Leiomyosarcoma
Leiomyosarcoma
Clinical features Leiomyosarcoma accounts for a significant proportion of superficial soft tissue sarcomas, although it is more common in a deep location, being most prevalent in the abdomen or retroperitoneum.1–5 The superficial tumors can be divided into two clinical groups:
• cutaneous leiomyosarcoma, which includes leiomyosarcoma of the nipple. The term atypical intradermal smooth muscle neoplasm was introduced in 2011 to include tumors previously classified as atypical (symplastic) leiomyoma and leiomyosarcoma that are primarily confined to the dermis with no or superficial extension to the subcutaneous tissue and indolent biological behavior (see below). However, this term has not been universally accepted.
Cutaneous lesions are usually solitary, derived from or differentiating towards the arrector pili muscle and arise most often in young to middle-aged adults, with a predilection for males.2–4,6,8–13 The trunk and the limbs, especially the lower leg, are most often affected, followed by the head and neck and the tumor can be painful. Local recurrence is commonly seen, but metastasis is very rare.6,14–23 The margin status of the primary tumor seems to be the strongest predictive factor of recurrence 6,18,19 A wide excision with at least 1 cm or Mohs micrographic surgery followed by long term follow-up are considered the best treatment options.24–31
Subcutaneous leiomyosarcomas are very closely related to deeper leiomyosarcomas of soft tissues.2,3,8,32 They arise most often in the fifth to seventh decades, usually in the limbs (especially the thigh) and are larger than dermal lesions. Occasional cases arise from a vein wall. There is a slight predilection for males. Local recurrence is common, and in the long term around 50% of tumors metastasize, with a mortality rate of between
1816 Connective tissue tumors
30% and 50%.11 The subcutaneous location and size are associated with aggressiveness.33 Tumor size greater than 5 cm is associated with a poor prognosis.11 Vulval and scrotal tumors appear to have a better prognosis than lesions arising at other sites.6,34,35
Exceptionally, leiomyosarcoma has been documented at the site of radiation dermatitis, in a pacemaker pocket, in a tattoo, in a scrofuloderma and in a smallpox scar, in a nevus sebaceous and in association with a chronic venous ulcer.36–43 Giant and rapidly growing lesions may occur especially in the face.44–46 A case with skip-lesion behavior has been reported.47 Cutaneous leiomyosarcoma in childhood is very rare.48
Association with hereditary leiomyomatosis and renal cell carcinoma (HLRCC) with Li-Fraumeni (Reed) Syndrome and hereditary retinoblastoma are well documented.6,49–54 In addition, an increased risk has been found in HIV-infected patients.55 Epstein-Barr virus–associated cases in patients with HIV have been reported.56–58
Metastatic sarcoma to the skin is rare, but leiomyosarcoma is the most common sarcoma to do so and usually presents as a rapidly growing mass with predilection for the scalp and with most cases arising from the genitourinary tract rather than other soft tissues.59–70 In a single case, the patient presented with hemorrhagic bullae.71
Histologic features Cutaneous tumors tend to present as an ill-defined diffuse lesion in contrast to the well-circumscribed, more nodular subcutaneous variant. Both, however, are locally infiltrative tumors composed of interlacing bundles of smooth muscle cells with eosinophilic cytoplasm and blunt-ended, cigar-shaped, often vesicular nuclei (Figs 35.418 and 35.419). Nuclear palisading and tandem alignment are not uncommon. Significant cytological pleomorphism (even to the point of mimicking so-called pleomorphic malignant fibrous histiocytoma, MFH) is more common in subcutaneous than cutaneous variants (Fig. 35.420). Prominent pleomorphism in dermal tumors is generally a feature of metastatic lesions, particularly from the uterus.72–74 Primary cutaneous lesions with prominent pleomorphism might be more aggressive as are those that extend into the subcutis even if the extension is minimal.75 Most cases are usually diffusely or more uncommonly focally positive for SMA, calponin, desmin and h-caldesmon (Fig. 35.421).8,76,77 Very focal keratin positivity has also been documented.78 By
1817 Malignant smooth muscle tumors
immunohistochemistry, PTEN is lost in a majority of cases suggesting a possible pathogenetic molecular mechanism.79 Periodic acid-Schiff staining may demonstrate perinuclear glycogen vacuoles. Cutaneous and subcutaneous leiomyosarcomas lesions can rarely be predominantly epithelioid or show granular cell change (Figs 35.422 and 35.423).80–83 A mature adipocytic component may be seen.84 Prominent desmoplasia has also been documented in rare cases.85–90 In addition, subcutaneous variants sometimes display myxoid change, hyalinization, admixed osteoclastic giant cells and an inflammatory cell infiltrate.91
primary counterparts. In addition, they often show a diffuse or nodular pattern and more extensive infiltration of the subcutaneous tissue. Nevertheless, none of the histologic features seem to correlate with adverse biological behavior.6
Although leiomyosarcoma may bear a close resemblance to benign leiomyoma, the former usually shows variable pleomorphism with at least mild cytologic atypia and mitotic activity. It has been suggested that positivity for p53 in a large number of cells supports a diagnosis of leiomyosarcoma.92–95 Other markers such as Ki67 and S100A6 may be of help (see also above).96,97 Necrosis and hemorrhage are more common in subcutaneous variants and are also suggestive of malignancy. Primary cutaneous tumors are most often grade 1 lesions. Subcutaneous extension is usually limited and superficial. Tumors either infiltrate the fibrous septa or extend into the adipose tissue typically with pushing margins. Recurrent tumors may show more cytologic atypia, and are more often associated with necrosis compared with their
The tumor cells may be identified ultrastructurally by the presence of actin filaments with focal densities (Figs 35.424 and 35.425).
Differential diagnosis Differential diagnosis is usually not problematic. Spindle cell melanoma can look remarkably similar to leiomyosarcoma, especially in an acral location, but the growth pattern in the former is more infiltrative, pleomorphism is usually more prominent and S100 protein is positive whereas muscle markers are negative. Similarly, epithelioid variants of leiomyosarcoma can be distinguished from melanoma and carcinoma by immunohistochemistry. Distinction from the cellular variant of fibrous histiocytoma and cellular schwannoma has already been discussed in the representative sections. Metastatic leiomyosarcoma also enters the differential diagnosis. This typically presents as a distinct nodule showing nuclear pleomorphism and mitotic activity (Figs 35.426 and 35.427). Clinicopathological correlation is essential to establish the correct diagnosis.
1818 Connective tissue tumors
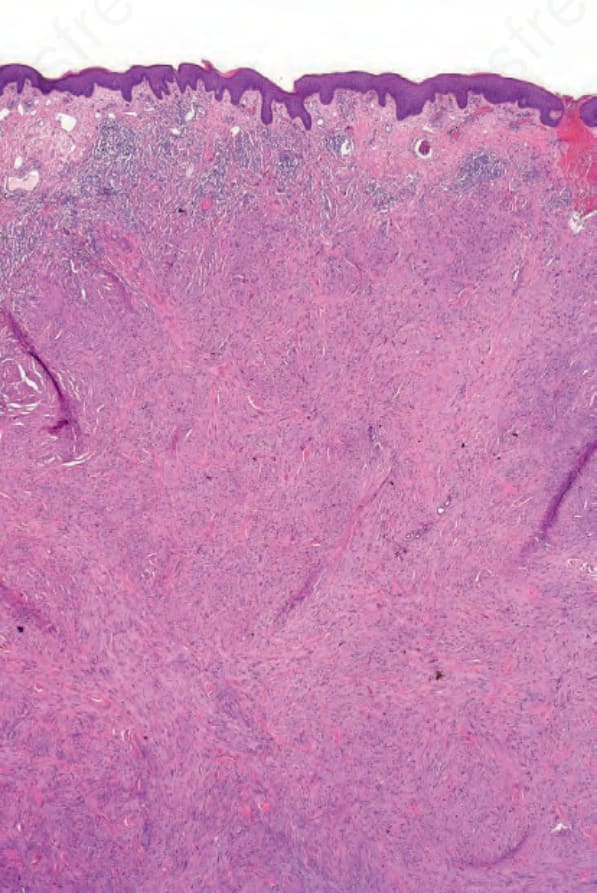
Fig. 35.418 Leiomyosarcoma: extending up to the papillary dermis is a spindled cell tumor.
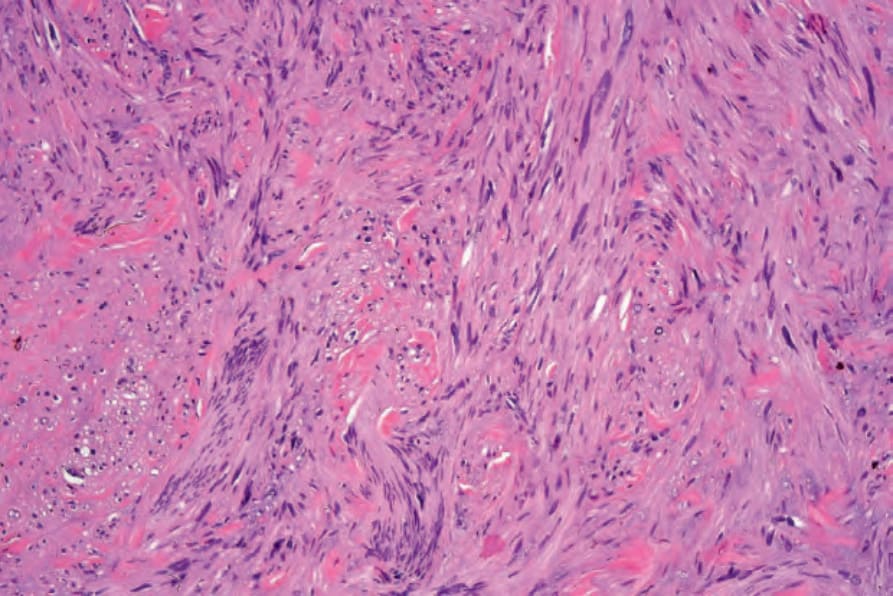
Fig. 35.419 Leiomyosarcoma: as with its benign counterpart, the spindled cells exhibit marked eosinophilia.
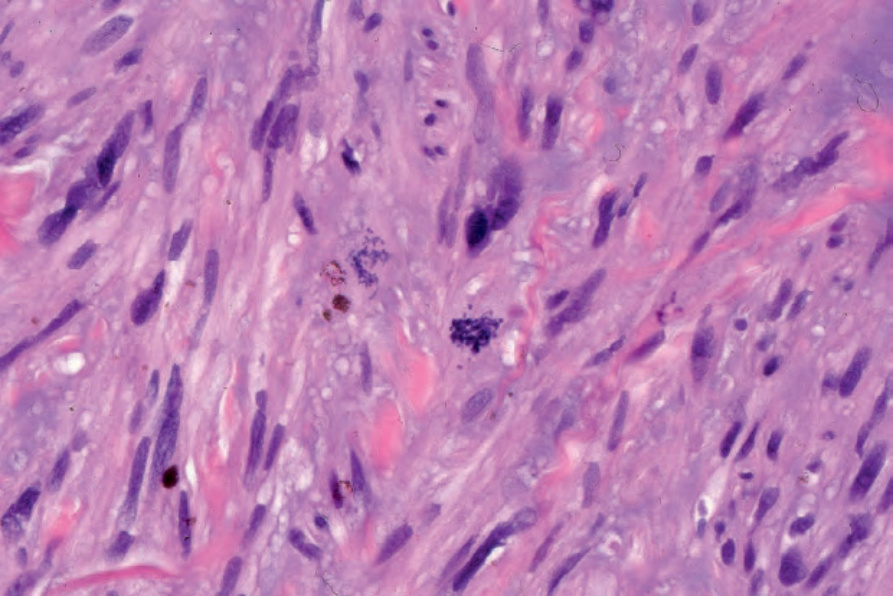
Fig. 35.420 Leiomyosarcoma: note the presence of marked mitotic activity.
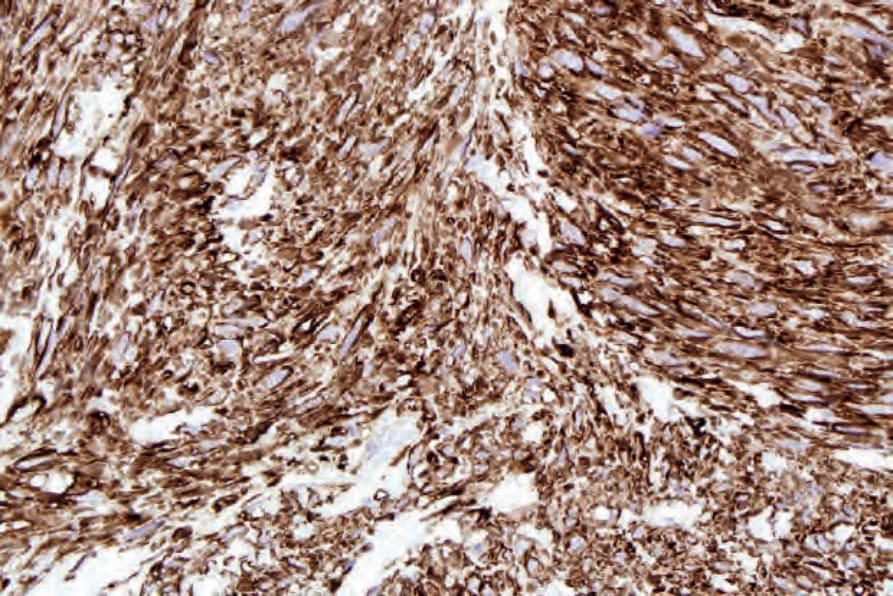
Fig. 35.421 Leiomyosarcoma: the tumor cells show strong h-caldesmon expression.
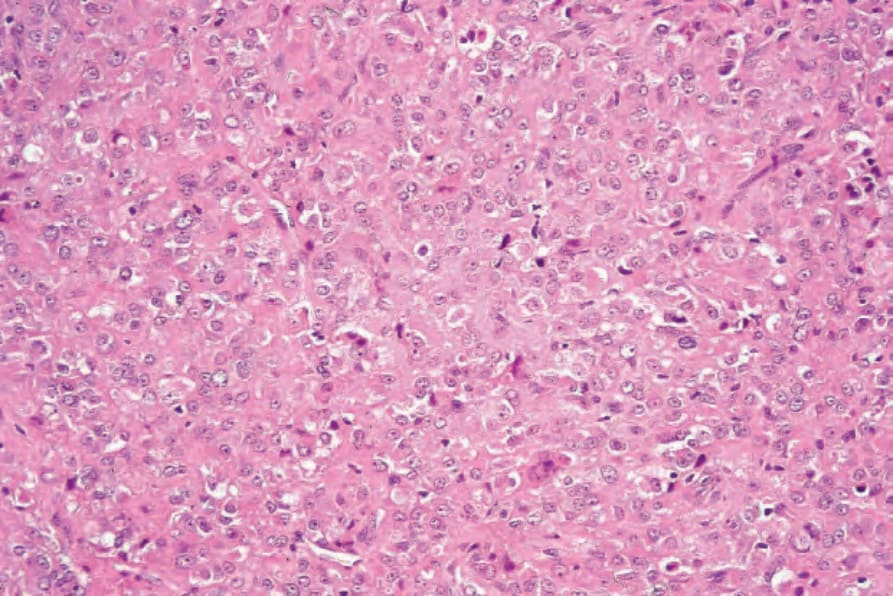
Fig. 35.422 Epithelioid leiomyosarcoma: in this variant, the tumor cells are epithelioid with abundant eosinophilic cytoplasm and vesicular nuclei with prominent nucleoli.
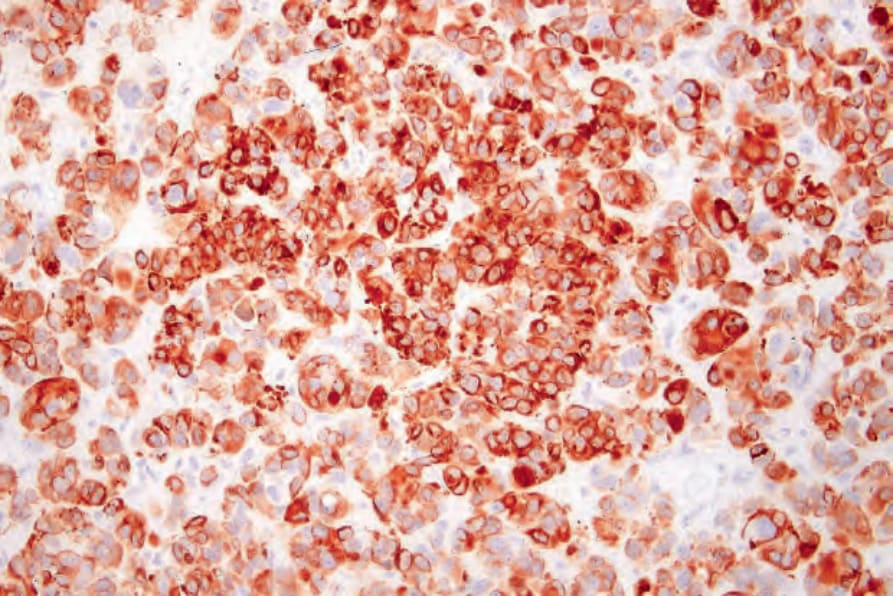
Fig. 35.423 Epithelioid leiomyosarcoma: the tumor cells express desmin.
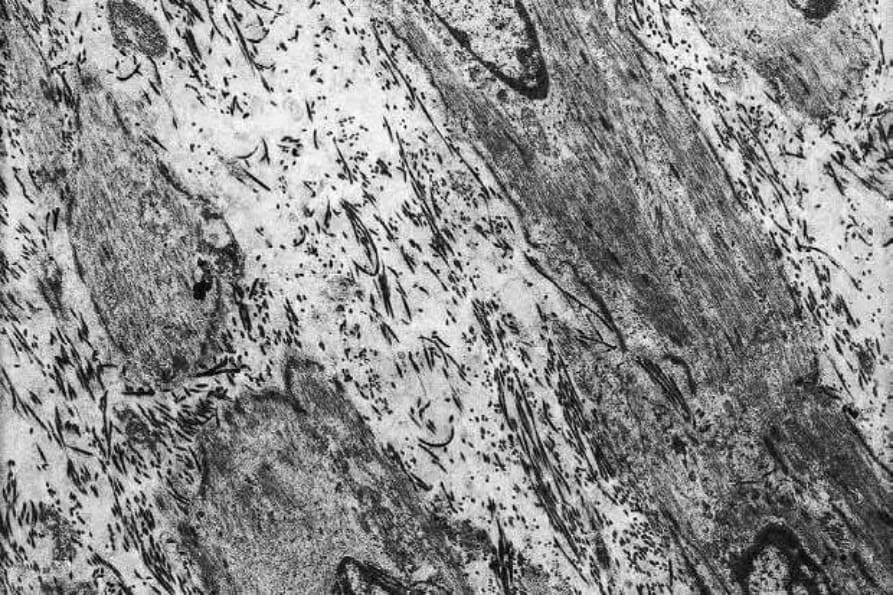
Fig. 35.424 Leiomyosarcoma: note the presence of abundant actin filaments.
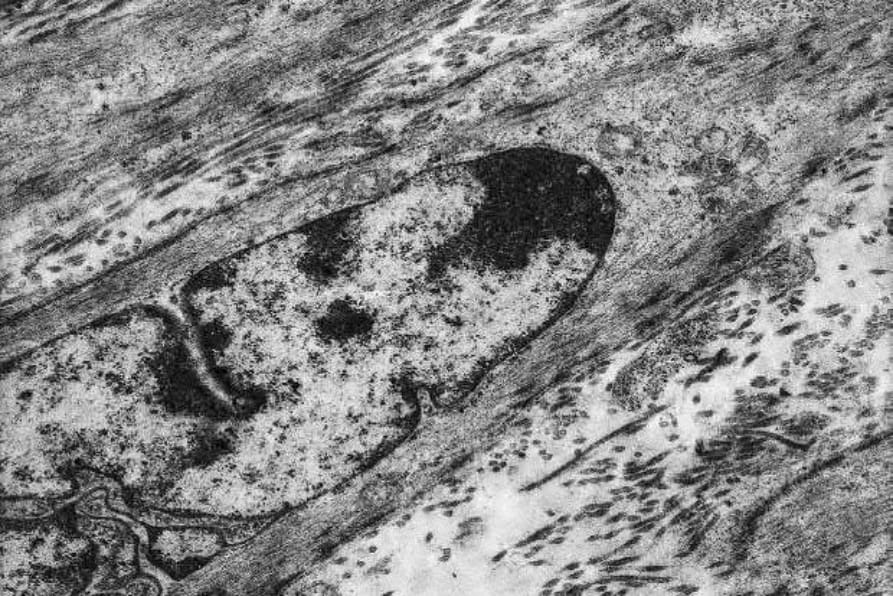
Fig. 35.425 Leiomyosarcoma: high-power view showing focal densities characteristic of smooth muscle differentiation.
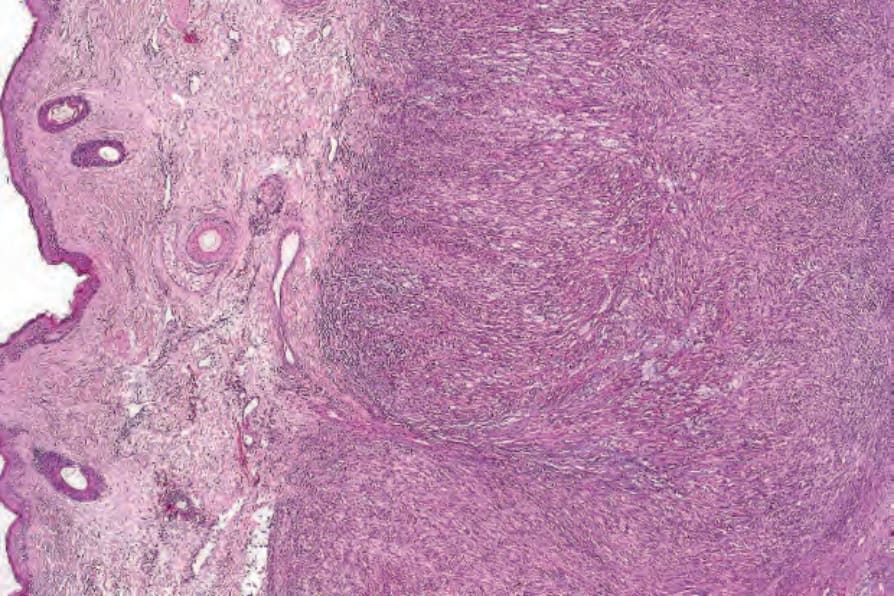
Fig. 35.426 Metastatic leiomyosarcoma: metastatic deposits are characteristically nodular and well circumscribed.
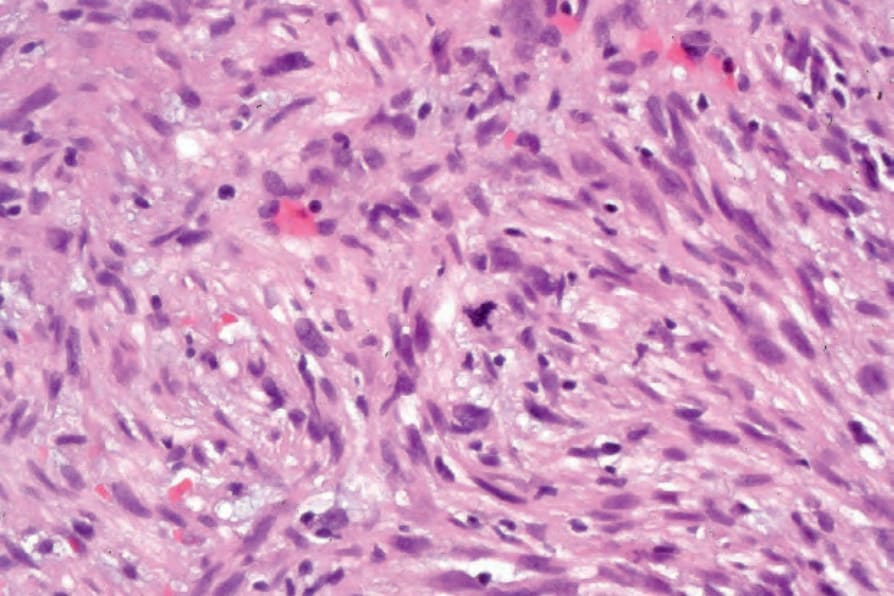
Fig. 35.427 Metastatic leiomyosarcoma: note the nuclear pleomorphism and abnormal mitosis.