Epithelioid hemangioendothelioma
Epithelioid hemangioendothelioma
Clinical features Epithelioid hemangioendothelioma was originally described in 1982 as a distinctive low-grade malignancy in soft tissues.1,2 However, this tumor is now classified as fully malignant in view of its behavior with potential for metastatic spread and mortality (see below). Identical cases involving other organs (mainly lung, liver and bone) have been described in the past under different names. Most cases present in adults and only rarely in children.3–5 Tumors can arise in any organ, as up to 50% of cases develop from a blood vessel, most often a vein. Pain is often a symptom. Multicentric disease is common, especially in the lungs, liver and bones. Involvement of the skin, which is relatively rare, may be associated with an underlying bone or soft tissue lesion and is occasionally multicentric. Cutaneous epithelioid hemangioendothelioma is rare, with wide anatomical distribution and no distinctive clinical features have been described.6–31 Skin lesions may present in isolation or associated with lesions in other organs either simultaneously or before or after the cutaneous presentation. Intraoral lesions are very rare.32,33 An adult patient with a hepatic tumor presented with
Pathogenesis and histologic features Cytogenetic studies have shown a distinctive t(7;19)(q11;q13) translocation resulting in fusion of the SERPINE 1 and FOSB genes.12–15
Tumors are not vasoformative and consist of poorly circumscribed nodules composed of fascicles or sheets of plump, brightly eosinophilic spindle cells with vesicular nuclei intermixed with variable numbers of cells with rhabdoid appearance (pink cytoplasm and eccentric nucleus) (Figs 35.558–35.560). Nuclear atypia is generally mild, and mitoses are sparse.
1856 Connective tissue tumors
Kasabach-Merritt syndrome and in a further patient the tumor presented after radiotherapy for a congenital hemangioma.34,35 Metastasis and mortality rates vary according to the organ involved, but it is generally believed that no more than 30% metastasize. Cases with isolated cutaneous lesions usually but not always tend to have an indolent behavior.
Pathogenesis and histologic features The translocation t(1;3)(p36.3;q25) resulting in a WWTR1-CAMTA1 gene fusion has been demonstrated in virtually all cases of epithelioid hemangioendothelioma.36–41 A t(10;14)(p13;q24) producing a YAP1-TFE3 fusion have also rarely been identified.42,43 WWTR1-CAMTA1 and YAP1-TFE3 gene rearrangements can sometimes coexist.44
Microscopically, most tumors are ill defined, infiltrative and composed of rounded, polygonal or short spindle-shaped cells with pink cytoplasm and vesicular nuclei. They are arranged in short cords or nests and are surrounded by abundant myxoid or hyaline stroma (often with a somewhat chondroid appearance and rich in sulfated acid mucopolysaccharides) (Figs 35.561 and 35.562). Intracytoplasmic lumina with occasional erythrocytes are often prominent and resemble primitive vascular channels (Figs 35.563–35.565). Well-formed vessels, however, are not a feature of most cases or are infrequent. Calcification, ossification and (less commonly) osteoclast-like giant cells can be present.45,46 Rare cases show significant cytologic atypia and a high mitotic rate, demonstrating a continuum with epithelioid angiosarcoma (Figs 35.566–35.568). Tumors of larger size and increased mitotic activity are associated with higher mortality. Poor prognosis is associated with tumors larger than 3 cm and more than three mitotic figures per 50 high-power fields. Necrosis, tumor site, cytologic atypia, and spindling of tumor cells do not seem to be affect prognosis.47
Immunohistochemically, the tumor cells label for vascular markers including ERG, CD31, CD34, podoplanin and FLI-1.48–50 CD10 is usually positive and keratin expression is seen in up to 25% of cases.51,52 Actin positivity may also be present.2,53,54 CD30 expression has also been reported.55 EMA is usually negative. CAMTA1 immunohistochemistry, which is usually expressed as positive nuclear staining helps in the differential diagnosis with other tumors with epithelioid morphology.56,57
Differential diagnosis In epithelioid hemangioma, there is prominent inflammation, and well-formed blood vessels predominate. Metastatic adenocarcinoma usually
1857 Malignant vascular tumors
shows more pleomorphism and is positive for epithelial markers including EMA and negative for vascular markers. Mucin stains are often positive in the tumor cell cytoplasm. Epithelioid sarcoma generally shows a more sheet-like growth pattern (at least in areas) and only occasional cytoplasmic vacuoles. It is positive for both keratin and EMA, often CD34 positive, but negative for ERG, CD31, von Willebrand factor, INI1 and CAMTA1. Epithelioid angiosarcoma lacks a fibromyxoid or sclerotic stroma and tends to consist of sheets of pleomorphic epithelioid cells with intracytoplasmic lumina and little tendency to form vascular channels. In addition, the latter is not associated with CAMTA1-WWTR1 fusions. Myxoid chondrosarcoma has a lobular architecture; the tumor cells are S100 protein positive and lack intracytoplasmic lumina.
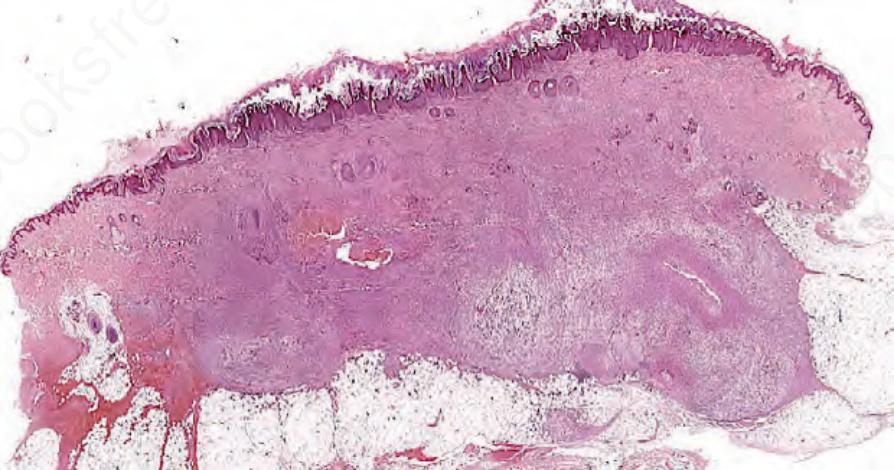
Fig. 35.558 Pseudomyogenic hemangioendothelioma: prominent involvement of the dermis and subcutaneous tissue by an infiltrative tumor.
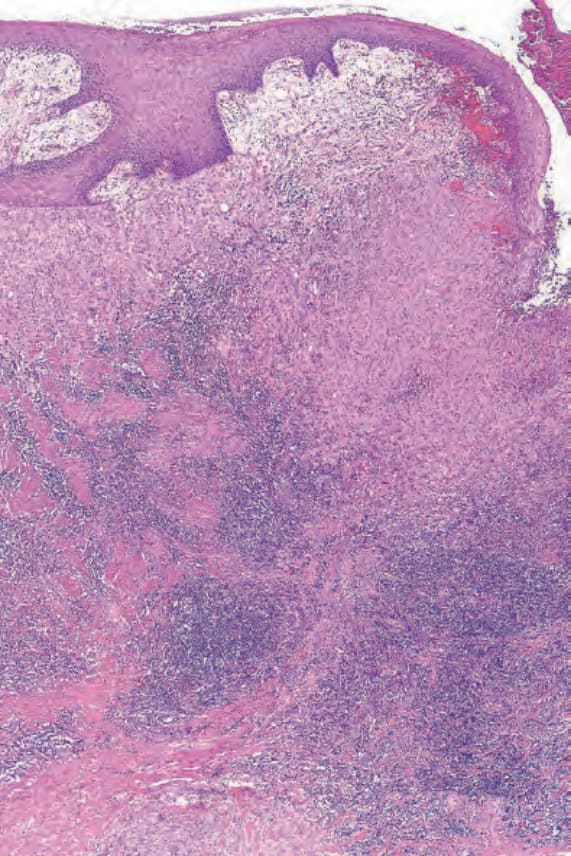
Fig. 35.561 Epithelioid hemangioendothelioma: this is the edge of an ulcerated lesion. Tumor is present superficially and is bordered by a heavy lymphoid infiltrate.
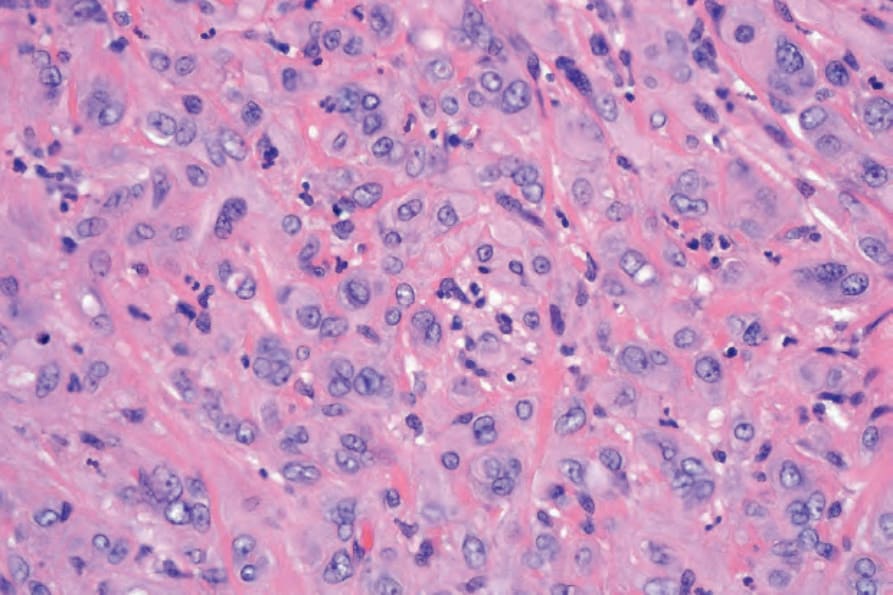
Fig. 35.562 Epithelioid hemangioendothelioma: the tumor cells have eosinophilic cytoplasm and large vesicular nuclei.
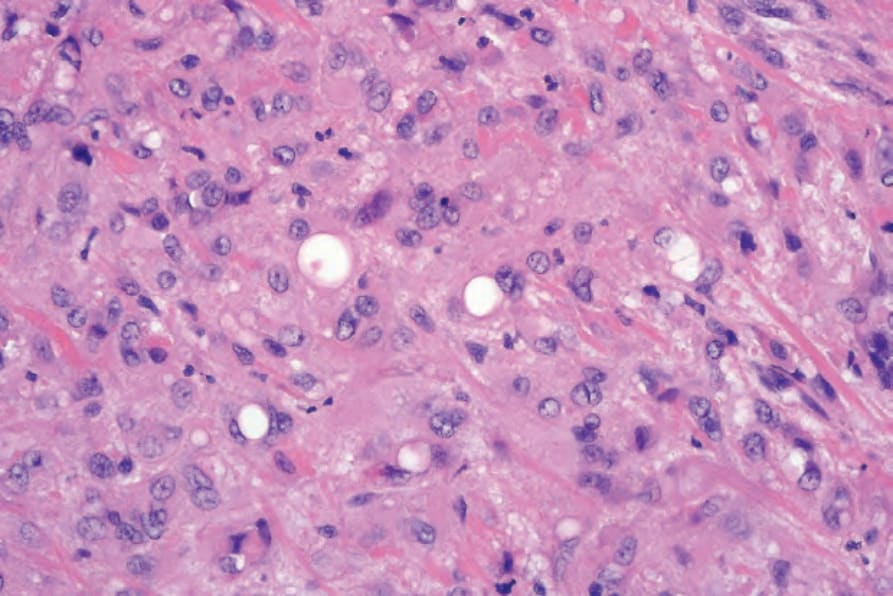
Fig. 35.563 Epithelioid hemangioendothelioma: intracytoplasmic lumina are a characteristic feature.
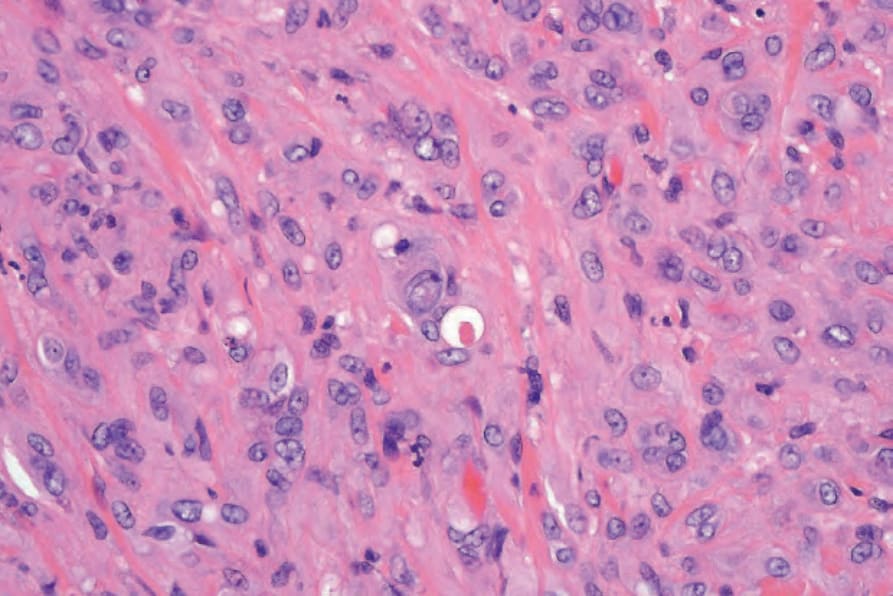
Fig. 35.564 Epithelioid hemangioendothelioma: careful scrutiny often reveals erythrocytes within the intracytoplasmic lumina.
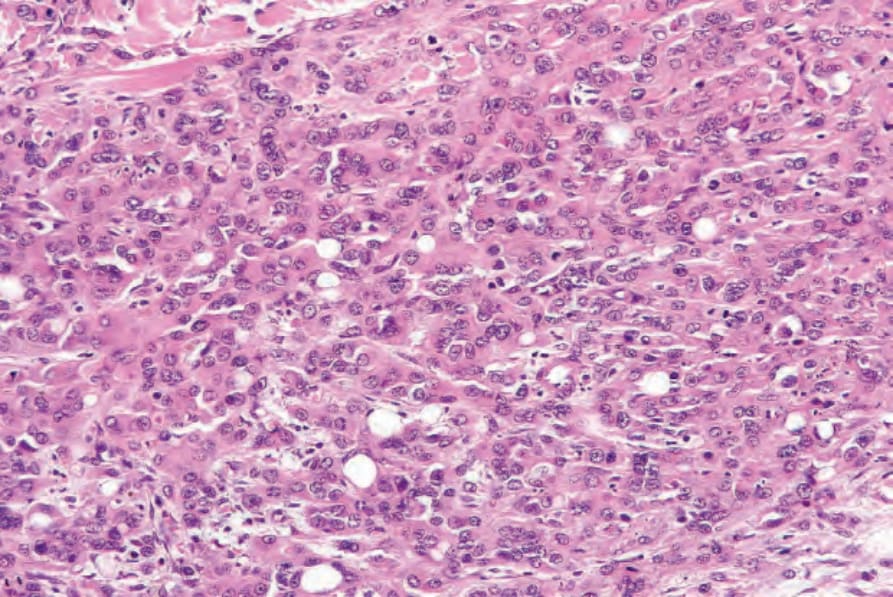
Fig. 35.566 Epithelioid hemangioendothelioma: this example is much more cellular. Intracytoplasmic lumina are still conspicuous.
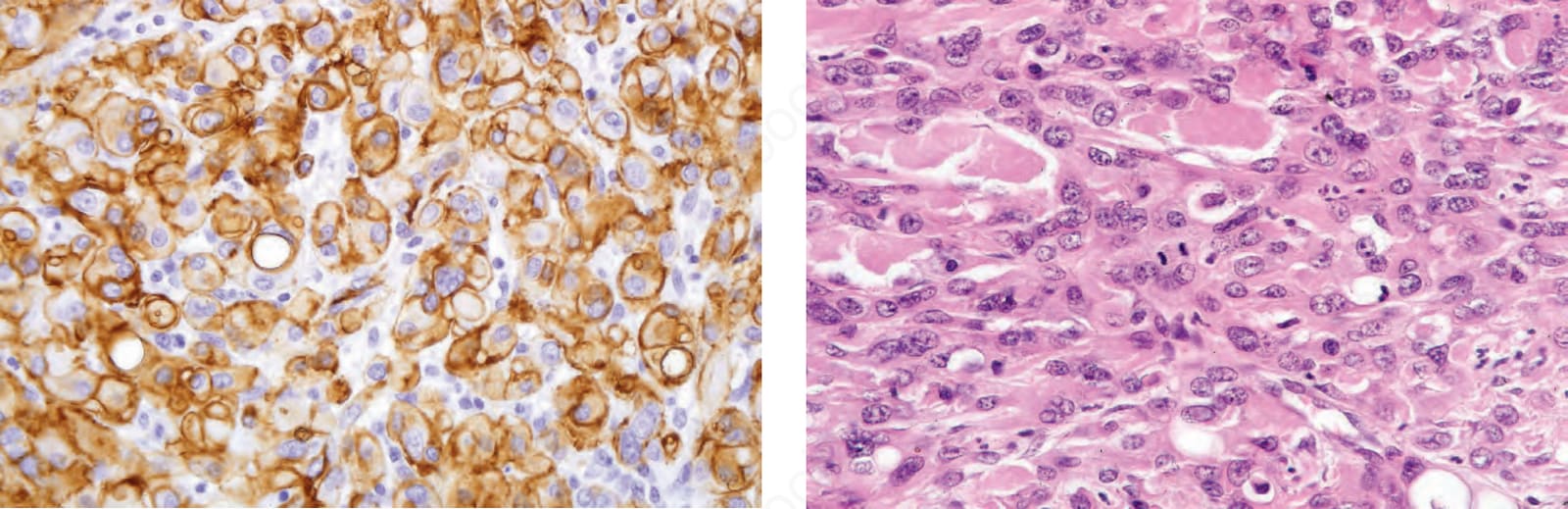
Fig. 35.568 Epithelioid hemangioendothelioma: note the mitotic figures.