Congenital hemangiomas
Congenital hemangiomas
The term congenital hemangioma is used to describe a group of hemangiomas that develop in-utero and are fully developed at birth presenting with an equal sex incidence.1–5 These lesions were classified in the past as infantile hemangiomas, vascular malformations and cavernous hemangiomas. There is overlap with the latter entities and the concept of congenital hemangiomas is still evolving.
Congenital hemangiomas have been divided into rapidly involuting congenital hemangioma (RICH) and non-involuting congenital hemangioma (NICH).2,3 Although they seem to represent distinctive clinicopathological entities, there is some degree of overlap not only between RICH and NICH but also between RICH and infantile hemangioma and they may be part of the same spectrum. This means that accurate diagnosis usually relies on
1830 Connective tissue tumors
Histologic features The histologic features between RICH and NICH overlap. Microscopic distinction is often not possible on histologic grounds and therefore clinicopathological correlation is crucial to reach the diagnosis. Non-involuting congenital hemangioma is characterized by vascular lobules of variable size and often composed of capillaries and larger, sometimes thicker, blood vessels. Draining larger blood vessels are present in tumor lobules. Surrounding the latter, there are areas of fibrosis containing large blood vessels with features of veins and arteries. Arteriovenous fistulae are common and this closely mimics an arteriovenous malformation. Histologic distinction can be very difficult and close clinicopathological correlation is often necessary. As opposed to vascular malformations, NICH does not tend to recur. GLUT-1 staining is usually negative.
Differential diagnosis Infantile hemangioma is the main differential diagnosis. Infantile hemangioma typically develops shortly after birth, grows rapidly during the first year of life and tends to involute over a period of several years. The vascular lobules of RICH and infantile hemangioma are often identical and it has been proposed that distinction between both is mainly based in the presence of bands of fibrosis around tumor lobules and lack of GLUT-1 positivity in the former. In practice, however, and especially in small biopsies, distinction may be very difficult or impossible. Clinicopathological correlation is paramount. Distinction between infantile hemangioma and NICH is easier, as the latter tends to display more variability in the size of vascular channels, GLUT-1 staining is usually negative and arteriovenous fistulae are identified. The main problem with NICH, RICH and infantile hemangioma is that there is some degree of overlap between the three entities as demonstrated by the fact that infantile hemangioma may coexist with either RICH or NICH. The problem is further compounded by the fact that some cases of RICH fail to involute completely and behave more like NICH, and in such cases the histologic appearances overlap with those of RICH and NICH. At present, the pathogenetic relation between these groups of lesions remains obscure.
close clinicopathological correlation. It is likely that these lesions are pathogenetically interconnected. In both types of congenital hemangiomas mutations in GNAQ and GNA11 have been identified.6
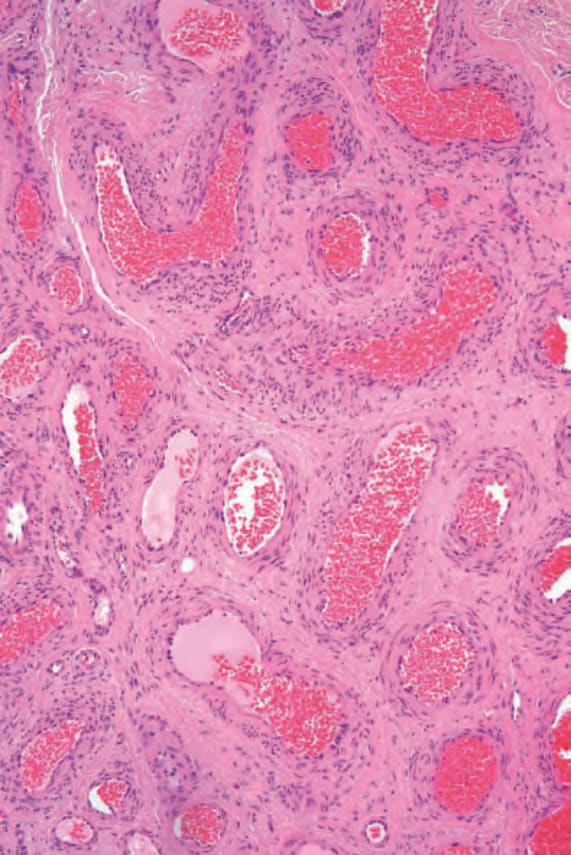
Fig. 35.464 Arteriovenous hemangioma: higherpower view showing admixture of arteries and veins.