Genital leiomyoma
Genital leiomyoma
Clinical features Genital leiomyoma originates from the superficial smooth muscle of the scrotum, vulva or nipple.1–5 Traditionally, such cases have been classified as variants of pilar leiomyoma. This is appropriate for nipple lesions, but scrotal and vulval tumors show different pathological features. They are uncommon, tend to be larger and are better circumscribed. They usually present in middle-aged adults. Multiple leiomyomas of the vulva may be a sign of Alport syndrome.3
A pericentric inversion (12)(p12q13–14) has been described in a single case of vulval leiomyoma.6
Histologic features Nipple leiomyoma is histologically identical to lesions arising elsewhere on the integument (Fig. 35.416). Scrotal leiomyomas, however, which arise from the dartos muscle, tend to be quite cellular and often show a focal mononuclear inflammatory cell infiltrate (Fig. 35.417). Cytologic atypia as present in symplastic leiomyoma may be seen but mitotic figures are exceptional (bizarre leiomyoma)5,7,8 Vulval leiomyomas arise in the labia majora and commonly display myxoid change and hyalinization.9 Epithelioid cell change may also be a feature.6 Scrotal leiomyomas express androgen receptor.10
• subcutaneous leiomyosarcoma, which includes vulval and scrotal variants.7
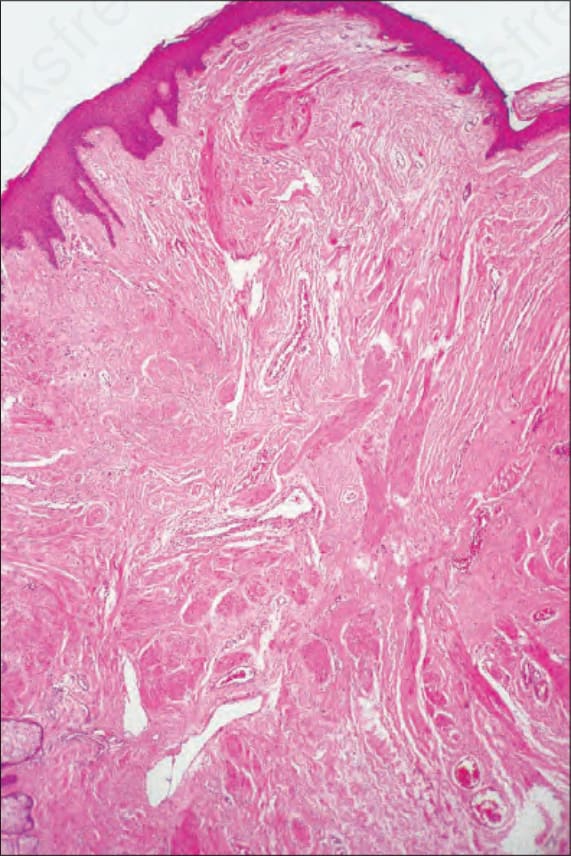
Fig. 35.416 Nipple leiomyoma: as with the pilar variant, the tumor is composed of a poorly circumscribed proliferation of mature smooth muscle cell infiltrate.
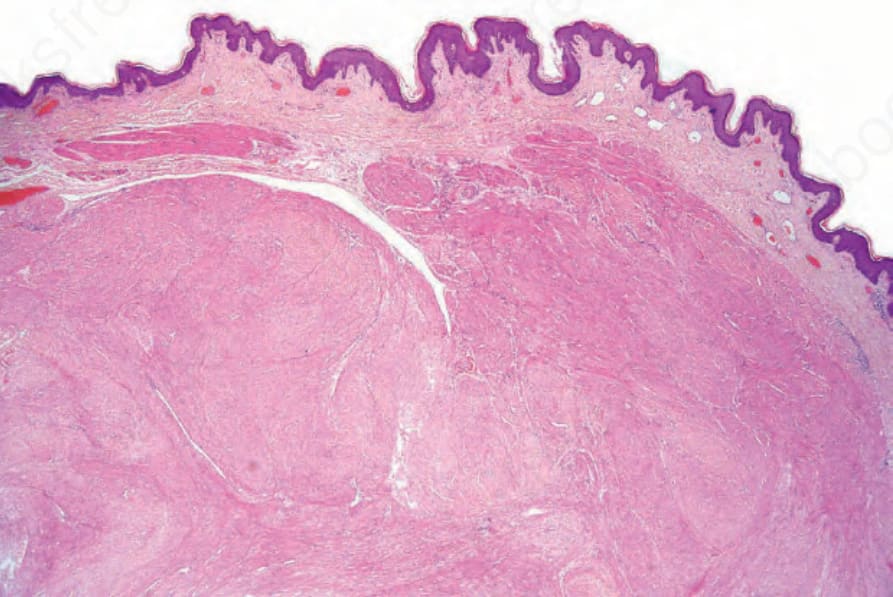
Fig. 35.417 Scrotal leiomyoma: note the circumscription and multinodularity.