Kaposi sarcoma
Kaposi sarcoma
The histogenesis of Kaposi sarcoma has been a source of debate for many years; currently, it appears most likely that it is derived from endothelial cells, particularly lymphatic endothelium.1–3 However, some studies have demonstrated a mixed cell population. Although we include Kaposi sarcoma in the group of low-grade malignant vascular tumors, in keeping with present convention, the issue about whether it is a reactive or neoplastic process remains controversial. Clonality has occasionally been found, supporting a neoplastic process, but other studies have not confirmed this.4–6 Although occasional cases of Kaposi sarcoma may have an aggressive behavior, at present most evidence suggests that the process is more likely to be reactive.7 This is further supported by the discovery of DNA sequences from a distinctive new type of human herpesvirus (HHV-8, KS-associated herpesvirus) in all types of Kaposi sarcoma.8–11 A study of multicentric advanced lesions of Kaposi sarcoma has shown that although some tumors are clonal most advanced cases represent oligo clonal proliferations, suggesting that the process is reactive rather than neoplastic.12 Serological evidence of infection by the virus is found before patients develop the tumor.13,14 HHV-8 is also associated with multicentric Castleman disease and primary effusion lymphoma.15
Histologically, tumors are lobular, infiltrative and composed of fascicles of bland endothelial cells, congested capillaries, slit-like vascular spaces and occasional pale epithelioid endothelial cells (Fig. 35.528). Different areas resemble either Kaposi sarcoma or capillary hemangioma (Fig. 35.529). Focally, the capillaries may show thrombosis, especially at the periphery of tumor lobules. Areas resembling lymphangioma are often seen.5
Epithelioid cells can contain hemosiderin granules, hyaline globules, and even cytoplasmic vacuoles. Rare hyaline globules can be seen in the spindle cells. Inflammatory cells are usually sparse, and mitotic figures are rare.
Biopsies of lesions after Kasabach-Merritt syndrome tend to show histologic features that resemble tufted angioma.29 In one case, prominent telangiectasia and amianthoid-like fibrosis were described.36 In an exceptional case, changes of lymphangiomatosis predominated and those of kaposiform hemangioendothelioma were only focal and microscopic.37
Endothelial cells in the tumor are positive for ERG, CD31, CD34 and FLI-1 but negative for GLUT-1 and LeY (juvenile hemangioma-associated antigens).17,38 Podoplanin is positive in the bulk of tumor lobules but negative in the dilated blood vessels.39 Focal actin positivity is seen in areas with epithelioid morphology. HHV-8 has not been demonstrated.
Clinical features Kaposi sarcoma may be divided into four distinct clinical groups:16–20
• Classic (endemic) Kaposi sarcoma most often arises in elderly males and shows a predilection for the distal extremities (Figs 35.530 and 35.531).16–18 Mediterranean and Jewish populations are most often affected. Familial cases are exceptional and presentation in children is very uncommon.19,20 Lesions have been reported in children born to consanguineous parents, suggesting an autosomal recessive predisposition that facilitates induction of the tumor by HHV-8.21 Internal lesions are distinctly uncommon and mucosal lesions are rare.22 Disseminated disease is very rare.23 The condition generally tends to pursue a prolonged indolent and only very rarely fatal course, but such patients have a higher incidence of lymphoreticular neoplasms, especially non-Hodgkin lymphoma.24,25 Aggressive behavior has only exceptionally been documented.26
1849 Vascular tumors of low-grade or borderline malignancy
• AIDS-related Kaposi sarcoma commonly presents in young adults, mostly males, many of whom either are homosexual or abuse drugs (Figs 35.532 and 35.533).27–29 Lesions are much less common in women and children.30 The tumor often disseminates widely and rapidly and may prove fatal. However, with the advent of highly active antiretroviral therapy, the incidence of Kaposi sarcoma has decreased dramatically, and when lesions develop they tend to be limited. The skin (especially of the trunk and limbs) and mucosae are usually extensively involved. Lesions may occur as a result of the immune reconstitution inflammatory syndrome.31,32 The condition can also develop in association with chronic lymphedema in HIV-positive patients.33
• Immunosuppression-associated Kaposi sarcoma is rare and presents in patients receiving immunosuppressive therapy, especially after kidney transplantation.34–36 Although the course of the disease tends to be indolent, it can occasionally be aggressive. Regression of the lesions sometimes occurs after immunosuppression is stopped or reduced. Kaposi sarcoma in this setting may be induced by local immunosuppression, for example after infiltration of steroids or the use of topical tacrolimus.37,38 Chronic use of systemic steroids, leflunomide and other immunosuppressive drugs outside the setting of transplantation can also induce lesions.39,40,41 A case associated with a hypothalamic adrenocorticotropic hormone-secreting adenoma has been documented.42 Interestingly, although immunosuppressive drugs such as sirolimus may induce recurrence of Kaposi sarcoma, in several instances complete regression has been noted after the introduction of the drug.43–45 Kaposi sarcoma has been described in a patient with idiopathic low CD4 counts.46
• African Kaposi sarcoma includes those cases arising largely in sub-Saharan Central Africa.17,18,47,48 In this region, Kaposi sarcoma has long been endemic and accounts for up to 10% of all cases of ‘malignant’ disease. Within this category there are two clinical subgroups: those arising predominantly on the limbs of middle-aged
men and tending to be fairly indolent; those arising in young children who typically present with visceral or lymph node involvement and in whom the disease is usually fatal. In addition, there are a large number of AIDS-related cases in young African adults of either sex (see above). Clinically, the cutaneous lesions present similarly in all the subtypes. They commence as small, reddish-blue macules or flat plaques, which are often multiple and gradually enlarge. They may become nodular, and sometimes coalesce to form larger lesions (Fig. 35.534). Some may regress as new lesions continually form and others ulcerate and fungate. The rate of spread
1850 Connective tissue tumors
or enlargement is usually related to the clinical subgroup into which the patient falls.
Regression may occur in a number of settings, particularly after immunosuppression is stopped or reduced. Anecdotal examples of regression have been reported with imatinib and sorafenib.49,50
Histologic features The microscopic appearances of Kaposi sarcoma go through three phases, apparently related to the duration of the lesion.27–29,51 There is morphological overlap between patch and plaque phases, but nodular lesions appear distinct. Lesions usually involve the dermis and may extend to the subcutaneous tissue. Purely subcutaneous tumors are rare.52
• The early patch stage is characterized by a mild increase in the number of dermal vessels showing minimal endothelial atypia and characteristically surrounded by an admixture of lymphocytes and plasma cells associated with hemosiderin deposition and red cell extravasation (Figs 35.535–35.539). These vessels are arranged mainly parallel to the epidermis, may dissect between collagen bundles and surround adnexal structures and vessels (the promontory sign). This stage of Kaposi sarcoma is the most difficult to recognize as it bears a superficial resemblance to granulation tissue.
1851 Vascular tumors of low-grade or borderline malignancy
• The plaque stage is typified by more obvious and extensive dermal vascular proliferation, the lumina of which vary considerably in caliber (Figs 35.540–35.544). Endothelial cells may appear plump, but remain single layered. Noticeable at this stage is the appearance of eosinophilic spindled cells in the dermis around these vessels. These cells have tapering, somewhat hyperchromatic nuclei. The margins of the lesion are ill defined and primitive vascular clefts may be apparent within the spindle cell mass. Chronic inflammatory cells remain a prominent feature.
• The nodular stage is manifest predominantly as a relatively well-circumscribed dermal mass of variably eosinophilic spindle cells (Fig. 35.545). Scattered between these cells are numerous irregular, slit-like, vascular spaces, which lack an endothelial lining, but often contain extravasated red cells. In cross-section these spaces resemble a sieve (Figs 35.546–35.549). Readily identifiable ectatic vessels may, however, still be apparent at the periphery of the nodule. Normal mitotic activity is most prominent at this stage. A chronic inflammatory infiltrate including histiocytes is variably conspicuous. The spindle cells are consistently CD34 positive and also CD31 positive (Fig. 35.550). Focal positivity for actin is also seen. Rarely, nodular Kaposi sarcoma is entirely or partially intravascular.53
1852 Connective tissue tumors
1853 Vascular tumors of low-grade or borderline malignancy
In HIV-positive patients with Kaposi sarcoma, treatment with paclitaxel or the angiogenesis inhibitor Col-3 induces partial or complete regression of lesions.62 Histologically, in partial regression, there is reduction in spindled cells and fibrosis. In complete regression, there is fibrosis, lymphocytic inflammation and hemosiderin deposition. In patients on HAART, lesions can also change, becoming more circumscribed, less cellular and surrounded by a thick band of fibrosis.63
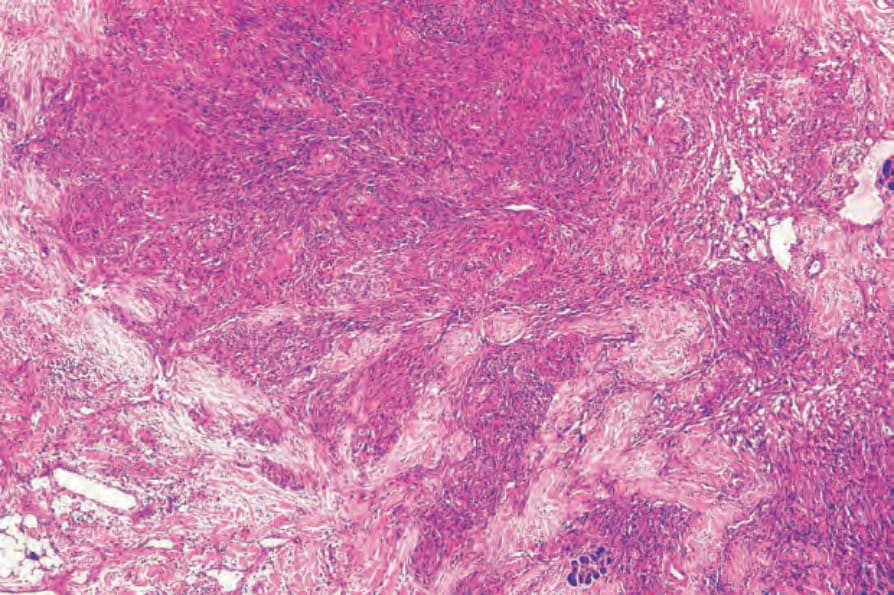
Fig. 35.528 Kaposiform hemangioendothelioma: nodular proliferation with lobular, vascular and spindle cell areas.
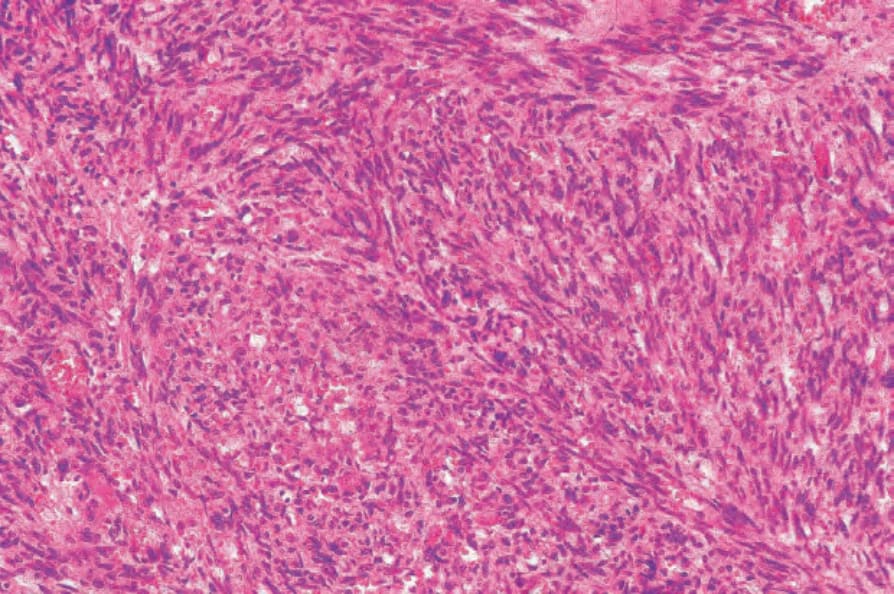
Fig. 35.529 Kaposiform hemangioendothelioma: in this field, the features are reminiscent of Kaposi sarcoma.

Fig. 35.530 Classic Kaposi sarcoma: the distal extremities are typically involved. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 35.531 Classic Kaposi sarcoma: numerous tumor nodules are present. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 35.532 AIDS-related Kaposi sarcoma: darkly pigmented plaques are widely distributed on this young man’s chest and abdomen. From the collection of the late N.P. Smith, MD, Institute of Dermatology, London, UK.

Fig. 35.533 AIDS-related Kaposi sarcoma: infraorbital and nasal purple plaques are present. From the collection of the late N.P. Smith, MD, Institute of Dermatology, London, UK.
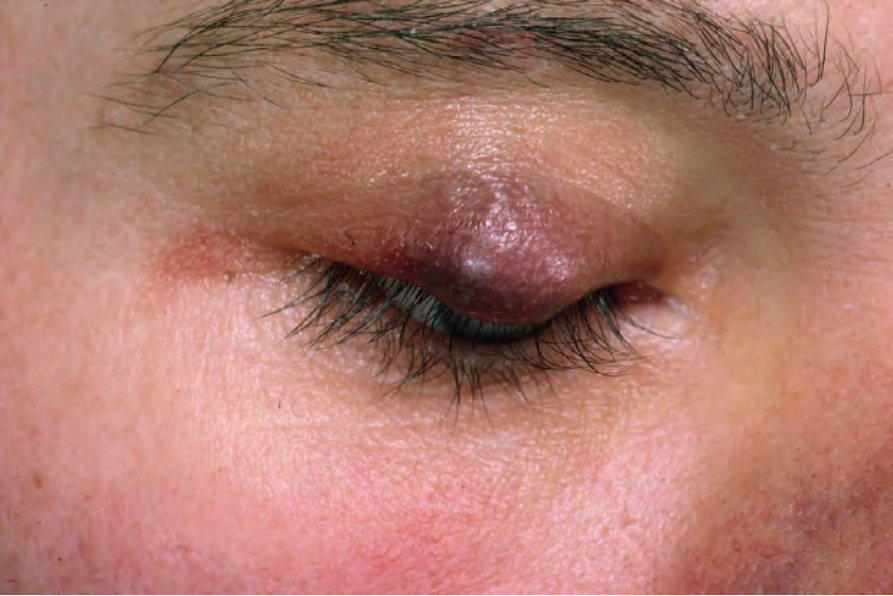
Fig. 35.534 Kaposi sarcoma: a tumor nodule is present on the upper eyelid. From the collection of the late N.P. Smith, MD, Institute of Dermatology, London, UK.
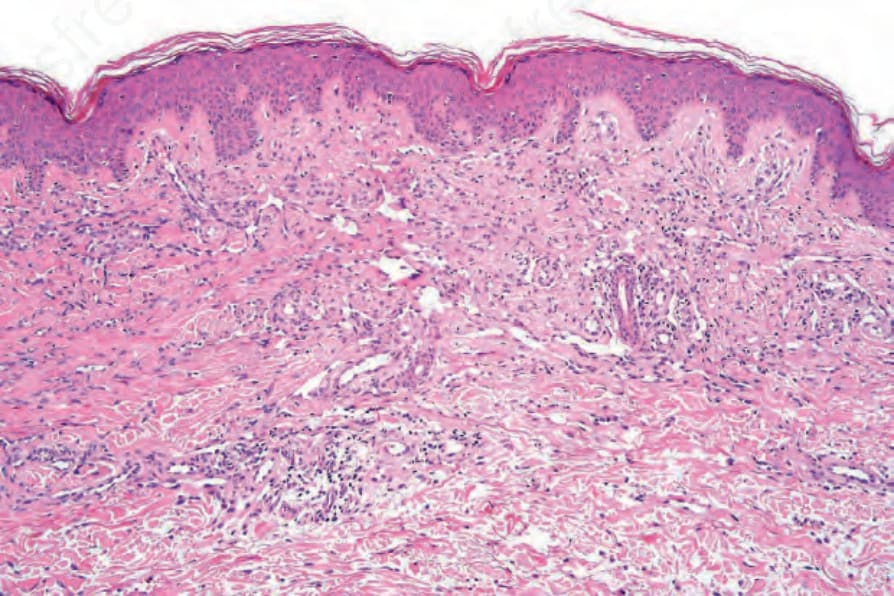
Fig. 35.535 Kaposi sarcoma (patch stage): there is increased vascularity, spindled cells and a light chronic inflammatory cell infiltrate.
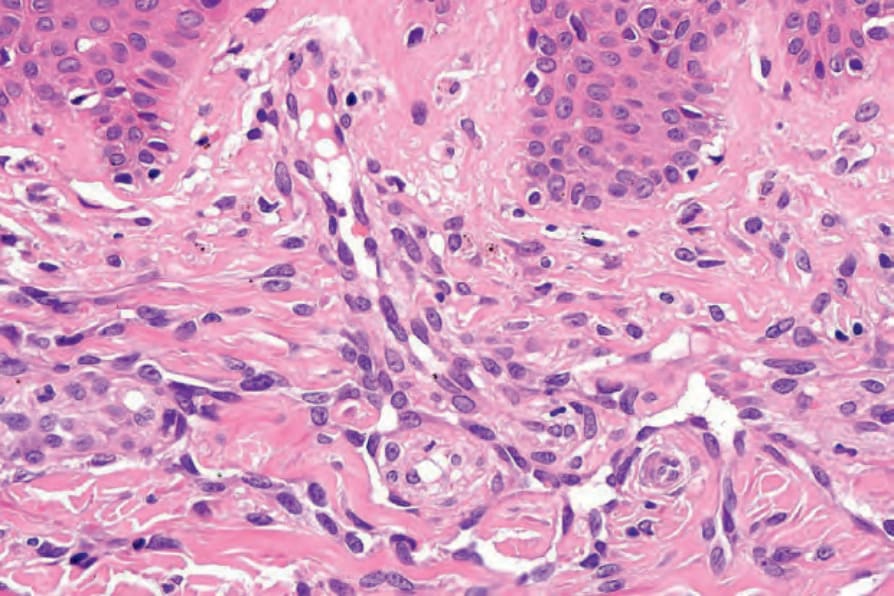
Fig. 35.536 Kaposi sarcoma (patch stage): the vessels are lined by swollen, focally hyperchromatic endothelial cells.
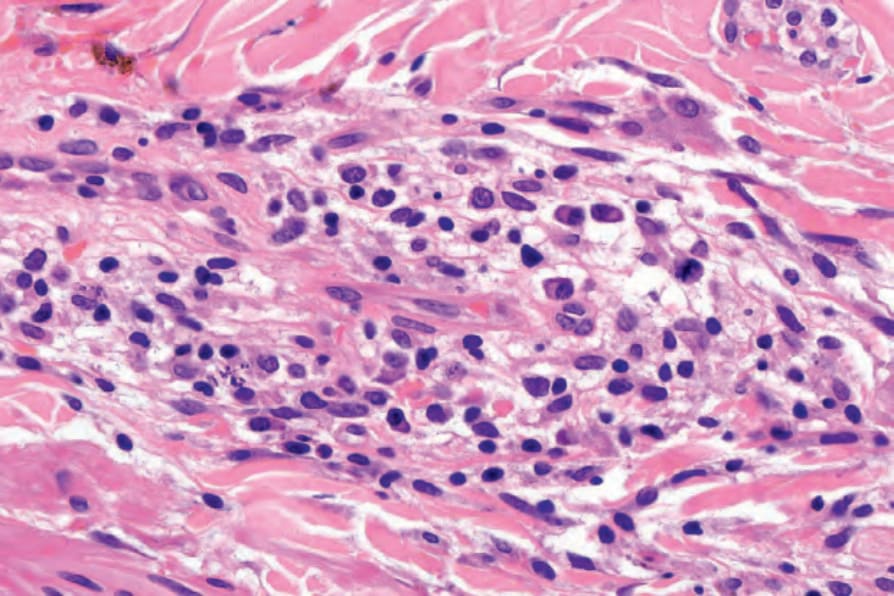
Fig. 35.537 Kaposi sarcoma (patch stage): the infiltrate consists of an admixture of lymphocytes and plasma cells.
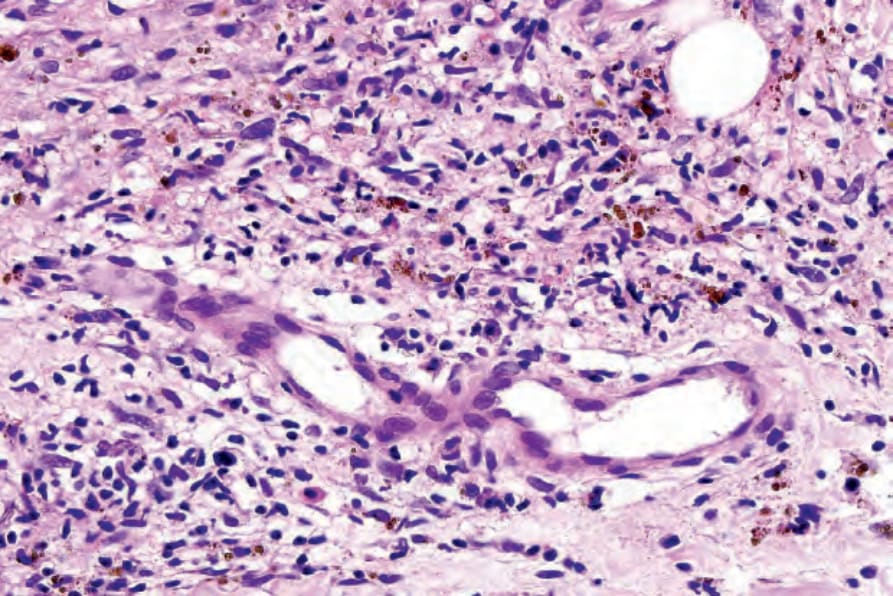
Fig. 35.538 Kaposi sarcoma (patch stage): focal hemosiderin deposition is present.
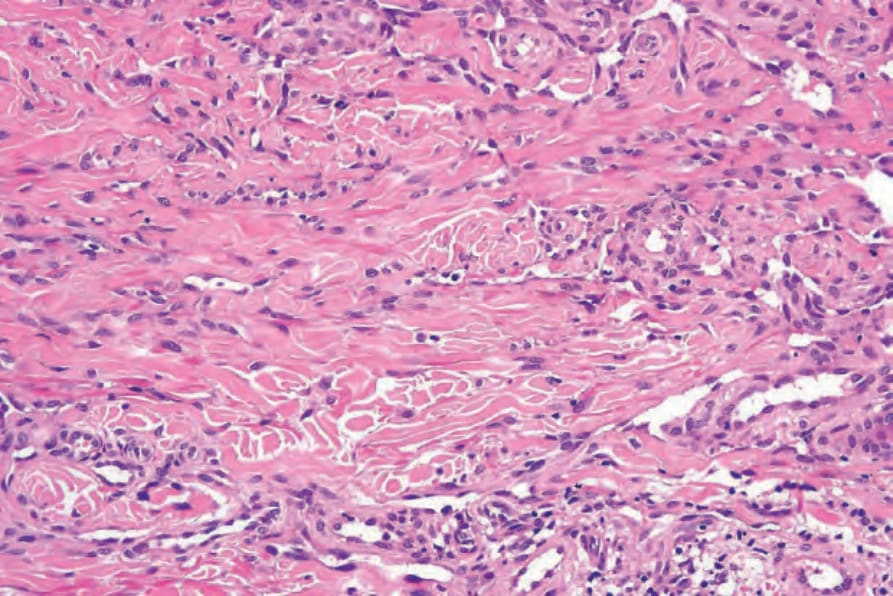
Fig. 35.539 Kaposi sarcoma (patch stage): this field shows extensive dissection of collagen (a characteristic feature).
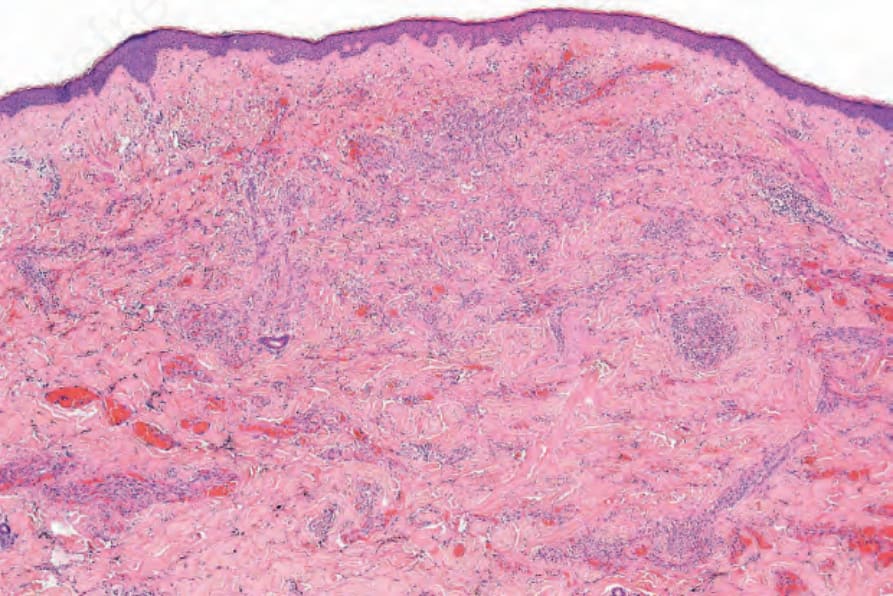
Fig. 35.540 Kaposi sarcoma (plaque stage): the changes affect the full thickness of the dermis.
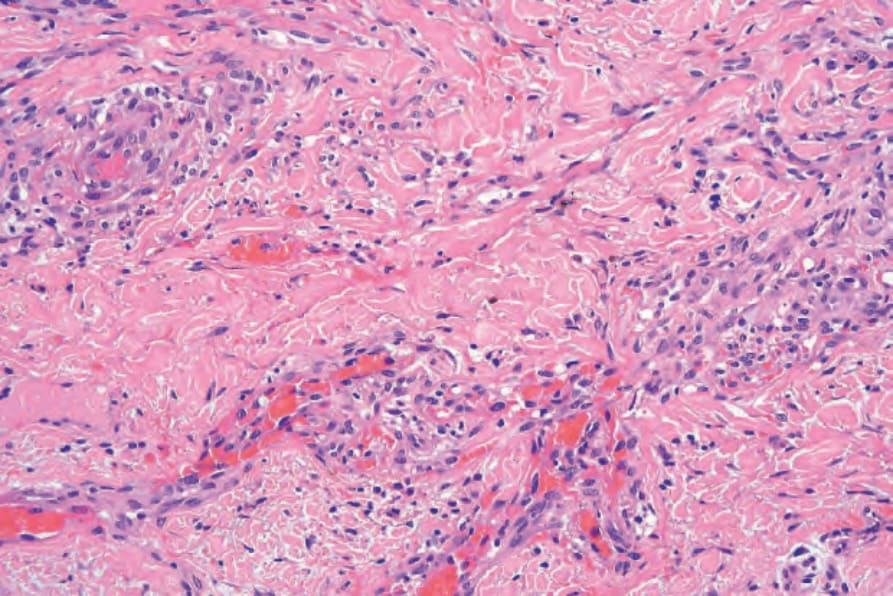
Fig. 35.541 Kaposi sarcoma (plaque stage): there is very extensive vascular proliferation.
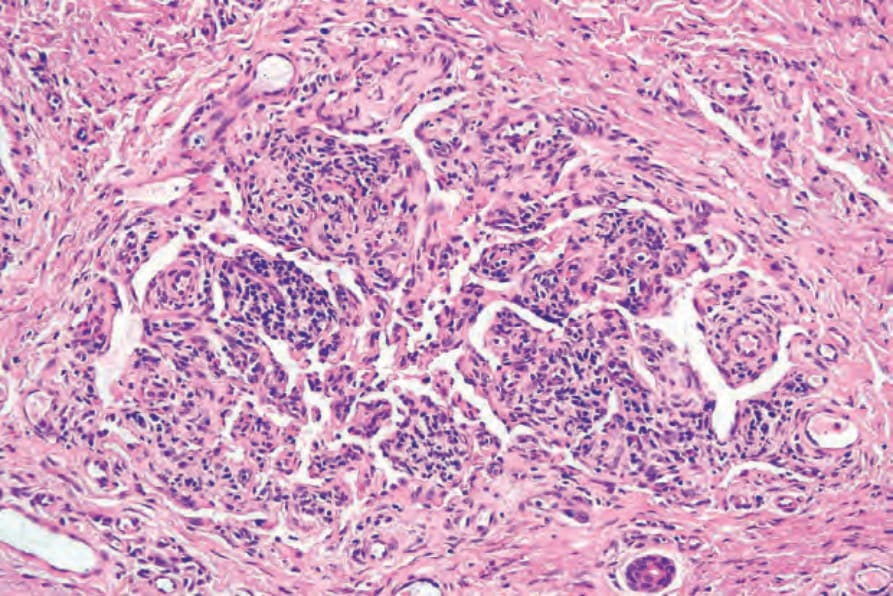
Fig. 35.542 Kaposi sarcoma: newly formed vessels sometimes ensheath pre-existent ones – the promontory sign.
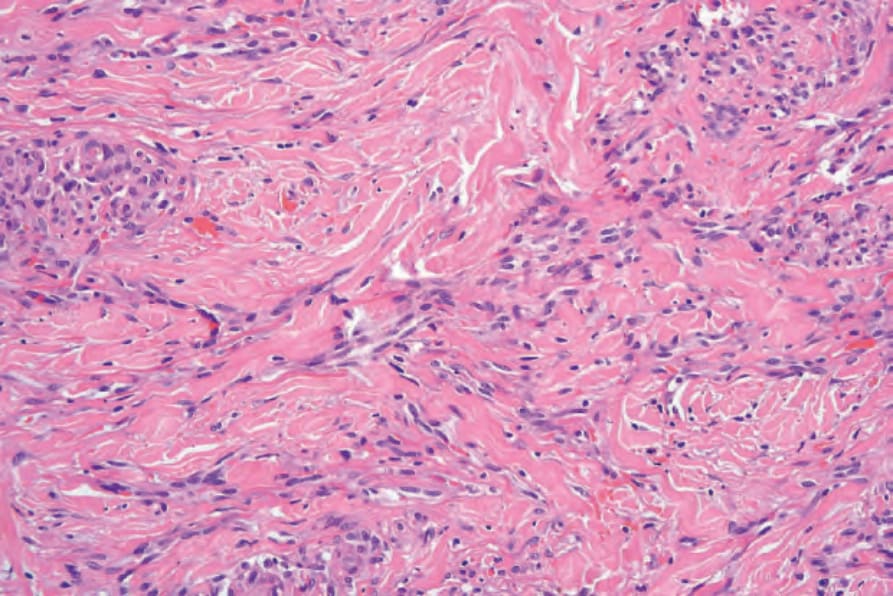
Fig. 35.543 Kaposi sarcoma (plaque stage): increased numbers of spindle cells are present. Dissection of collagen is marked.
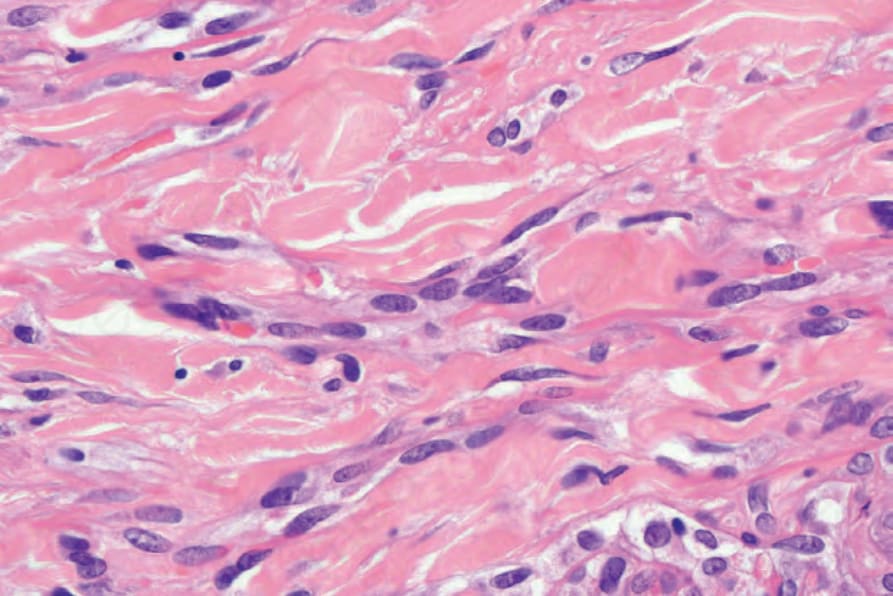
Fig. 35.544 Kaposi sarcoma (plaque stage): the spindle cells have pale eosinophilic cytoplasm with oval or elongated nuclei.
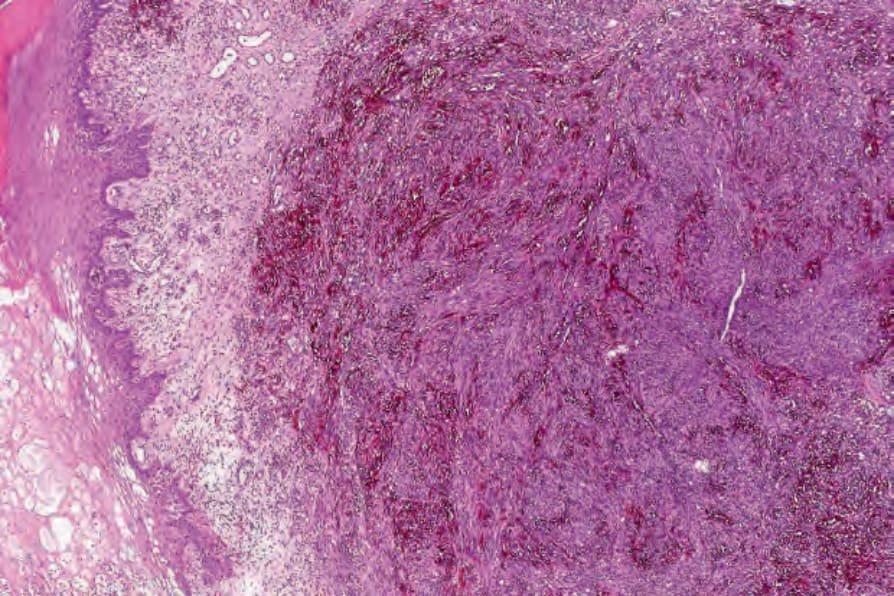
Fig. 35.545 Kaposi sarcoma (nodular stage): the dermis is diffusely infiltrated by a spindle cell tumor.
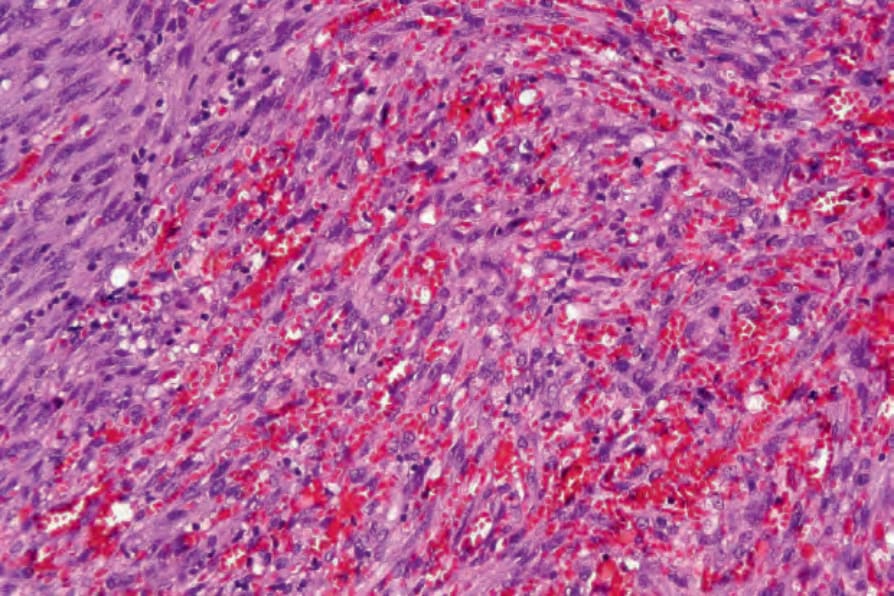
Fig. 35.546 Kaposi sarcoma: the spindled cells have eosinophilic cytoplasm. Hemorrhage is conspicuous.
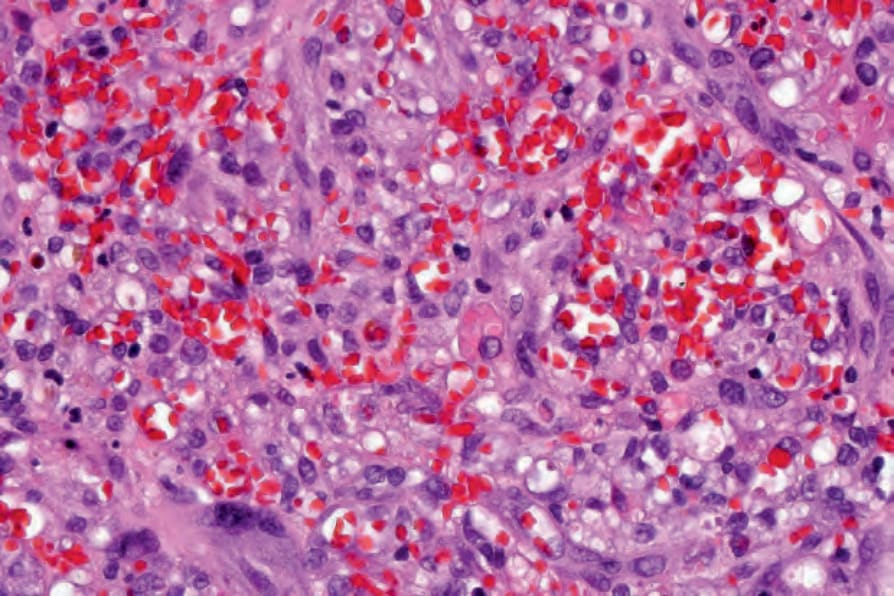
Fig. 35.547 Kaposi sarcoma (nodular stage): this sieve-like appearance is diagnostic.
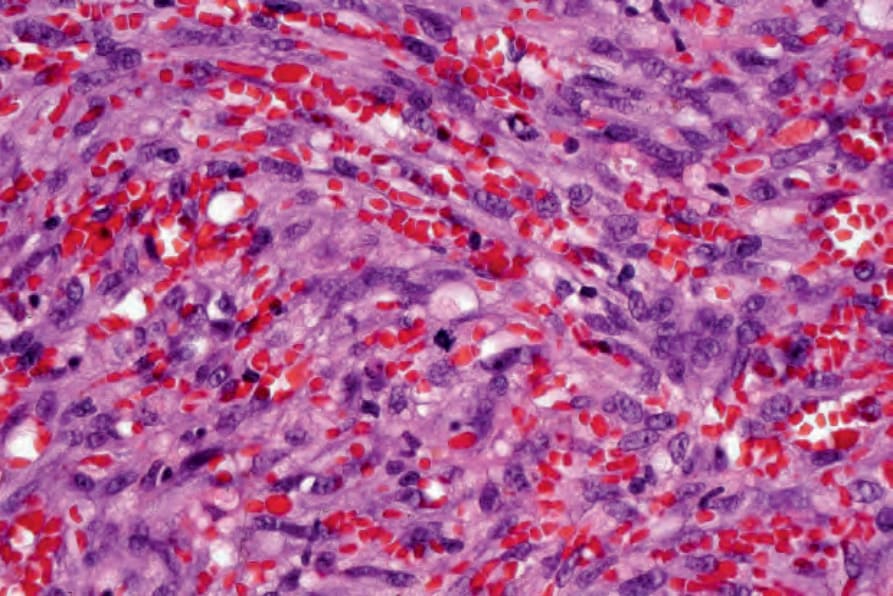
Fig. 35.548 Kaposi sarcoma (nodular stage): multiple mitoses are present.
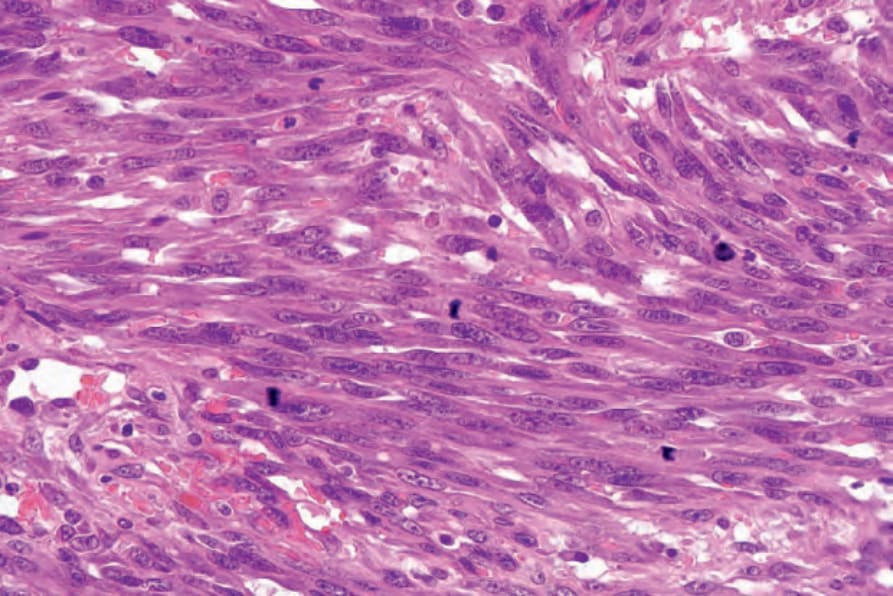
Fig. 35.549 Kaposi sarcoma: numerous mitoses are present in this predominantly spindled cell high-grade population.
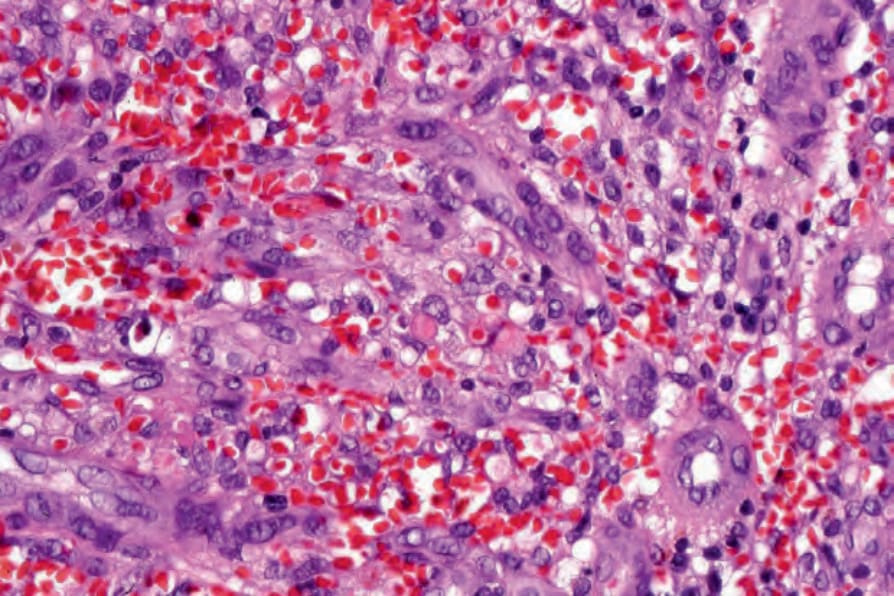
Fig. 35.550 Kaposi sarcoma: the presence of hyaline inclusions is a useful diagnostic marker.
It is important to remember that in patients with HIV/AIDS more than one pathology can be found in a single biopsy. Kaposi sarcoma has been reported in association with cryptococcosis and tuberculosis and cryptococcosis and Mycobacterium avium intracellulare in the same sample.64–66
After the discovery of HHV-8, demonstration of virus in skin biopsies from patients with Kaposi sarcoma was done by in situ hybridization. A monoclonal antibody against the latent nuclear antigen-1 of HHV-8 is routinely used in paraffin-embedded biopsies.67,68 This represents an invaluable tool in the histologic diagnosis of Kaposi sarcoma and its differential diagnosis as other vascular tumors are usually not positive for HHV-8 (Fig. 35.553). Exceptional cases of Kaposi sarcoma are negative for HHV-8 by immunohistochemistry and the diagnosis has to be confirmed by PCR.69 Genomic characterization of Kaposi sarcoma to demonstrate molecular derangements has not yet been published, but might help clarify some of the debate over its neoplastic status.
The vascular spaces in Kaposi sarcoma are positive for D2–40, suggesting a lymphatic lineage (Fig. 35.551).54,55
Also noted in all forms of Kaposi sarcoma, but especially in the nodular variant, is the presence of amorphous eosinophilic hyaline globules lying free between spindle cells or intracellularly. These probably represent degenerate red blood cells.56 They are diastase resistant and PAS positive, and stain bright red with Masson trichrome.
Differential diagnosis The differential diagnosis is wide and includes acroangiodermatitis, aneurysmal benign fibrous histiocytoma, progressive lymphangioma, tufted angioma, targetoid hemosiderotic hemangioma, spindle cell hemangioma, kaposiform hemangioendothelioma and angiosarcoma.27,70
In acroangiodermatitis, which most often affects the lower legs and complicates severe chronic venous stasis, there is proliferation of small normal capillaries in the superficial dermis associated with fibrosis, hemosiderin deposition and few inflammatory cells.71 Aneurysmal benign fibrous histiocytoma is a more polymorphic, focally storiform lesion in which foamy histiocytes and multinucleated cells are prominent. In angiosarcoma, endothelial cytologic atypia is more prominent and endothelial multilayering is present.
Lymphangiomatous Kaposi sarcoma is a variant of the patch–plaque stage in which moderately dilated vascular channels, resembling lymphatics, are prominent (Fig. 35.552).57,58 It may be mistaken for progressive lymphangioma.
In HIV patients with chronic lymphedema, additional histologic features include fibrosis, pools of lymph fluid and fibroma-like nodules.33 The latter may include Kaposi sarcoma spindle-shaped cells.
Anaplastic Kaposi sarcoma is very rare and characterized by cytologic atypia and variable mitotic activity.59 Epithelioid morphology can rarely be seen.60 Distinction from angiosarcoma is often very difficult and a helpful clue is the finding of areas typical of Kaposi sarcoma in the same sample. Many of the cases of anaplastic disease described before the advent of immunohistochemistry are probably examples of other sarcomas.
Unusual histologic variants of Kaposi sarcoma may be encountered including glomeruloid, pigmented, KS with myoid nodules, telangiectatic and ecchymotic.61
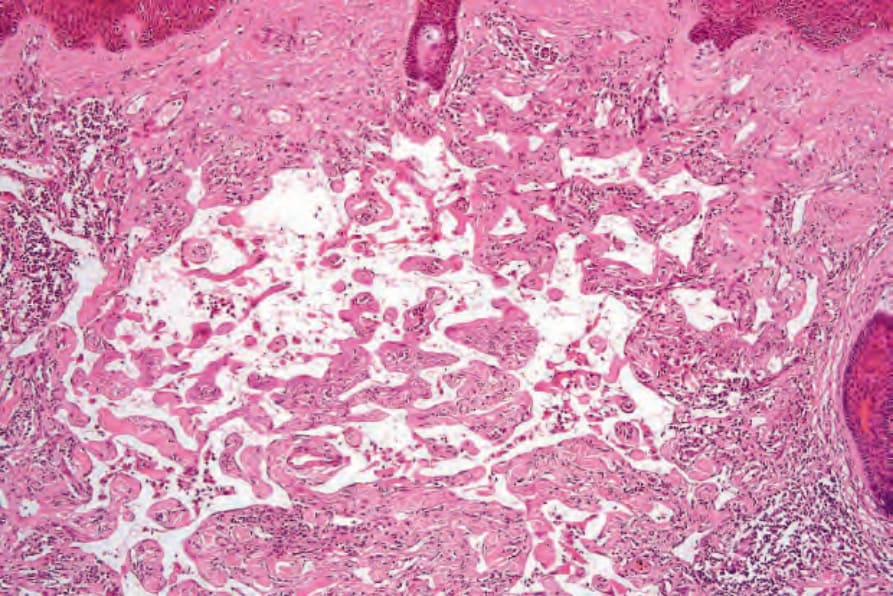
Fig. 35.552 Kaposi sarcoma: rarely, marked lymphatic dilatation gives rise to the lymphangiomatous variant.
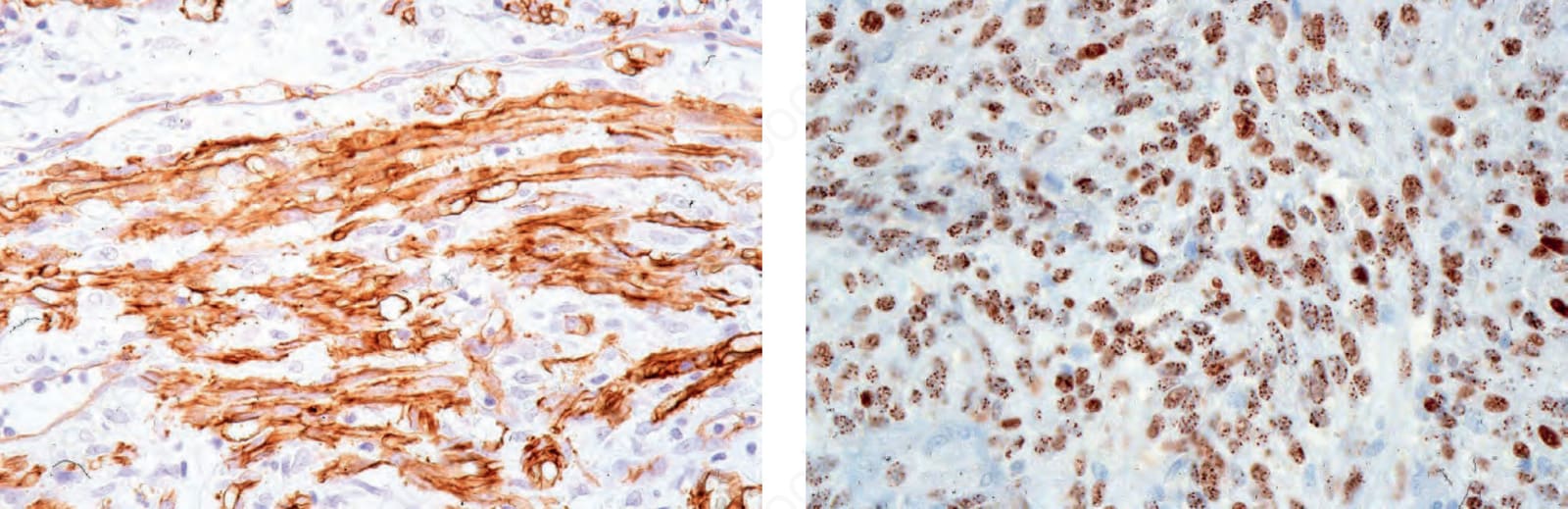
Fig. 35.553 Kaposi sarcoma: HHV-8 is regularly present.
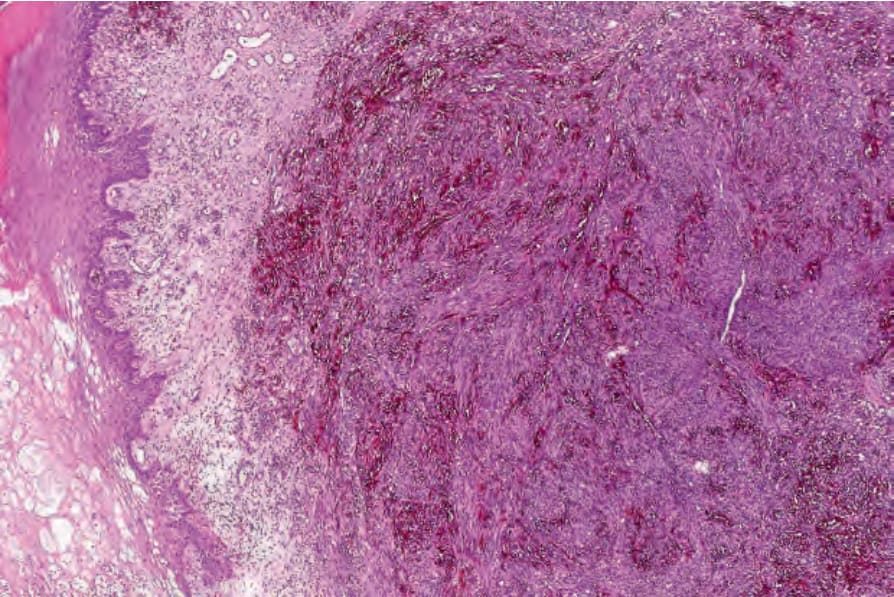
Fig. 35-551 (caption embedded in image / 圖說烘焙於圖內)