘dissecting’ the collagen bundles (Figs 35.580 and 35.581). Focal epithelioid change is not uncommon and can be prominent in some instances. In some cases, the tumor adopts (focally or diffusely) a solid, undifferentiated, spindled cell appearance, which is not easily recognizable as vascular in origin (Figs 35.582–35.584).
A number of cases appear to demonstrate true lymphatic differentiation, mainly those located on the scalp and face.89 These tumors are characterized by interconnecting irregular channels devoid of red blood cells lined by atypical hobnail endothelial cells, have stromal lymphoid aggregates and stain for lymphatic markers including D2-40, prox-1 and VEGFR-3. A small subset of angiosarcomas simulate Kaposi sarcoma, a feature also suggestive of lymphatic differentiation.90,91 Distinction from the latter is very difficult in some cases, as the promontory sign which is seen in many
1860 Connective tissue tumors
1861 Malignant vascular tumors
tumors with lymphatic differentiation particularly Kaposi sarcoma, may be seen in angiosarcoma.92 However, in the latter there is cytologic atypia, mitotic activity and multilayering.
A useful means of identifying the vascular nature of this tumor is by reticulin staining, which will demonstrate that in the better differentiated areas the tumor cells lie within a perivascular reticulin sheath; single cells are not surrounded by the reticulin framework (Fig. 35.585). Chronic inflammatory cells scattered throughout the tumor are often a prominent feature. In exceptional cases the infiltrate simulates a lymphoma and obscure the real tumor.93 Rare cases of angiosarcoma are mainly composed of cells with granular cytoplasm or signet ring appearance.94–96 A variant composed of foamy cells mimicking histiocytes has also been reported.97
In postirradiation tumors, capillary lobules may be present, and although this has been traditionally regarded as a feature indicative of a benign proliferation, in this setting it should raise the alarm about the presence of angiosarcoma.98,99
In poorly differentiated cases, it is useful to assess a panel of endothelial markers because individual antibodies tend to be variably positive in different tumors. These include von Willebrand factor (factor VIII-related antigen), CD31, CD34, FLI1 and ERG (Fig. 35.586). ERG is an ETS family transcription factor now regarded as the most sensitive and specific vascular marker.100,101 FLI1 is fairly sensitivity but less specific marker of endothelial
1862 Connective tissue tumors
cell differentiation.102 CD34 is variably positive and tends to be negative in angiosarcomas of the head and neck. Claudin-5 has been proposed as a good marker of angiosarcoma but it is positive in other vascular tumor and also in byphasic synovial sarcoma and carcinomas.103 CD30 is expressed in up to one third of angiosarcomas and this may be a source of confusion in poorly differentiated tumors.104
Tumors lacking epithelioid morphology are usually not positive for keratin and epithelial membrane antigen.105 It is important to remember that no antibody is entirely specific, and staining of histiocytes by CD31 may be a confounding feature in hemorrhagic atypical fibroxanthomas and my lead to a misdiagnosis of angiosarcoma.106 CD31 staining of histiocytes is cytoplasmic and granular, while staining of cells with endothelial cell differentiation reveals not only cytoplasmic staining but also crisp cytoplasmic membrane positivity.
Angiosarcomas are usually negative for HHV-8 except in tumors occurring in patients with AIDS.25
Ultrastructurally, the presence of Weibel-Palade bodies confirms the vascular nature of the tumor (Fig. 35.587). However, the latter technique is hardly used nowadays.
Differential diagnosis The presence of endothelial cell atypia, multilayering and mitotic activity allows ready distinction from a benign hemangioma (or lymphangioma) and Masson tumor. Occasional cases may need to be distinguished from spindle cell melanoma or carcinoma, in which circumstances immunohistochemistry is most helpful.
epithelioid angiosarcoma.4 Occasional cases have been associated with a foreign body, radiotherapy, an arteriovenous fistula, vascular dacron grafts and orthopedic joint prostheses.1–10 One case developed at a peristomal site and one within an ovarian teratoma.11,12
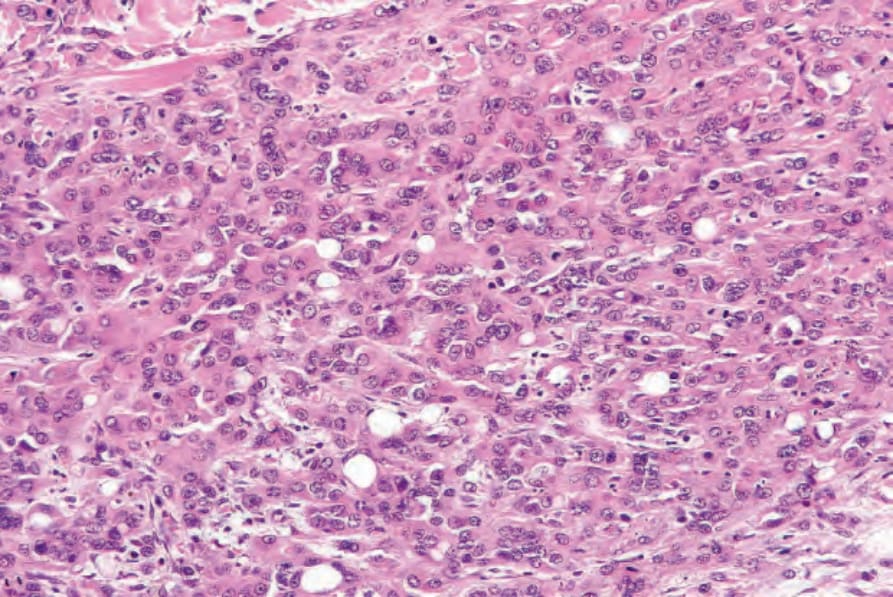
Fig. 35.566 Epithelioid hemangioendothelioma: this example is much more cellular. Intracytoplasmic lumina are still conspicuous.
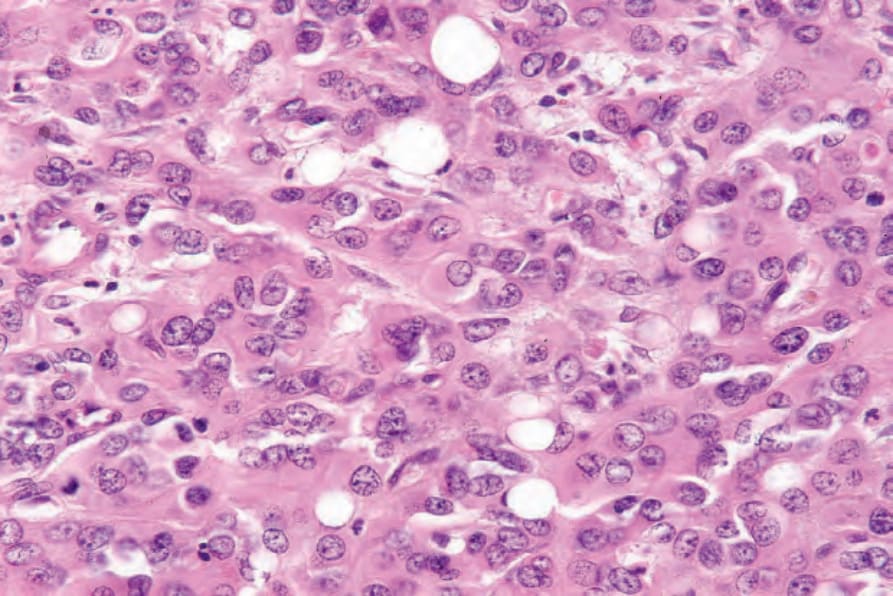
Fig. 35.567 Epithelioid hemangioendothelioma: high-power view.

Fig. 35.569 Angiosarcoma: there is a purplish bruise-like discoloration of the face with an infraorbital nodule. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 35.570 Angiosarcoma: ulcerated and hemorrhagic plaque on the frontal scalp. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 35.571 Angiosarcoma: note this diffuse crusted and ulcerated lesion. The face and scalp are sites of predilection. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 35.572 Angiosarcoma: patients often present with a bruise-like lesion. By courtesy of the Institute of Dermatology, London, UK.

Fig. 35.573 Angiosarcoma: the scalp, particularly in bald individuals, is a commonly affected site. By courtesy of the Institute of Dermatology, London, UK.
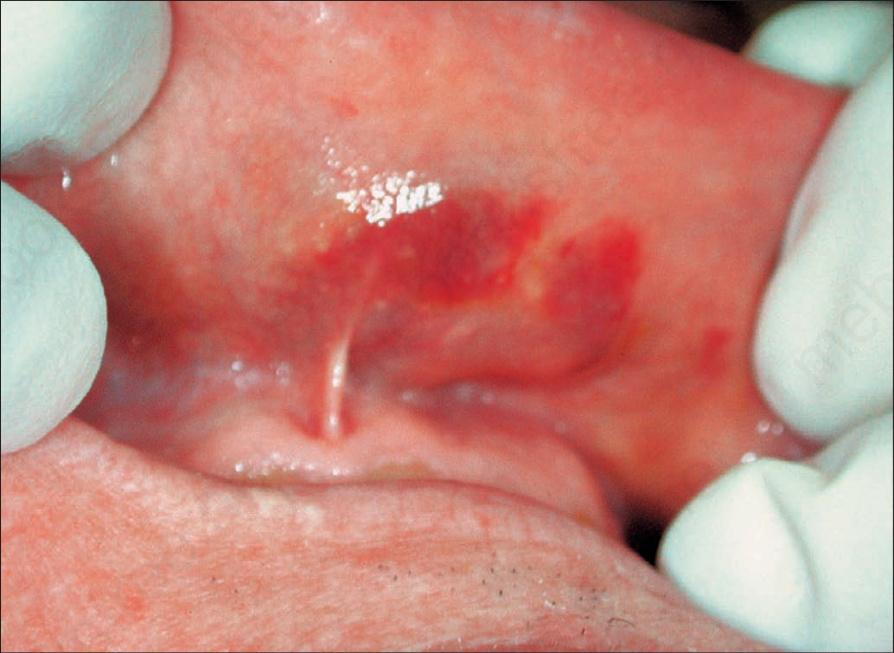
Fig. 35.574 Angiosarcoma: oral lesions in a patient with minimal cutaneous involvement highlighting the multifocality of the process. By courtesy of the Institute of Dermatology, London, UK.

Fig. 35.575 Lymphedema-associated angiosarcoma (Stewart- Treves tumor): very marked lymphedema has complicated radical mastectomy in this elderly female patient. There is diffuse involvement of the arm by tumor.
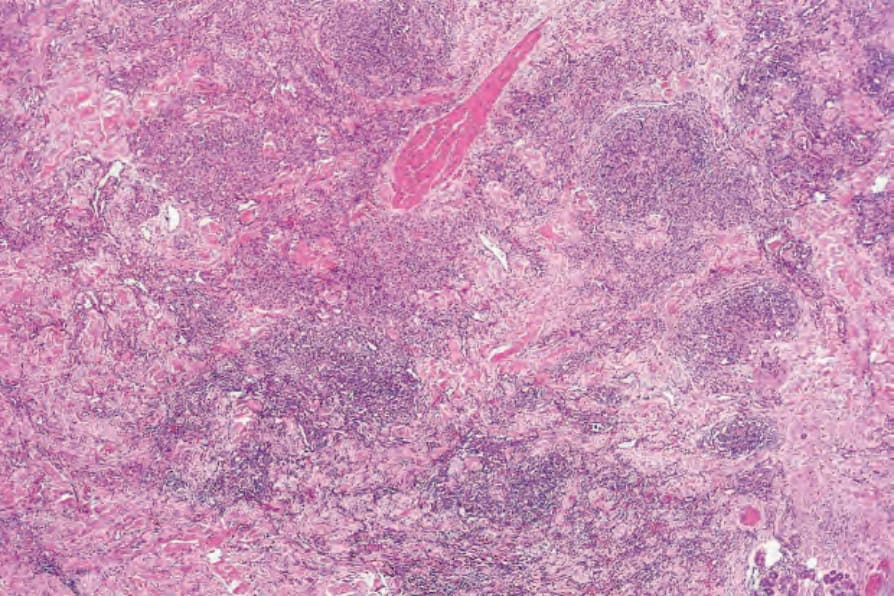
Fig. 35.576 Angiosarcoma: this low-power view shows extensive infiltration of the dermis by a vascular tumor.
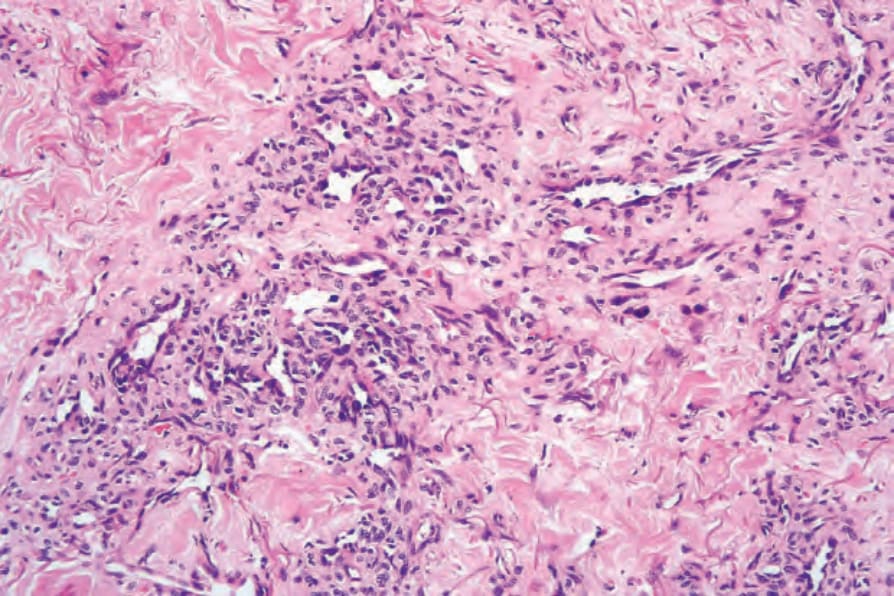
Fig. 35.577 Angiosarcoma: the endothelial cells are pleomorphic and hyperchromatic.
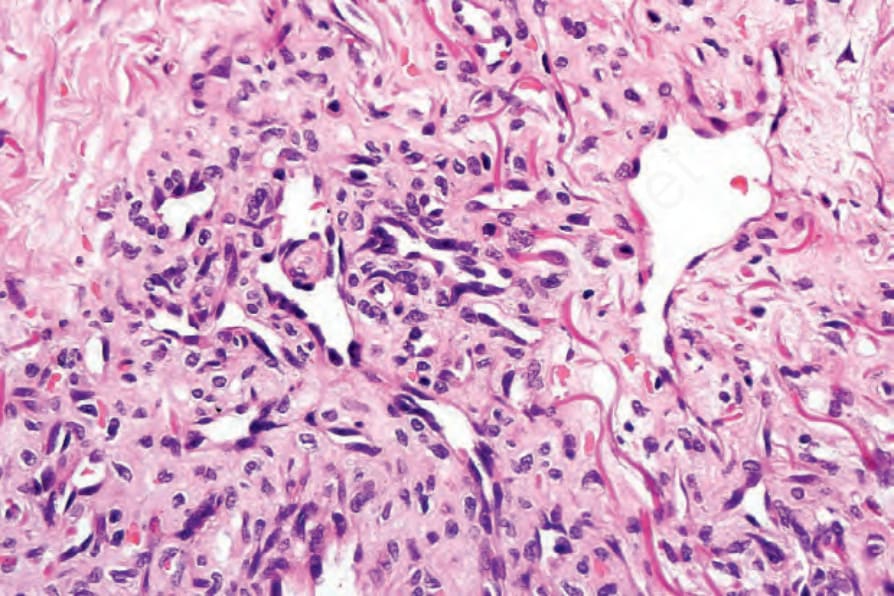
Fig. 35.578 Angiosarcoma: high-power view.
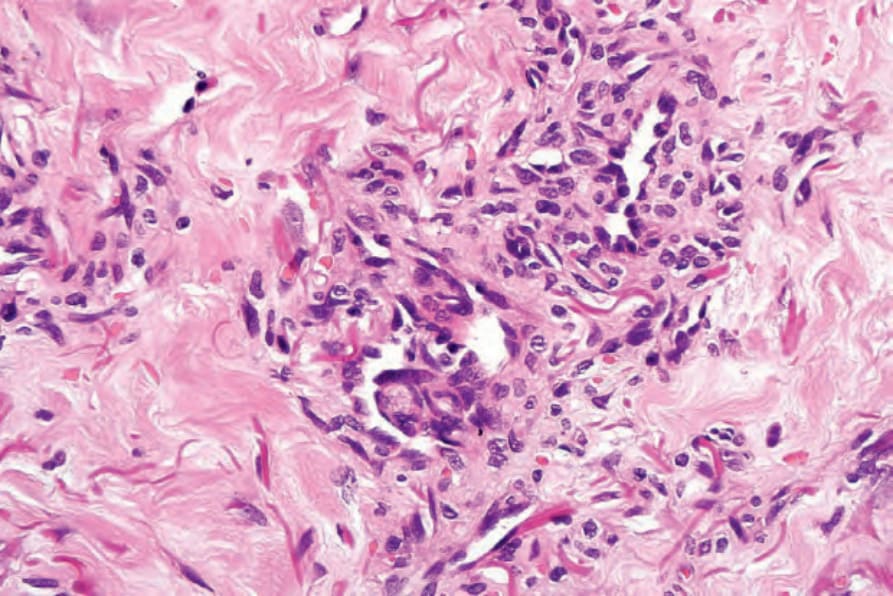
Fig. 35.579 Angiosarcoma: in this example, intraluminal papillae are present.
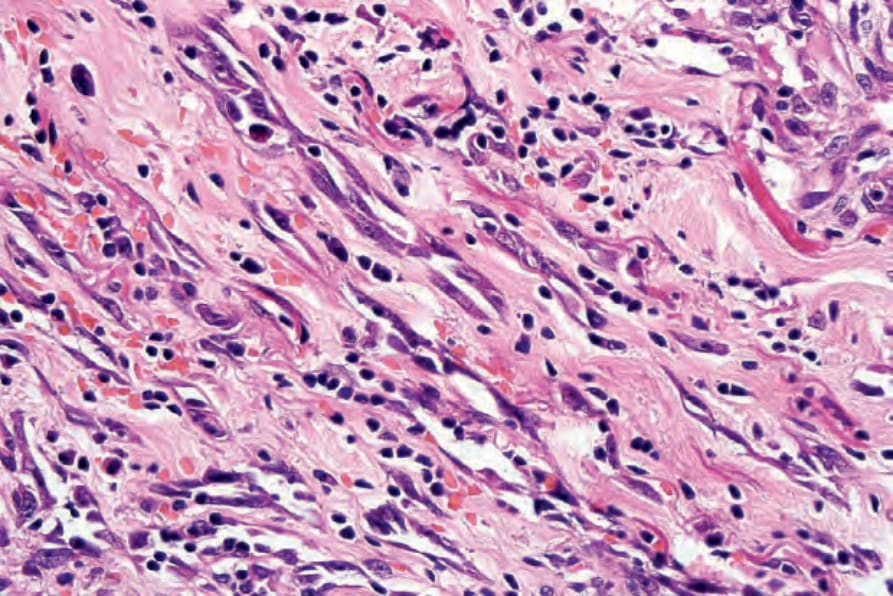
Fig. 35.580 Angiosarcoma: note the spindled cell population with vesicular nuclei and prominent nucleoli.
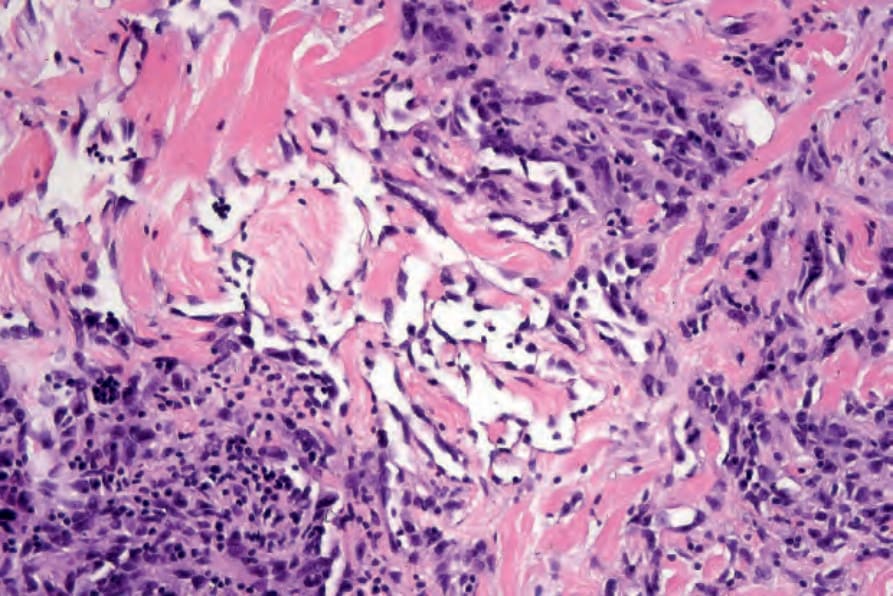
Fig. 35.581 Angiosarcoma: there is conspicuous dissection of collagen.
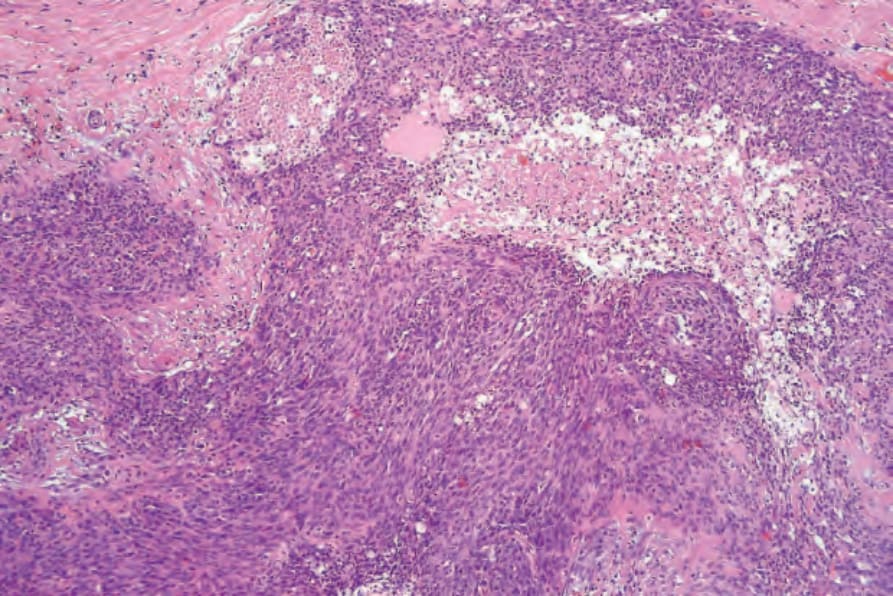
Fig. 35.582 Angiosarcoma (spindle cell variant): the dermis is extensively infiltrated by a spindled cell tumor.
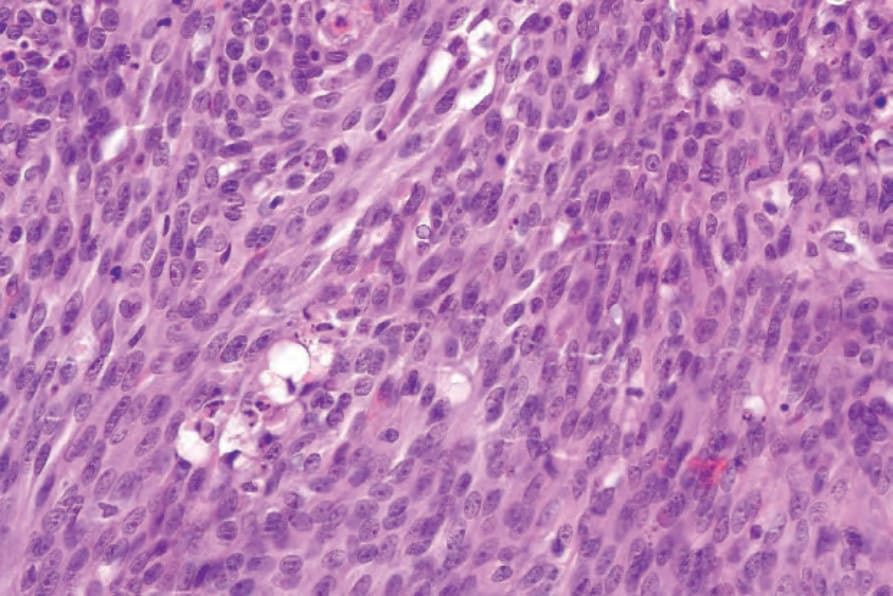
Fig. 35.583 Angiosarcoma (spindle cell variant): the spindle cells have eosinophilic cytoplasm and pleomorphic, vesicular nuclei. Intracytoplasmic lumina are apparent.
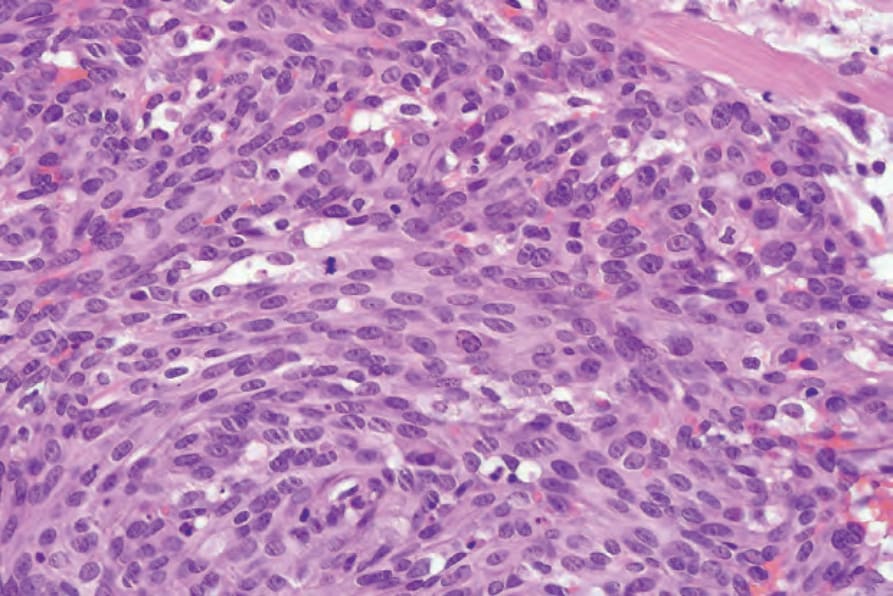
Fig. 35.584 Angiosarcoma (spindle cell variant): note the mitotic activity.
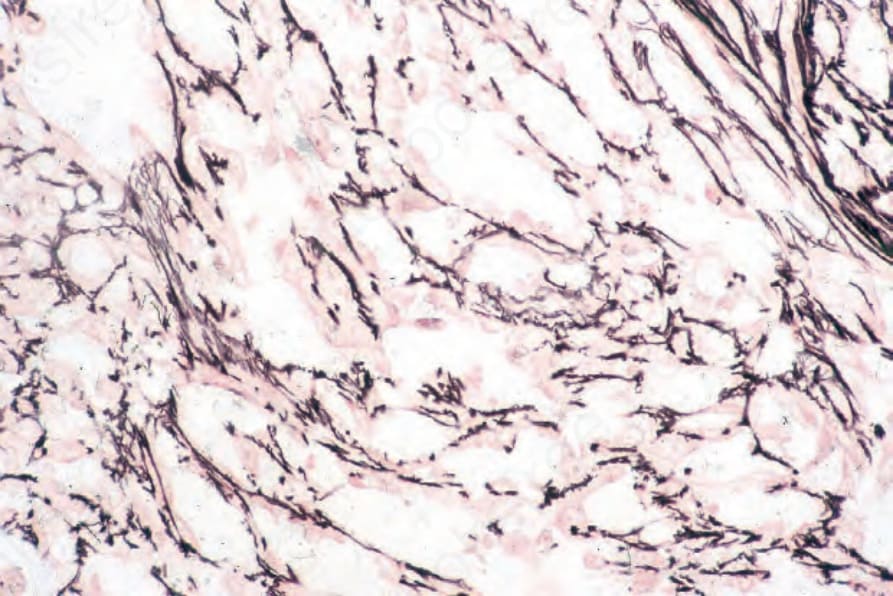
Fig. 35.585 Angiosarcoma: the tumor cells are enclosed within a reticulin sheath.
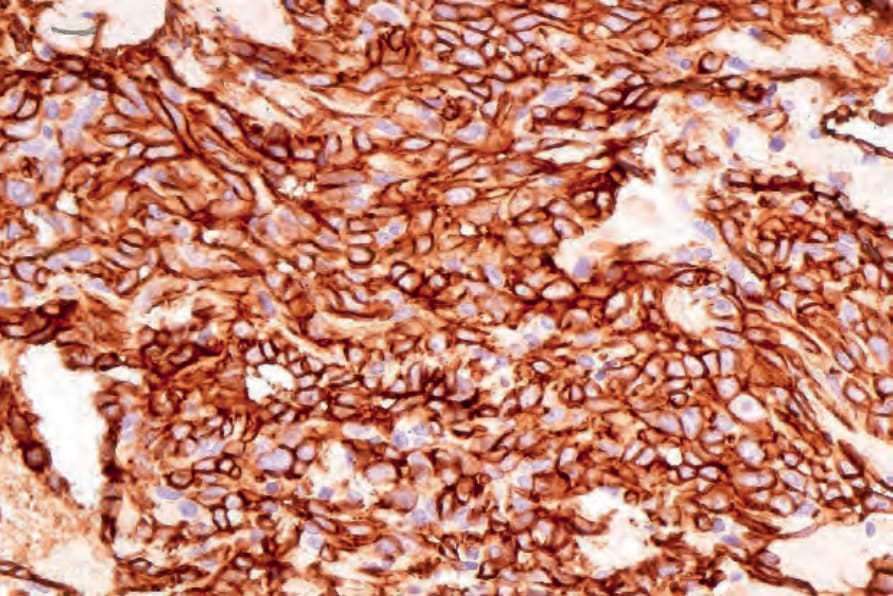
Fig. 35.586 Angiosarcoma: the tumor cells express CD31.
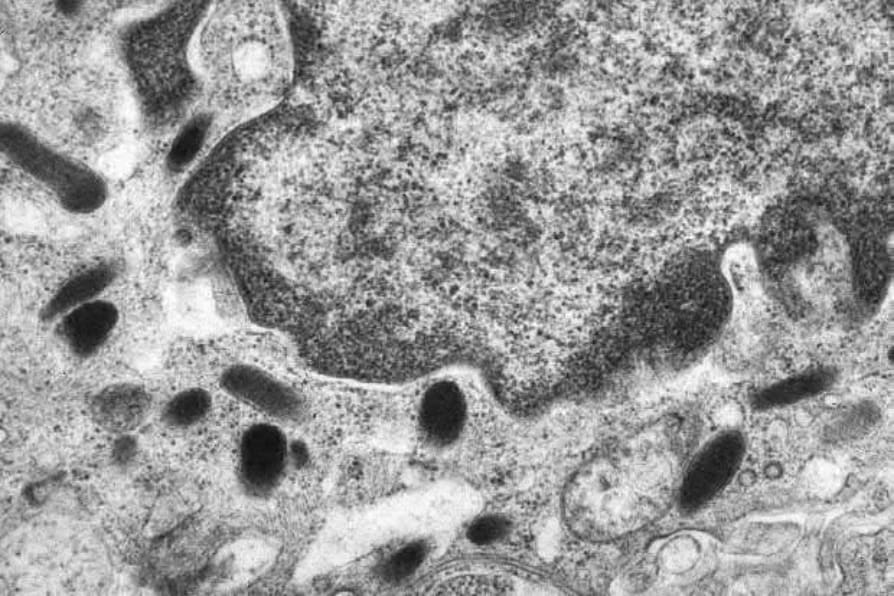
Fig. 35.587 Angiosarcoma: in spindle cell variants, the diagnosis is sometimes confirmed ultrastructurally by the identification of Weibel-Palade bodies.
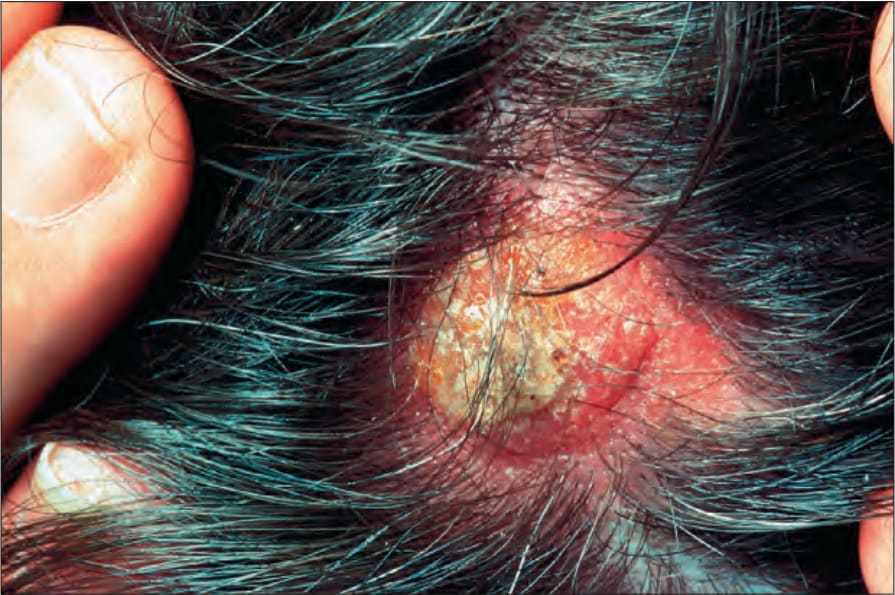
Fig. 35.588 Epithelioid angiosarcoma: presentation on the scalp is not uncommon. The lesion is less obviously vascular when compared with more typical angiosarcoma. By courtesy of the Institute of Dermatology, London, UK.
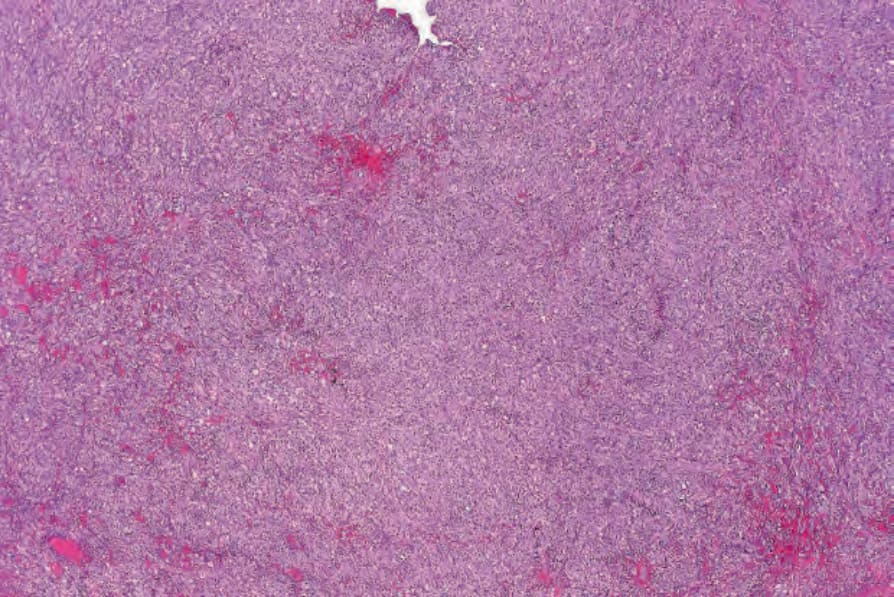
Fig. 35.589 Epithelioid angiosarcoma: there is a diffuse epithelioid cell infiltrate with multiple foci of hemorrhage.