Reactive angioendotheliomatosis
Reactive angioendotheliomatosis
Clinical features
For many years, angioendotheliomatosis was divided into benign and malignant variants, which were difficult to separate on clinical and histologic grounds.1 With the advent of immunohistochemistry, it became apparent that the malignant type is not endothelial in nature, but is an aggressive form of systemic angiotropic lymphoma. The benign variant of reactive angioendotheliomatosis is uncommon, purely cutaneous and self-limited. It presents as erythematous macules, papules or plaques, which can occasionally be purpuric (Fig. 35.445).1,2 Ulceration may be seen. A livedo-like pattern is sometimes observed. Anatomical distribution and age range are wide and there is no sex predilection. Presentation in children is very rare.3
Histologic features Lesions are located mainly in the dermis with occasional extension into the subcutis. They consist of a multifocal, variably lobular proliferation of closely packed capillaries lined by plump endothelial cells and surrounded by pericytes (Fig. 35.446). Cytologic atypia is absent or mild and frequently the vessel lumina are obliterated by plump endothelial cells. Cases related to cryoglobulinemia show capillaries occluded by hyaline eosinophilic thrombi. In diffuse dermal angiomatosis there is proliferation of poorly canalized capillaries and endothelial cells. This proliferation may involve the whole dermis and extend into the subcutaneous tissue in a diffuse manner.
Some cases are related to systemic infections, especially bacterial endocarditis, but this association is not as strong as was previously believed. Associations with cryoglobulinemia, paraproteinemia, renal disease, amyloidosis, antiphospholipid syndrome, rheumatoid arthritis, cirrhosis, polymyalgia rheumatica, myelodysplastic syndrome, a well-differentiated angiosarcoma and the administration of certain drugs have also been documented.2,4–13 A case of reactive angioendotheliomatosis associated with myelodysplastic
It has been suggested that intralymphatic histiocytosis and reactive angioendotheliomatosis are part of the same spectrum.25,32 The former, however, is mainly seen in patients with rheumatoid arthritis, can be an incidental finding in skin biopsies of patients with various pathologies and is characterized by dilated lymphatics containing numerous histiocytes.33–35 It does appear however, that the so-called intracapillary histiocytosis is better classified within the spectrum of reactive angoendotheliomatosis.35
Differential diagnosis On scanning magnification, reactive angioendotheliomatosis can mimic tufted angioma. However, the clinical presentation of both conditions is different and closer histologic examination reveals the typical tufts of capillaries with a crescent-like lymphatic channel in the periphery in tufted angioma. Diffuse dermal angiomatosis may mimic angiosarcoma. In the former, although endothelial cells appear plump there is hardly any cytologic
1824 Connective tissue tumors
larger cells with vacuolated cytoplasm and PAS-positive hyaline globules (representing immunoglobulin) are sometimes seen. By electron microscopy, the inclusions appear to represent enlarged secondary lysosomes (thanatosomes).13 Two types of endothelial cell with different immunophenotype have been described in glomeruloid hemangioma.14 The endothelial cells express endothelial growth factor and its receptor.15
Human herpesvirus 8 (HHV-8) is not present in the lesions of glomeruloid hemangioma.16
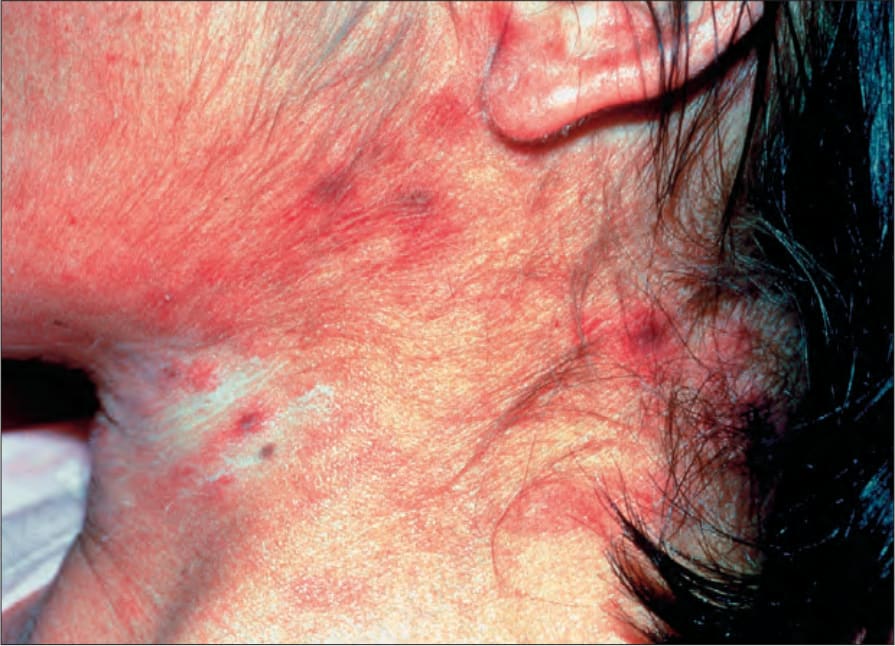
Fig. 35.445 Reactive angioendotheliomatosis: note the purpuric macular and papular lesions. By courtesy of the Institute of Dermatology, London, UK.
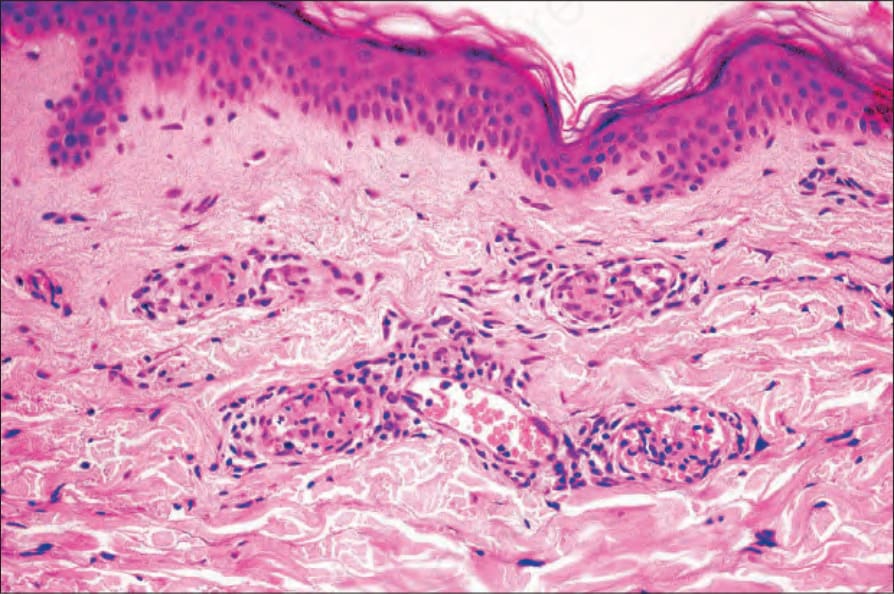
Fig. 35.446 Reactive angioendotheliomatosis: the dermis is extensively infiltrated by welldefined capillary lobules.
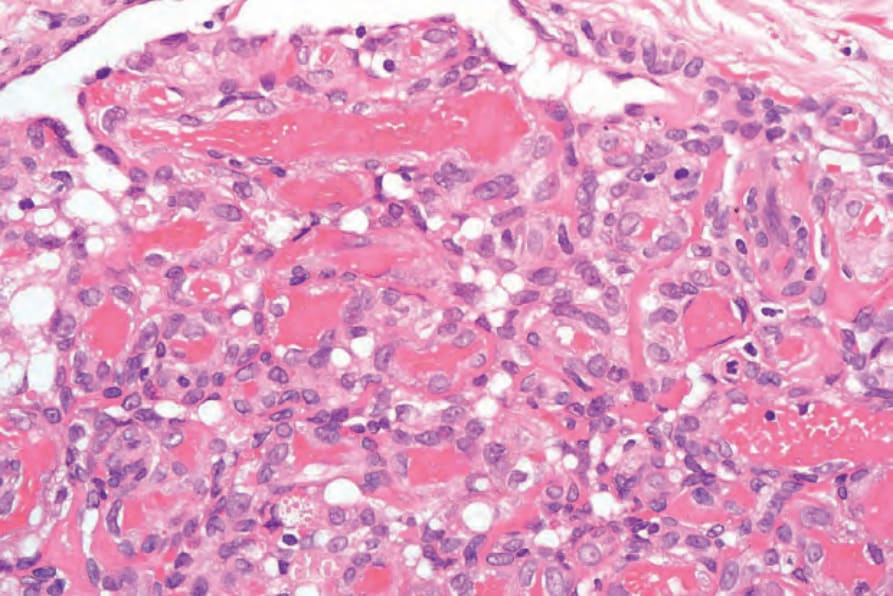
Fig. 35.448 Glomeruloid hemangioma: high-power view.