Non-involuting congenital hemangioma (NICH)
Non-involuting congenital hemangioma (NICH)
Clinical features Non-involuting congenital hemangioma is fully developed at birth but does not regress; rather it tends to progress over time. Males and females are equally affected. Anatomical distribution is wide, but there is predilection for the head and limbs.3
Histologic features Infantile hemangiomas have a fairly uniform microscopic appearance characterized by an intradermal or subcutaneous multilobular proliferation of numerous small vascular spaces lined by plump endothelial cells, which may be mitotically active (Figs 35.467 and 35.468). In the early stages, vascular lumina tend to be inconspicuous and the vascular nature of the tumor might not be immediately apparent. However, a reticulin stain highlights the presence of numerous poorly canalized vascular channels. With maturation, the vessels enlarge and dilate and the endothelium appears more flattened and mature. At the deep margin of the lesion a large feeding arteriole is often apparent. An occasional entirely benign feature is the presence of perineural invasion.5,6 Older lesions become progressively more fibrotic, showing a gradual disappearance of the vascular elements, and histologic diagnosis of largely regressed examples can be difficult.
1831 Capillary hemangioma and its variants
By immunohistochemistry and electron microscopy it has been demonstrated that the tumor cell population is heterogeneous and composed not only of endothelial cells but also of fibroblasts and pericytes.7,8 This favors a hamartomatous process rather than a true neoplasm. It has a unique immunophenotype shared with placental microvessels expressing GLUT-1, LeY and WT-1.9 GLUT-1, the erythrocyte-type glucose transporter protein, is expressed by these hemangiomas at all stages of their evolution.9,10 Since GLUT-1 and WT-1 are not expressed in other vascular tumors which occur in children, the presence of this marker is a valuable aid in differential diagnosis, particularly in the setting of vascular malformations.11,12 Endothelial cells in proliferating lesions co-express LYVE-1 and CD34 and are negative for Prox-1, while LYVE-1 is negative in involuting lesions, suggesting that endothelial cells in proliferating infantile hemangiomas are arrested early in the developmental stage of vascular differentiation.13. In addition, capillary hemangiomas have been shown to be clonal.14,15
Differential diagnosis The differential diagnosis with congenital hemangiomas is discussed under the latter.
Infantile hemangiomas with minimal or arrested growth (abortive hemangiomas)
Clinical features These recently described lesions are characterized by telangiectatic patches with peripheral papules and predilection for the lower body.1–3 They are defined as vascular lesions with a proliferative component equal to or less than 25% of the total surface of the lesion.1 Slightly less than 50% of patients have typical infantile hemangiomas elsewhere.1 Lesions tend to persist.
Histologic features A biopsy from the telangiectatic patch shows scattered dilated vascular channels in the superficial dermis. In the deep dermis, lobules of capillaries may be seen. A biopsy from a papule shows features of a capillary hemangioma. Endothelial cells are positive for GLUT-1. This feature, and the coexistence with typical infantile hemangiomas, confirms that they are closely related.

Fig. 35.465 Infantile hemangioma: multiple raised erythematous nodules are present around this child’s ear and neck. By courtesy of J. Dayrit, MD, Manila, The Philippines.

Fig. 35.466 Infantile hemangioma: two raised nodules are present on the forehead of this female infant. By courtesy of M.M. Black, MD., The Institute of Dermatology, London, UK.
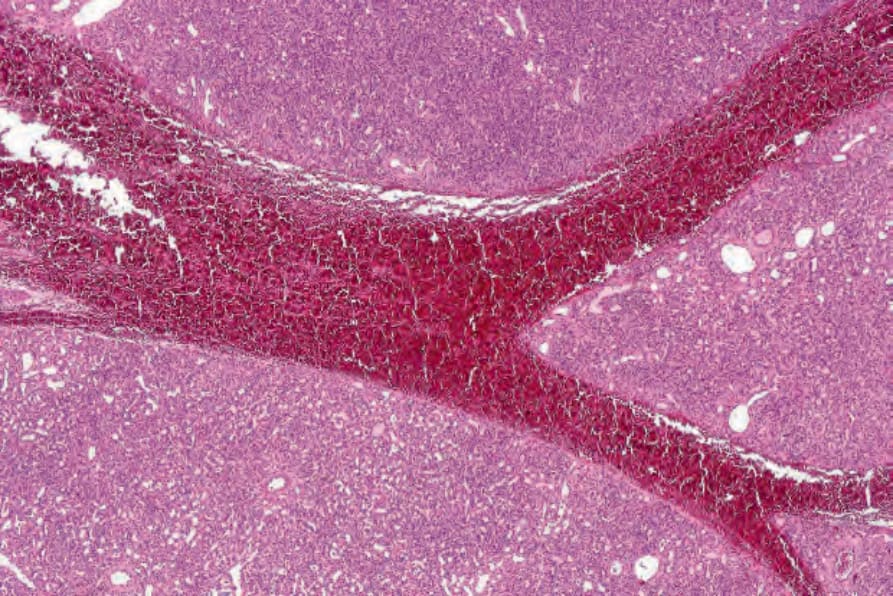
Fig. 35.467 Infantile hemangioma: this is an evolving lesion composed of lobulated aggregates of poorly canalized blood vessels.
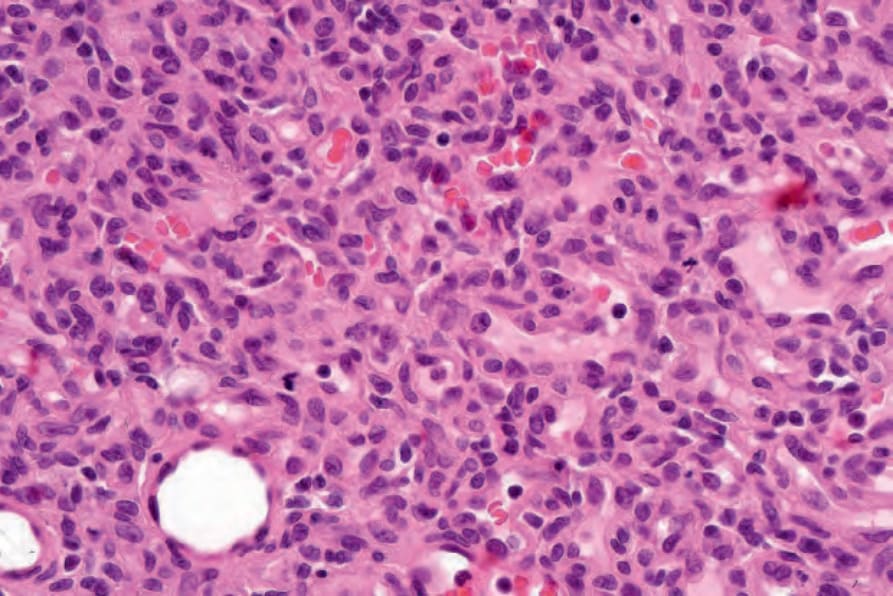
Fig. 35.468 Infantile hemangioma: the blood vessels are lined by plump endothelial cells. Note the multiple mitoses.