Microvenular hemangioma
Microvenular hemangioma
Pathogenesis and histologic features Based on immunohistochemical negativity for WT1 only it has been proposed that this lesion represents a superficial lymphatic malformation.12,13
Clinical features Microvenular hemangioma is an asymptomatic lesion that commonly presents on the limbs of young adults as a red–bluish papule, nodule or plaque.1–3 Multiple, sometimes numerous, lesions have been documented in a few patients.3–6 In a reported case, multiple bilateral macules, patches and plaques were described.7 Presentation in children is rare.8,9 A case positive for human herpesvirus-8 has been documented in the context of POEMS syndrome.10 Recurrence is exceptional.
Histologic features Histologically, it consists of irregular, branching, thin-walled venules lined by bland endothelial cells containing plump nuclei (Fig. 35.489). The tumor extends widely throughout the dermis, dissecting between somewhat hyalinized collagen bundles (Fig. 35.490). Infiltration of arrector pili muscles by vascular channels is a frequent finding. Each channel is surrounded by a
The most striking low-power feature is the presence of a wedge-shaped vascular proliferation with the base towards the epidermis. The vascular channels are irregular, thin-walled, dilated, and lined by endothelial cells with bland protruding nuclei and scanty cytoplasm (hobnail cells) (Figs 35.492 and 35.493). Focal papillary projections are a characteristic feature. As the lesion descends into the deep dermis, the vascular channels become less conspicuous, appear to dissect between collagen bundles, and are lined by more flattened endothelial cells. Extravasation of red blood cells and hemosiderin deposition can be prominent but this depends on the stage of the lesion. Inflammation is not usually a feature but scattered lymphocytes and plasma cells may sometimes be seen.
It is likely that this tumor represents the benign end of the spectrum of a group of lesions characterized by hobnail endothelial cells, including papillary intralymphatic angioendothelioma (PILA, Dabska tumor) and retiform
1838 Connective tissue tumors
A
B
hemangioendothelioma.14 Trauma may induce secondary changes similar to those seen in hobnail hemangioma.15
The endothelial cells in hobnail hemangioma stain diffusely for vascular markers including CD31 and ERG. CD34 is usually negative or only very focally positive. A layer of alpha-SMA–positive pericytes surrounds some of the vascular channels. Despite the changes associated with the menstrual cycle, endothelial cells are negative for estrogen and progesterone receptors.9 The positive staining for vascular endothelial growth factor receptor 3 (VEGFR-3) and D2-40 has led to the suggestion that hobnail hemangioma displays lymphatic differentiation.4,12,13,16 VEGFR-3 is, however, not entirely specific for lymphatic endothelium. Staining for HHV-8 is consistently negative.17
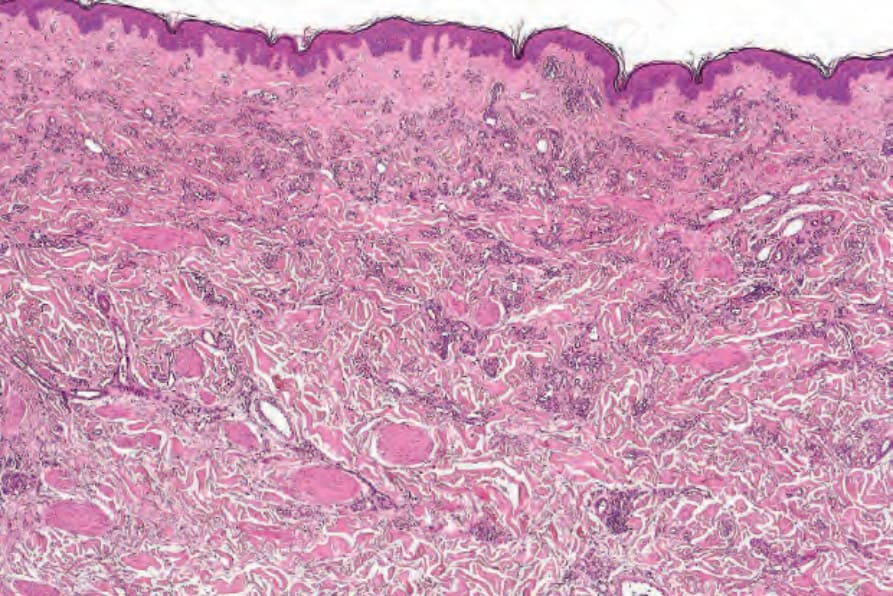
Fig. 35.489 Microvenular hemangioma: the manner in which the vessels irregularly infiltrate the dermis is sometimes mistaken for Kaposi sarcoma.
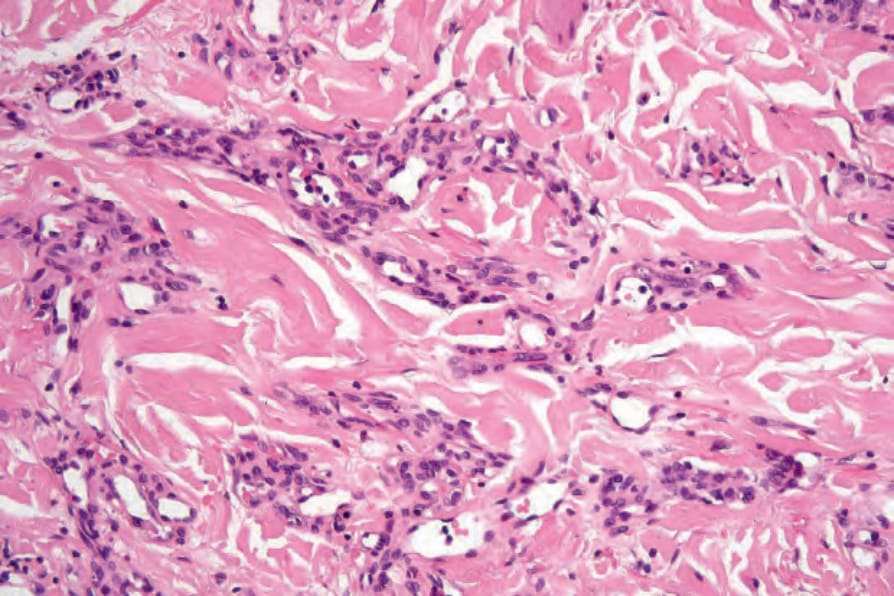
Fig. 35.490 Microvenular hemangioma: the ramifying vessels are lined by a plump endothelial monolayer and an outer layer of more spindled pericytes.

Fig. 35.491 Hobnail hemangioma: this example shows the characteristic targetoid appearance.
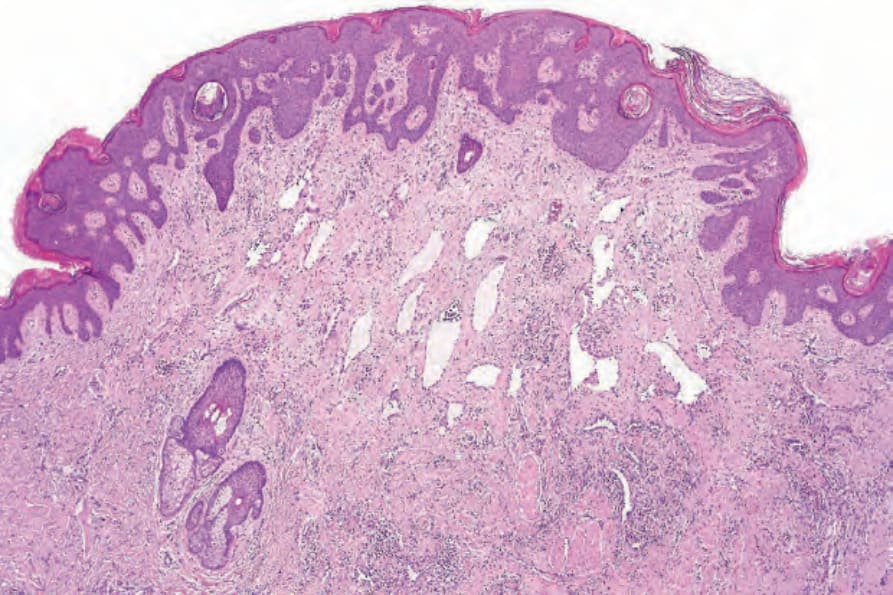
Fig. 35.492 Hobnail hemangioma: thin-walled vascular channels are present in the superficial dermis. The growth pattern is wedge shaped.
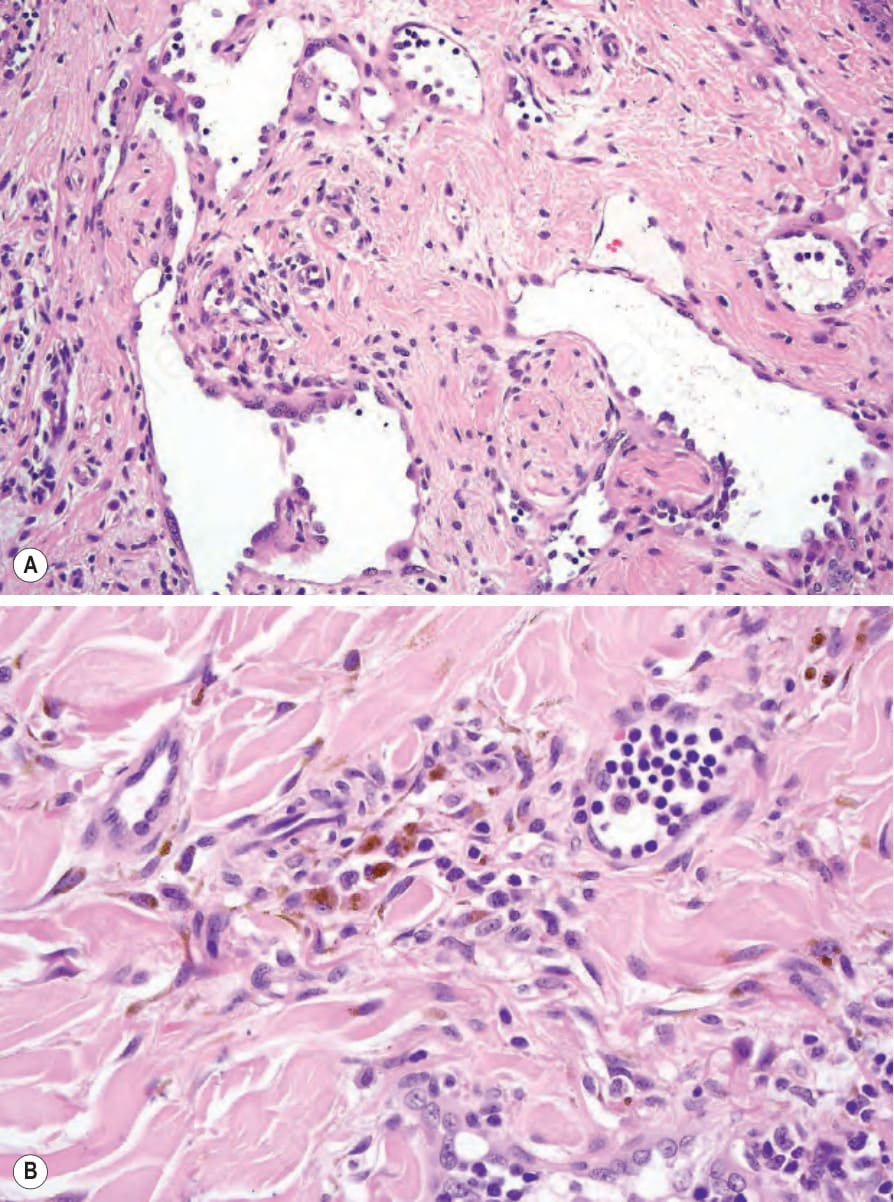
Fig. 35.493 Hobnail hemangioma: (A) the endothelial cells are prominent and protrude into the lumen. Note the papillary processes; (B) there is abundant hemosiderin pigment.