Rhabdomyosarcoma
Rhabdomyosarcoma
Rhabdomyosarcoma very rarely presents to the dermatologist, first because the tumor itself is rare, and second because it seldom arises in the dermis, albeit that occasional cutaneous metastases do occur.1–6 Traditionally, four main subtypes have been described:7 embryonal (including the botryoid variant), alveolar, pleomorphic and spindle cell/sclerosing. A further very rare epithelioid variant has been recently documented.8–10 The first two, are the most common.11–13
Clinical features Rhabdomyosarcoma presenting in the skin either as a primary tumor or as a metastasis is extremely rare, accounting for only 0.7% of all
1820 Connective tissue tumors
rhabdomyosarcomas (Fig. 35.432).1–3,9,14–26 In the documented cutaneous cases there is a slight male predominance, a predilection for the head and neck, a bimodal age distribution (with a mean age of 10 years for pediatric cases and of 74 years for adult cases) at presentation. The alveolar followed by the embryonal are the most common histologic subtypes in the pediatric population whereas the pleomorphic variant is much more common in adults.9 Cases associated with epidermal nevus syndrome have been reported.27,28 Information about the prognosis of cutaneous lesions is extremely limited but potential for an aggressive course has been reported.9 Although the data available for epithelioid rhabdomyosarcoma are limited, 4 of 18 cases occurred in a superficial location with an equal sex distribution and a mean age of 69.5 years.10
Pathogenesis and histologic features At the molecular genetic level, the alveolar type is characterized by a t(2;13) (q35;q14) and less frequently a t(1;13) (p36;q14) fusing PAX3 or PAX7, respectively, with FOXO1A.13,29–32 More recently, NCOA1 (2p23) and AFX/FOXO4 (Xq13.1) have been shown to substitute for FOXO1A and pair with PAX3 on rare occasion.33,34 PAX3-FOXO1 tumors seem to have a worst prognosis compared to PAX7-FOXO1 tumors.35 In a subset of lesions rearrangements similar to those seen in low grade liposarcoma (MDM2 and CDK4 ) have been identified.36
Embryonal lesions usually have 11p deletions amongst other cytogenetic aberrations.11
8q 13 rearrangements resulting in SRF-NCOA2 and TEAD1-NCOA2 fusion genes have been identified in spindle cell rhabdomyosarcoma.37 A recurrent neomorphic MYOD1 mutation correlates with worse prognosis.38 Pleomorphic rhabdomyosarcoma shows a complex karyotype.39,40
as rhabdomyoblasts, and may be arranged as delicate papillae, solid clumps or lying free within each cell nest. Nuclei are larger and more hyperchromatic than in the embryonal type. Multinucleated (wreath-like) giant cells are a common feature (Fig. 35.439). Epidermotropism has been documented in a case of primary alveolar rhabdomyosarcoma.6 Alveolar-type histology can be seen in cases lacking characteristic fusion genes. Whether these cases are more similar to embryonal or fusion-positive alveolar cases genetically and clinically is currently debated in the literature.41–43
Embryonal type The embryonal type is composed largely of small round or spindle-shaped undifferentiated cells, often arranged loosely in a myxoid stroma.11 Obvious rhabdomyoblasts are variably prominent and show eosinophilic cytoplasm with a ‘strap’ or ‘tadpole’ shape (Figs 35.433–35.435). Variants of this type of rhabdomyosarcoma include botryoid, spindle cell and anaplastic.
Alveolar type The alveolar variant is typified by tumor cells arranged in discrete nests separated by fibrous septa and with an alveolar pattern of cellular dissociation at the center of the cellular aggregates (Figs 35.436 and 35.437).11 Some cases, however, have an almost entirely solid growth pattern (Fig. 35.438). Tumor cells tend to be relatively large and rounded or readily recognizable
Pleomorphic type The pleomorphic type is a heterogeneous tumor characterized by bizarre spindled cells admixed with readily recognizable polygonal rhabdomyoblasts, often in large numbers (Fig. 35.440).11 This variant is largely confined to adults and is almost unknown in the skin.44
Immunohistochemistry is very useful in the diagnosis of rhabdomyosarcoma because tumor cells tend to be at least focally positive for desmin, muscle-specific actin (HHF-35), and the more diagnostically specific myogenin and MyoD1 (Fig. 35.441).11,12
1821 Malignant striated muscle tumors
1822 Connective tissue tumors
Epithelioid type This rare type is composed of uniform cells with epithelioid features (abundant cytoplasm and large vesicular nuclei) in a diffuse sheet-like growth. Nucleoli are prominent and tumor cells may resemble melanoma cells.8 Multinucleated cells may be seen. Obvious rhabdomyoblasts are absent. Prominent necrosis is typically seen.
In all variants of rhabdomyosarcoma tumor cells are variably positive for desmin, myogenin (myf-4) and MyoD-1. Rhabdomyosarcoma may show focal positivity for cytokeratins. Furthermore, positivity for S100 may occasionally be seen focally. Myogenin, Ap2beta, NOS-1, and HMGA1 are available immunohistochemical markers that seem to correlate with fusion status.46
Differential diagnosis Rhabdomyosarcomas should be distinguished from other small round cell neoplasms:
• neuroblastoma contains neurofibrils and shows rosette formation,
• primitive neuroectodermal tumor often has a packeted appearance, shows variable intracytoplasmic PAS positivity, lacks cells resembling rhabdomyoblasts and is diffusely CD99 positive,
• malignant lymphomas are most often (but not always) PAS negative and stain positively for LCA. The pleomorphic type should be differentiated from other pleomorphic tumors by immunohistochemistry and identification of rhabdomyoblasts.
Spindle cell type Although embryonal rhabdomyosarcoma includes a spindle cell variant, a distinctive variant of spindle cell rhabdomyosarcoma has been described in adults. In these lesions there are atypical spindle-shaped cells intermixed with rhabdomyoblasts.45

Fig. 35.432 Cutaneous rhabdomyosarcoma: presentation in the skin is exceptional and occurs in children. This was an embryonal variant. By courtesy of the Institute of Dermatology, London, UK.
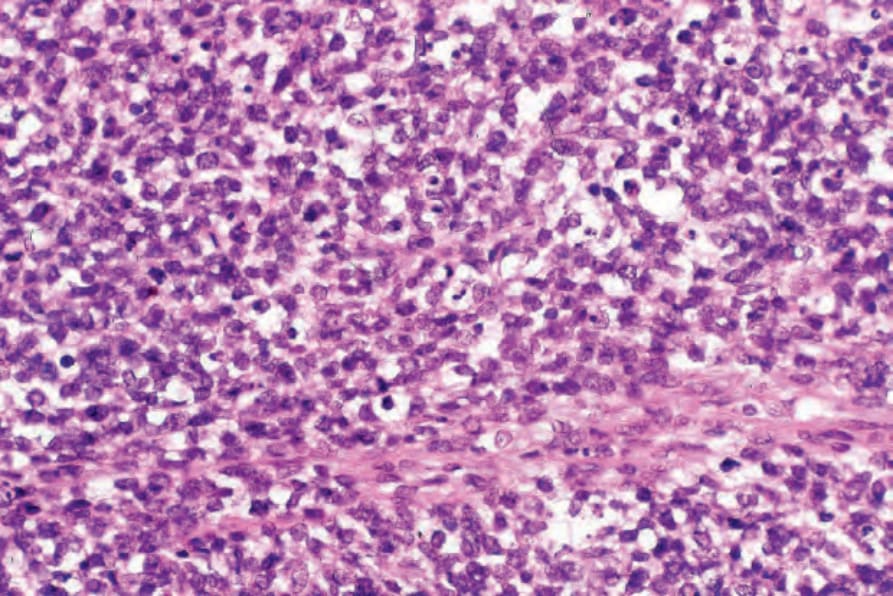
Fig. 35.433 Embryonal rhabdomyosarcoma: an example of undifferentiated rhabdomyosarcoma. The tumor cells are small and contain basophilic nuclei. Diagnosis depends upon immunocytochemistry or identifying more typical rhabdomyoblasts elsewhere in the specimen.
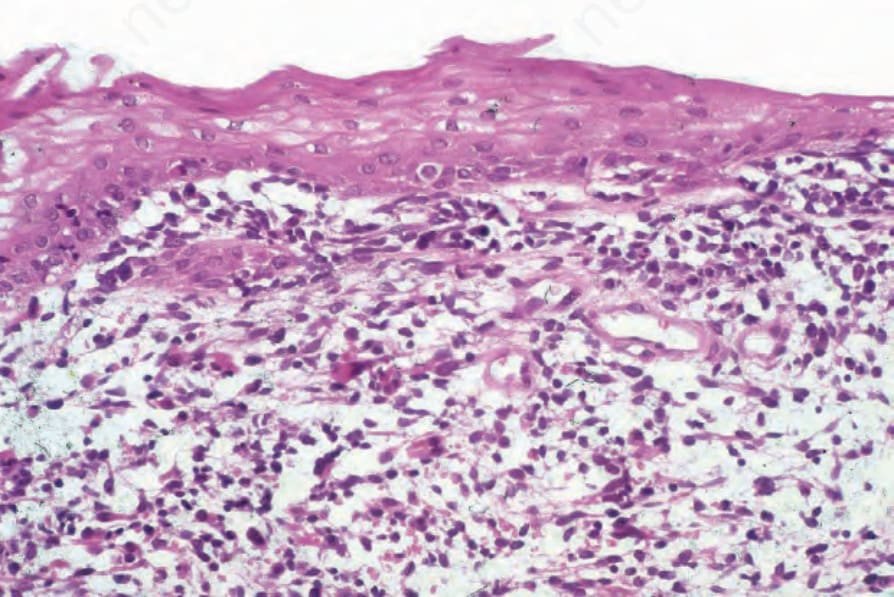
Fig. 35.434 Embryonal rhabdomyosarcoma: beneath the epithelium is an infiltrate of small basophilic cells, and there are also occasional primitive rhabdomyoblasts with more obvious eosinophilic cytoplasm.
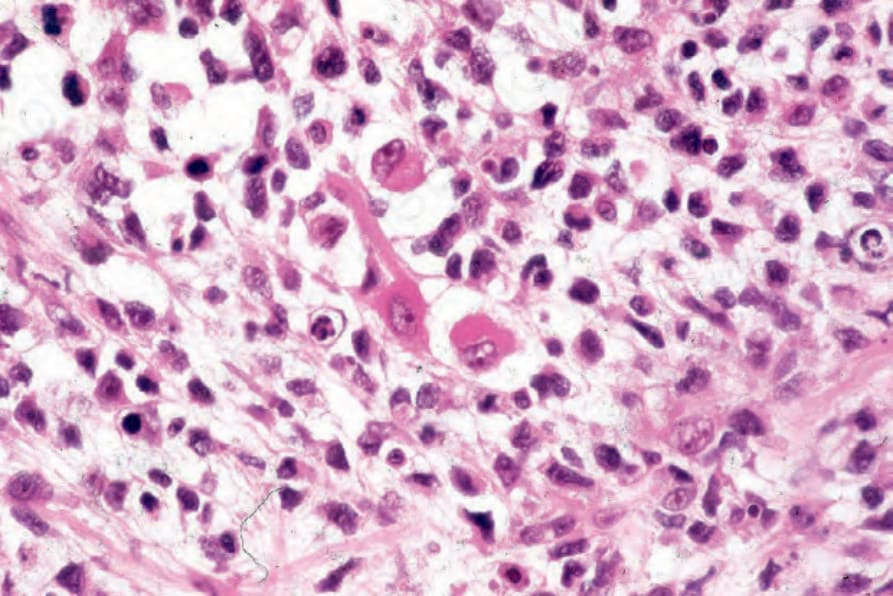
Fig. 35.435 Embryonal rhabdomyosarcoma: in the center of the field is a typical ‘tadpole’ rhabdomyoblast with a tapering eosinophilic, cytoplasmic process.
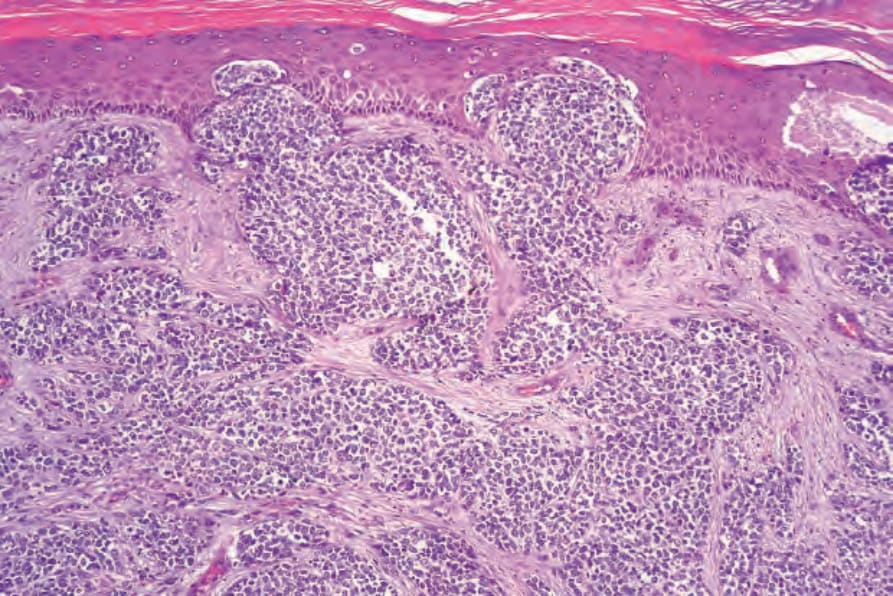
Fig. 35.436 Alveolar rhabdomyosarcoma: this is a very rare example showing epidermotropism. The features mimic neuroendocrine (Merkel cell) carcinoma.
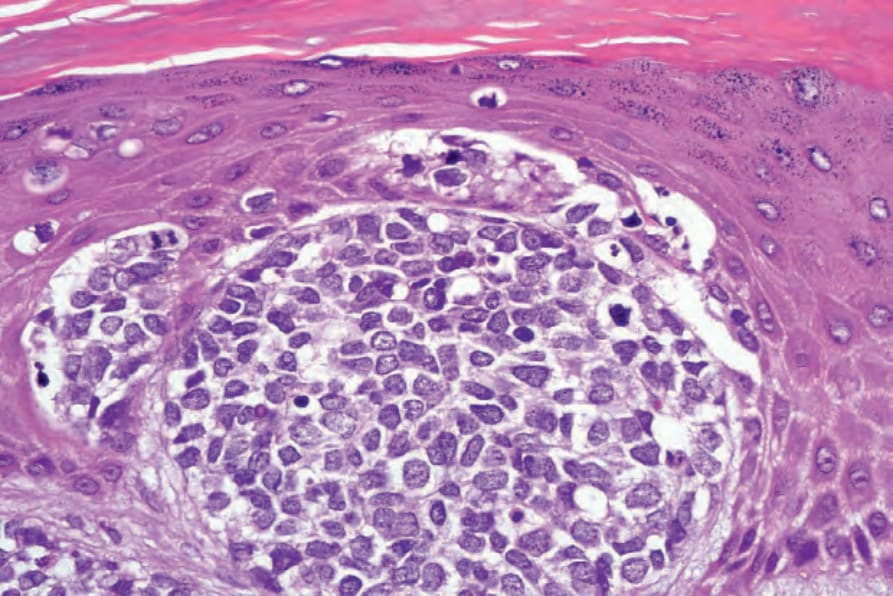
Fig. 35.437 Alveolar rhabdomyosarcoma: high-power view.
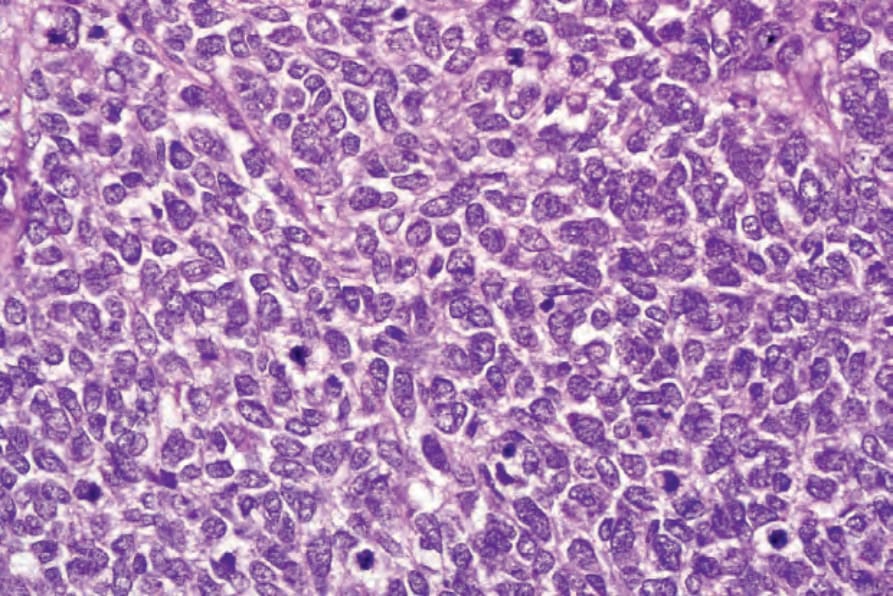
Fig. 35.438 Alveolar rhabdomyosarcoma: the tumor cells have pleomorphic nuclei and multiple mitoses are present. There is no evidence of skeletal muscle differentiation in this example. Diagnosis depends upon immunohistochemistry.
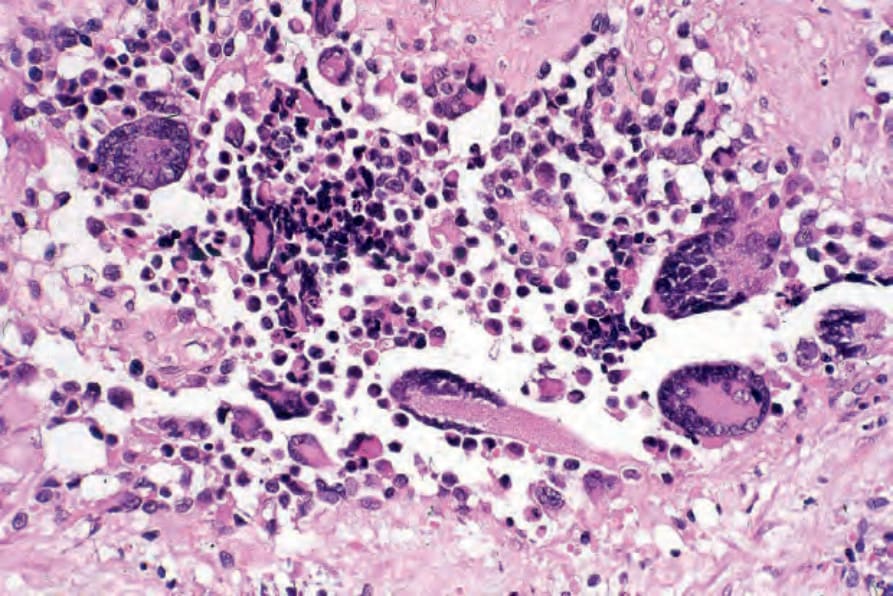
Fig. 35.439 Alveolar rhabdomyosarcoma: wreath-like giant cells are a characteristic feature.
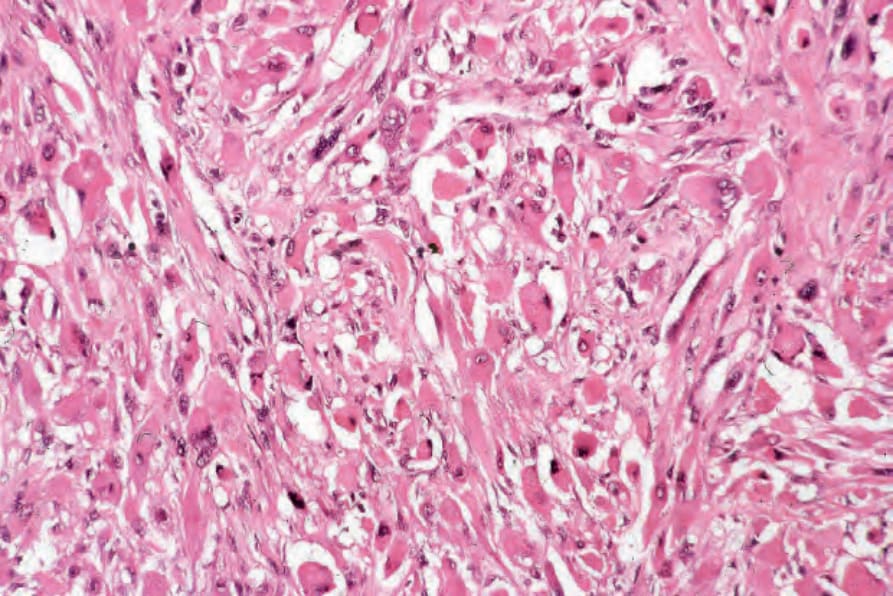
Fig. 35.440 Pleomorphic rhabdomyosarcoma: the rhabdomyoblasts are extremely pleomorphic.
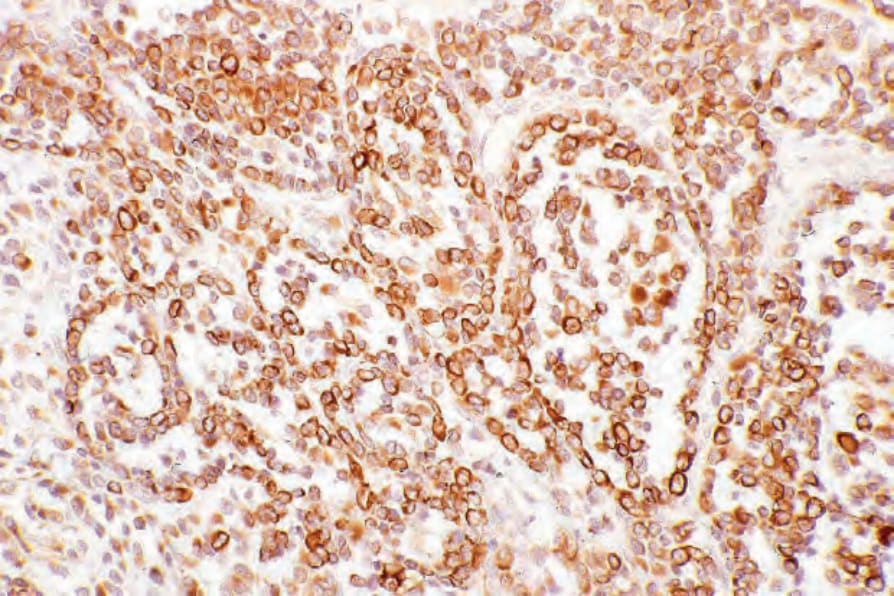
Fig. 35.441 Alveolar rhabdomyosarcoma: in this example, the tumor cells strongly express desmin.