Lobular capillary hemangioma (pyogenic granuloma)
Lobular capillary hemangioma (pyogenic granuloma)
Clinical features Lobular capillary hemangioma (pyogenic granuloma) is a very common benign vascular lesion that was regarded for many years as a reactive or infective process.1 This assumption was based on the extensive secondary changes that are almost invariably present in these lesions. However, the underlying process is that of a lobular proliferation of capillaries, which is much more likely to be neoplastic, and therefore it has been redesignated lobular capillary hemangioma.2 It may arise at any age in either sex and shows a predilection for the head and neck (especially the mucous membranes) and limbs (particularly the arms and hands) (Fig. 35.470). Oral lesions are more common in females.3,4 Lobular capillary hemangioma also occurs in the gastrointestinal tract and other organs. Typically, the lesion evolves rapidly, reaching its maximum size (usually less than 2 cm in diameter) within a matter of months. It presents as a pedunculated red or bluish nodule, which is prone to ulceration or bleeding (Fig. 35.471).5 Complete spontaneous regression does not occur and rare patients present with multiple lesions, either disseminated or localized.6–10 Eruptive lesions have been described following a drug hypersensitivity reaction, a landmine injury, burns and associated with an acquired arteriovenous malformation.11–13 Congenital lesions are exceptional and one case presented with disseminated lesions.14–17 Lesions may occur within a port-wine stain and more rarely in association with unilateral dermatomal superficial telangiectasia.18–21 Multiple pyogenic granuloma-like lesions have been documented in association with BRAF inhibitors, capecitabine, topical tretinoin, isotretinoin, gefitinib, afatinib, 5-fluorouracil, levothyroxine, EGFR tyrosine kinase inhibitors, and
anti-TNF-alpha therapy.22–32 In one case an association with erythropoietin was suggested.33 Subungual lesions may occur not only in association with drugs and trauma but also after peripheral nerve injury.34 Lobular capillary hemangiomas have also been documented as a complication of pulse dye laser used to treat port-wine stains, following orbital hydroxyapatite implants,35,37 after bone marrow transplant38 and in a patient with NF1 and von Hippel-Lindau syndrome.39
Local recurrence after excision is relatively frequent and in a small proportion of cases there is a recurrence with multiple satellite lesions that may be clinically worrying (Fig. 35.472).39,40 This latter phenomenon tends to occur in younger individuals who very often have primary lesions on the trunk.
• Granuloma gravidarum is a variant that presents on the gingivae of pregnant women and involutes after delivery. Pregnancy may also induce lesions elsewhere.41,42
1833 Capillary hemangioma and its variants
• Subcutaneous or deep dermal lobular capillary hemangioma has a predilection for the upper limb.43,44 Since it never becomes ulcerated, it is not associated with secondary inflammatory changes.
• Intravenous lobular capillary hemangioma is uncommon, but tends to occur on the neck and upper extremity of young adults.45–47
Histologic features Lobular capillary hemangioma consists of a usually exophytic, lobulated, dermal mass made up of numerous small capillaries, often radiating from larger, more central vessels set in a loose edematous collagenous matrix (Figs 35.473 and 35.474). Endothelial cells have variably bland to plump nuclei and may be focally epithelioid, especially in mucosal tumors.48 Mitoses are commonly present and may be numerous (Fig. 35.475). Focal cytologic atypia as a result of degeneration may be seen (Figs 35.476 and 35.477). Metaplastic ossification is sometimes seen and extramedullary hematopoiesis has exceptionally been documented.49,50
1834 Connective tissue tumors
Superficial infiltration by acute and chronic inflammatory cells in large numbers is a common finding, but this is seen only in ulcerated lesions. In such instances, the adjacent epidermis is often acanthotic and tends to form a well-defined collarette. When inflammation is marked, the overall features show a close resemblance to granulation tissue, except for the presence of capillary lobules in the deeper dermis at the base of the lesion.
rarely in other immunosuppressed hosts or exceptionally in normal individuals. Although both lesions are architecturally very similar, bacillary angiomatosis is composed of pale eosinophilic endothelial cells and shows polymorphs throughout the lesion, accentuated in the vicinity of basophilic granular aggregates. The latter, when stained with Giemsa or Warthin-Starry, show clumps of short bacilli. The bacilli may also be demonstrated by immunohistochemistry.
Those cases developing satellite lesions often show extension into the subcutaneous fat.
Intravenous lobular capillary hemangioma is histologically similar to the more conventional lesion except that it lacks a significant inflammatory component (Figs 35.478 and 35.479).
Human papillomavirus type 2 has been found in some cases of lobular capillary hemangioma suggesting a possible etiological link.51,52 RAS and BRAF mutations, particularly BRAF V600E, have been found in sporadic and lobular capillary hemangiomas associated with port-wine stains, suggesting a possible role of the RAS / ERK pathway in their pathogenesis.52–54
Differential diagnosis The most important differential diagnosis is bacillary angiomatosis, an infectious vascular proliferation caused by a rickettsial organism Rochalimaea henselae.55–57 The latter occurs mainly in patients with AIDS and
Lobular capillary hemangioma may sometimes need to be distinguished clinically from other types of capillary hemangioma. Mucosal lesions with very plump endothelial cells and a high mitotic rate may be readily distinguished from angiosarcoma by their lobular architecture.

Fig. 35.470 Lobular capillary hemangioma: a typical raised red nodule on the face of a young female patient. By courtesy of M.M. Black, MD, St Thomas’ Hospital, London, UK.

Fig. 35.471 Lobular capillary hemangioma: these lesions are characteristically ulcerated. By courtesy of the Institute of Dermatology, London, UK.

Fig. 35.472 Lobular capillary hemangioma (satellitosis): characteristic appearance of multiple satellite lesions on the trunk. By courtesy of E. Wilson Jones, MD, Institute of Dermatology, London, UK.
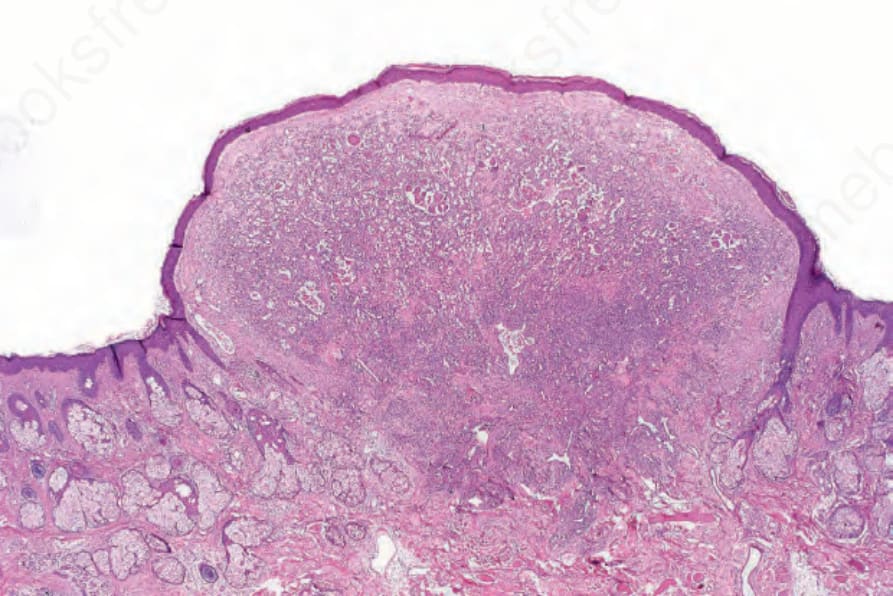
Fig. 35.473 Lobular capillary hemangioma: this scanning section shows the polypoid structure of the lesion and the well-formed collarette.
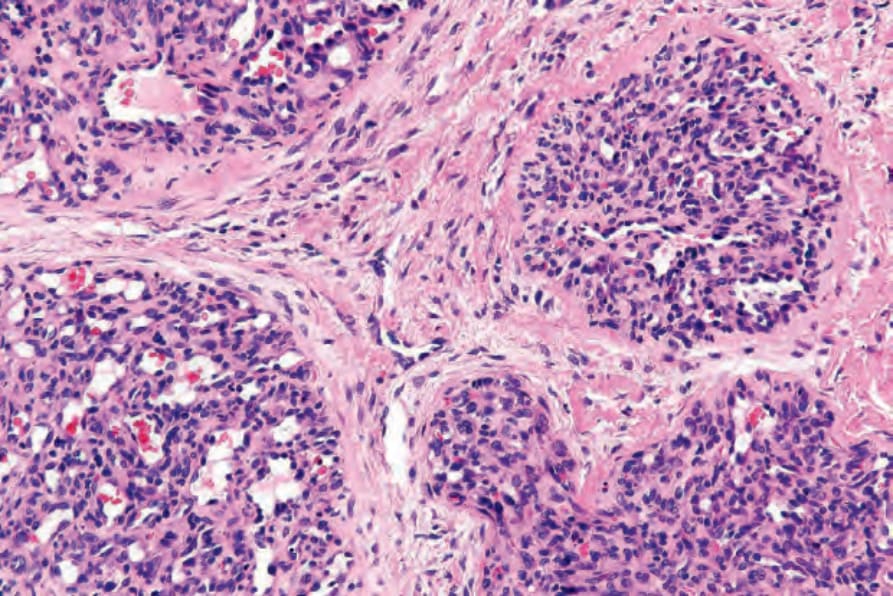
Fig. 35.474 Lobular capillary hemangioma: note the well-developed lobular architecture.
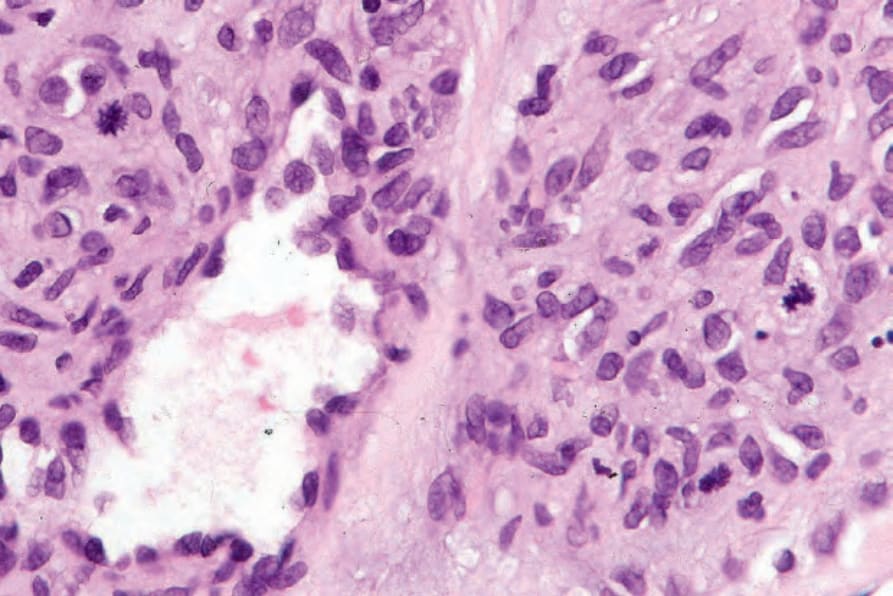
Fig. 35.475 Lobular capillary hemangioma: conspicuous mitotic activity is often present, particularly in evolving lesions.
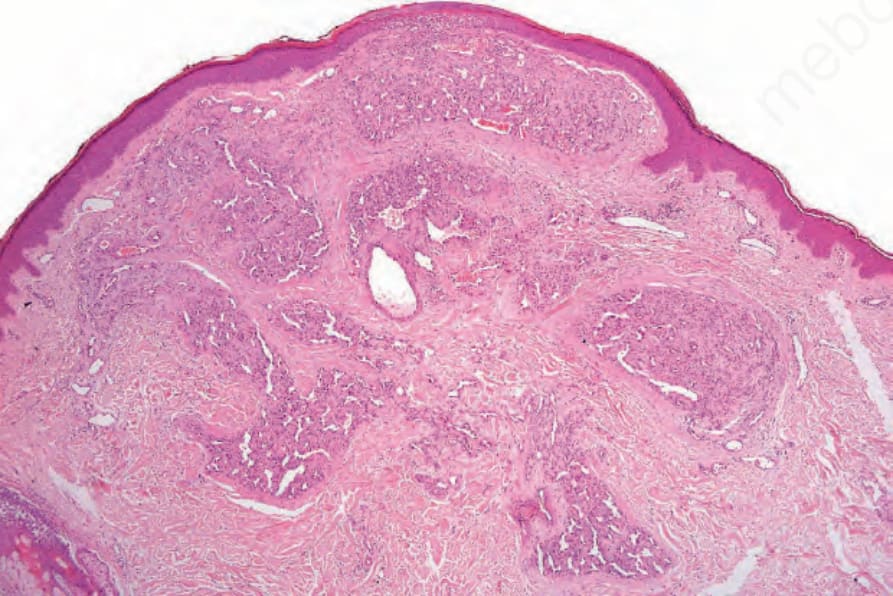
Fig. 35.476 Lobular capillary hemangioma with atypia: scanning view showing multiple lobules with an associated fibrous stroma.
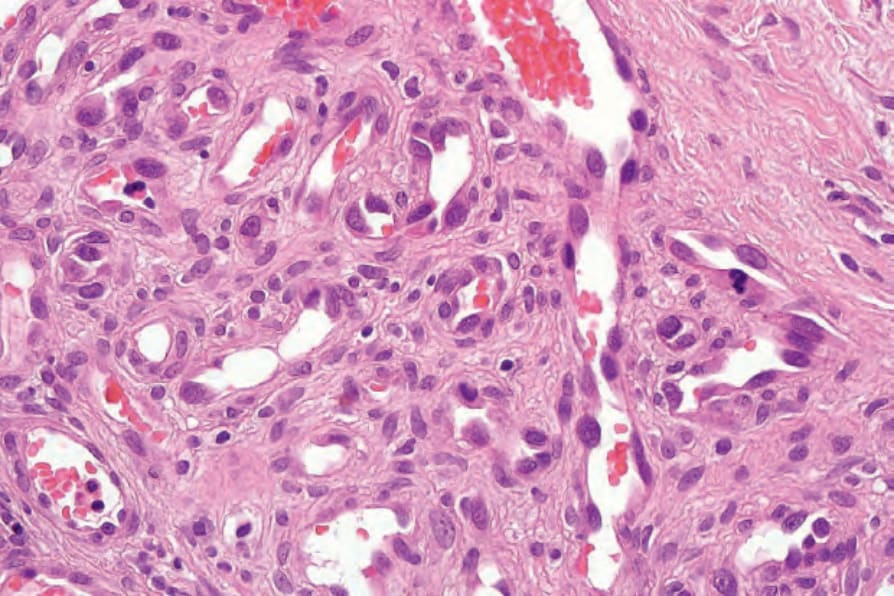
Fig. 35.477 Lobular capillary hemangioma with atypia: there is nuclear pleomorphism and an atypical mitosis is present.
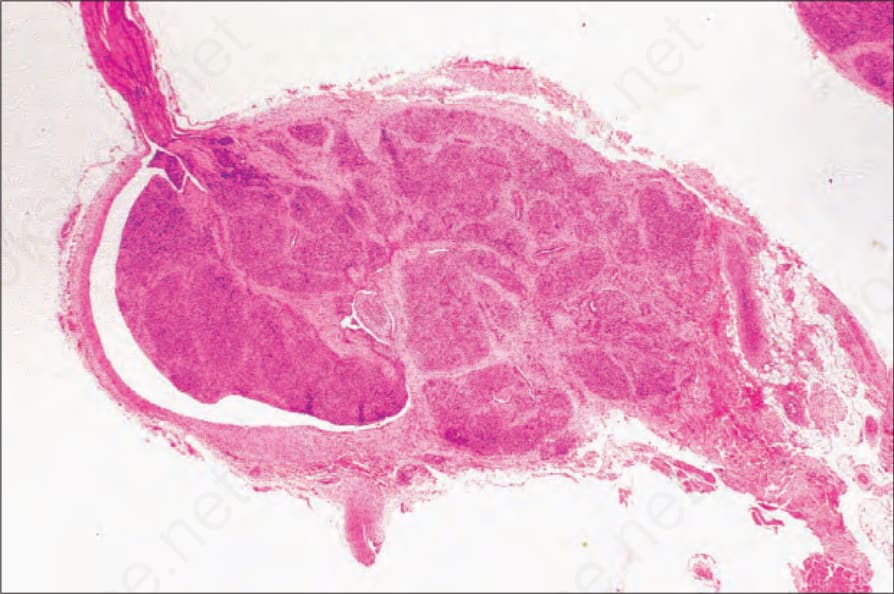
Fig. 35.478 Intravascular lobular capillary hemangioma: this is a rare lesion. Note the thin vessel wall and prominent lobularity.
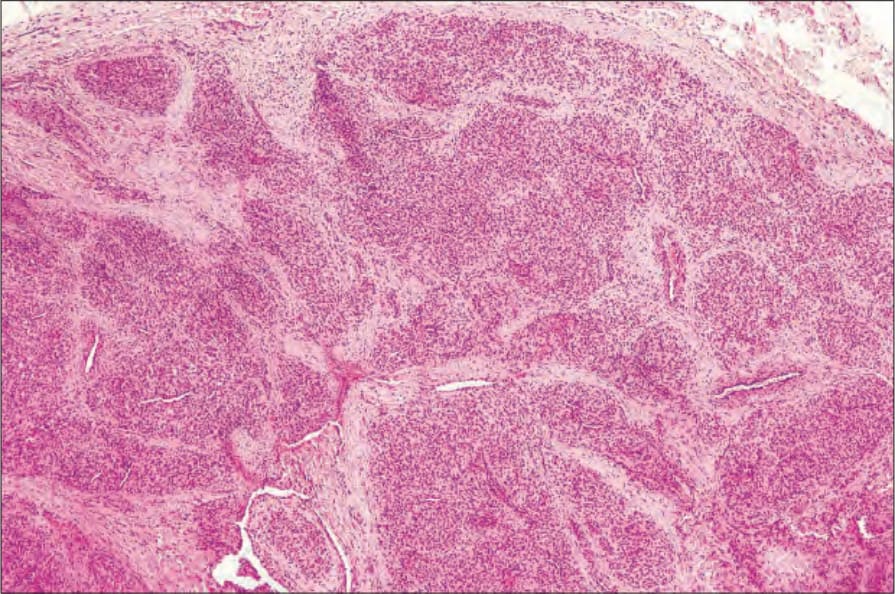
Fig. 35.479 Intravascular lobular capillary hemangioma: higher-power view showing the vascular lobules.

Fig. 35.480 Tufted angioma: lesions commonly present on the neck and upper trunk. Note the presence of extensive macules and plaque-like lesions. By courtesy of the Institute of Dermatology, London, UK.