Pilar leiomyoma
Pilar leiomyoma
Clinical features
Congenital smooth muscle hamartoma is a rare lesion that presents in infants as an indurated, often hyperpigmented macule or plaque with perifollicular papules or coarse hairs.1–6 There is a slight male predominance and the prevalence has been estimated as 1 : 2600 live births.5 Occasional cases have been reported presenting after birth.7,8 The most frequent location is the lumbosacral area and there is also predilection for the proximal limbs, with rare cases occurring elsewhere including face, volar skin, and the oral cavity.9–11 Unusual presentations include a linear and atrophic plaque, marked folding of the skin, a reticulate vascular nevus-like appearance, a Michelin tire syndrome-like appearance, and diffuse involvement with hypertrichosis lanuginosa.12–18 In one case, the presenting sign was myokymia (pseudo-Darier sign).19 In other cases, a pseudo-Darier sign can rarely be elicited.20 Unusual sites of presentation include the conjunctival fornix.21 Occasional patients have multiple lesions and more extensive, generalized involvement.22,23 Familial cases may occur.24,25 Acquired cases are exceptional.26,27 Examples of acquired smooth muscle hamartoma of the genitalia may represent hyperplasia of smooth muscle as a result of chronic scrotal lymphedema.28,29 Focal changes simulating smooth muscle hamartoma have been documented in a case of port-wine stain.30
Pilar leiomyoma usually presents in young adults, most often on the limbs or trunk (Figs 35.411 and 35.412).1–5 Congenital lesions are probably variants of smooth muscle hamartoma.6 Occurrence in children is exceptional.7 Lesions are multiple (rarely hundreds of lesions are seen), small, slowly growing papules generally less than 1 cm in diameter, and typically painful or tender, particularly when compressed or exposed to a cold environment. In the limbs, pilar leiomyomas tend to favor the extensor surfaces. Patients
Histologic features Histologically, there are numerous haphazardly oriented intradermal bundles of mature smooth muscle (Figs 35.409 and 35.410). Hair follicles are normal in number and there is sometimes mild hyperkeratosis, acanthosis and hyperpigmentation of the basal cell layer. A rare association within the same lesion of a congenital melanocytic nevus and a smooth muscle hamartoma has been documented.31
Immunohistochemistry shows diffuse staining for SMA, desmin and h-caldesmon.32
A close relationship with Becker nevus has been suggested, but the latter is an acquired lesion that appears later in life and shows hypertrichosis, hyperpigmentation and usually only a mild increase in the amount of smooth muscle.2,6,33
1814 Connective tissue tumors
may present with plaque-like variants or tumors in a zosteriform distribution.8 Multiple leiomyomas have been described in association with HIV infection, chronic lymphocytic leukemia and erythrocytosis.9–11
Recurrence is uncommon after excision, but new lesions may continue to develop over the years. An eruptive case resembling spontaneous eruptive keloids has been reported.12
Solitary pilar leiomyomas are less commonly seen and tend to be larger. There is a slight male predominance, with predilection for the limbs.40–42
In a small proportion of cases with multiple lesions, there is a positive family history, with an autosomal dominant inheritance (Fig. 35.413).13,14 A case in identical twins has been documented.15 A segmental distribution may be seen in familial and exceptionally in sporadic cases.16–20 For many years it was recognized that multiple cutaneous leiomyomas are associated with uterine leiomyomas (MCUL).21–24 A further association with papillary or collecting duct renal cell cancer was been identified and the syndrome is now termed hereditary leiomyomatosis and renal cell cancer (HLRCC).24–28 Loss of function in the gene responsible for this syndrome, FH (1q42.3~q43), results in fumarate hydratase deficiency.29–36 Fumarate hydratase, a component of the tricarboxylic acid cycle, acts as a tumor suppressor gene and may be involved in DNA damage response.37 Although most patients with the syndrome have cutaneous and uterine leiomyomas, renal cancer is only seen in a minority of patients. Interestingly, similar mutations are very rare in sporadic variants.38,39
Histologic features Pilar leiomyomas, which are ill defined and intradermal, usually merge imperceptibly with the surrounding connective tissue (Figs 35.414 and 35.415). Only occasional lesions are more nodular. The epidermis is typically unaffected but elongation of the rete ridges and or hyperpigmentation may be seen.41 Each tumor is composed of uniform interlacing bundles or irregular collections of elongated cells with brightly eosinophilic cytoplasm and blunt-ended or cigar-shaped nuclei. A mature adipocytic component is exceptional.43 Mitotic figures are only very rarely seen.5 Focal cytologic atypia due to degeneration may be a feature, similar to that seen in symplastic leiomyomas of the uterus (pilar symplastic or atypical leiomyoma).44–50 Adequate sampling of these lesions is necessary as changes of otherwise typical leiomyosarcoma may be focally found.51 Exceptionally, palisading mimicking Verocay bodies, and granular cell change may be evident.52,53
Tumor cells are usually uniformly positive for SMA, calponin, desmin and h-caldesmon.
Immunohistochemistry for fumarate hydratase (negative staining) has been suggested to identify patients with MCUL and HLRCC.54 However, the sensitivity and specificity of this test in the published series was only of 83.3% and 75%, respectively.54 In a further study by the same authors, it has been suggested that anti S-(2-Succino)-Cysteine staining (positive as opposed to negative fumarate hydratase in suspected cases) increases the diagnostic accuracy in around 19% of cases.55
1815 Malignant smooth muscle tumors
Differential diagnosis The clinical history, particularly in cases with multiple lesions, often makes the diagnosis straightforward. Distinction from dermatofibroma is afforded by the leiomyoma’s uniform cell content and configuration in addition to desmin and SMA positivity. Cellular neurofibroma is S100 protein positive and lacks the eosinophilic cytoplasm, myofibrils and blunt-ended nuclei of leiomyoma. Differentiation from cutaneous leiomyosarcoma (atypical intradermal smooth muscle neoplasm) is based on the presence of mitoses and the usually greater nuclear pleomorphism in the latter tumor. When pyknotic nuclei are present staining with Ki67 and/or phosphohistone-H3 may be of help to identify proliferating cells or those undergoing mitosis respectively.56 In addition S100A6 has been found to be weak or absent in leiomyoma and strongly positive in cutaneous leiomyosarcoma (atypical intradermal smooth muscle neoplasm).57
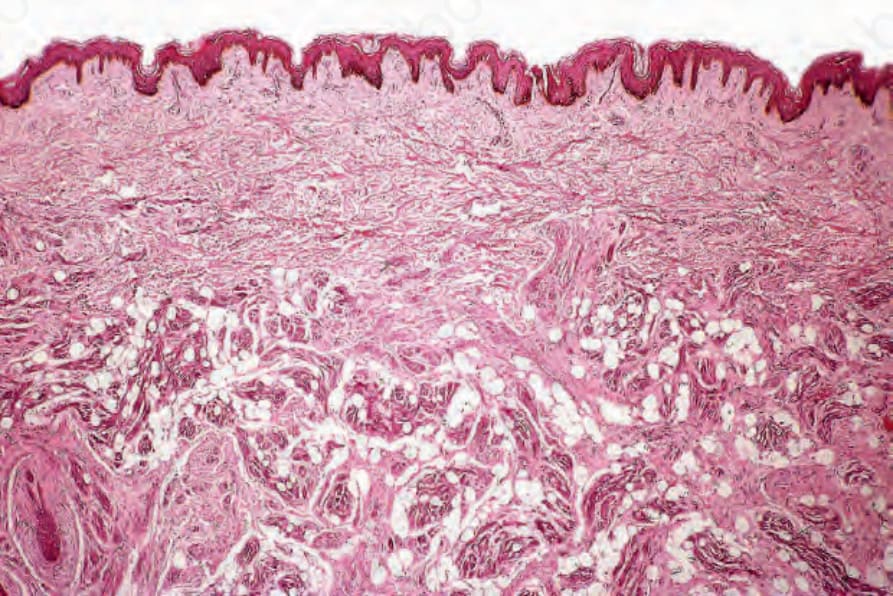
Fig. 35.409 Congenital smooth muscle hamartoma: irregular bundles of smooth muscle are present in the deeper dermis and subcutaneous fat.

Fig. 35.410 Congenital smooth muscle hamartoma: high-power view.

Fig. 35.411 Pilar leiomyoma: multiple erythematous papules are present. By courtesy of the Institute of Dermatology, London, UK.

Fig. 35.412 Pilar leiomyoma: close-up view of an erythematous nodule. By courtesy of the Institute of Dermatology, London, UK.

Fig. 35.413 Familial pilar leiomyomas: sometimes, hundreds of lesions may be present. By courtesy of the Institute of Dermatology, London, UK.
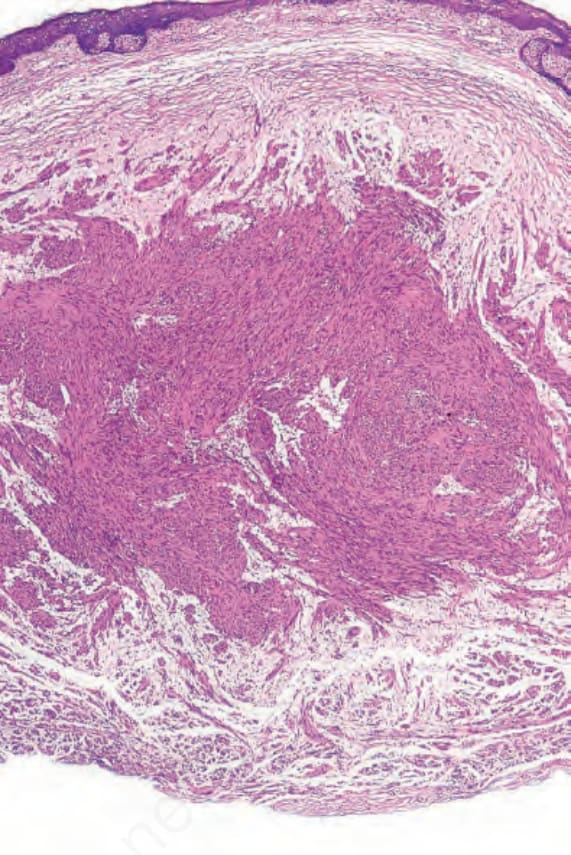
Fig. 35.414 Pilar leiomyoma: within the reticular dermis is an ill-defined tumor composed of broad interlacing fascicles of eosinophilic spindle cells.
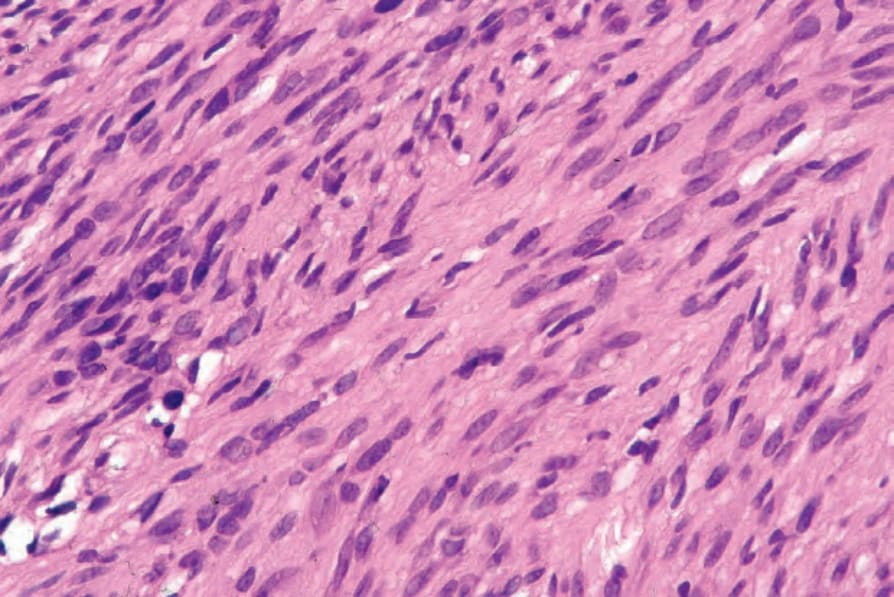
Fig. 35.415 Pilar leiomyoma: the tumor cell nuclei are characteristically cigar shaped.
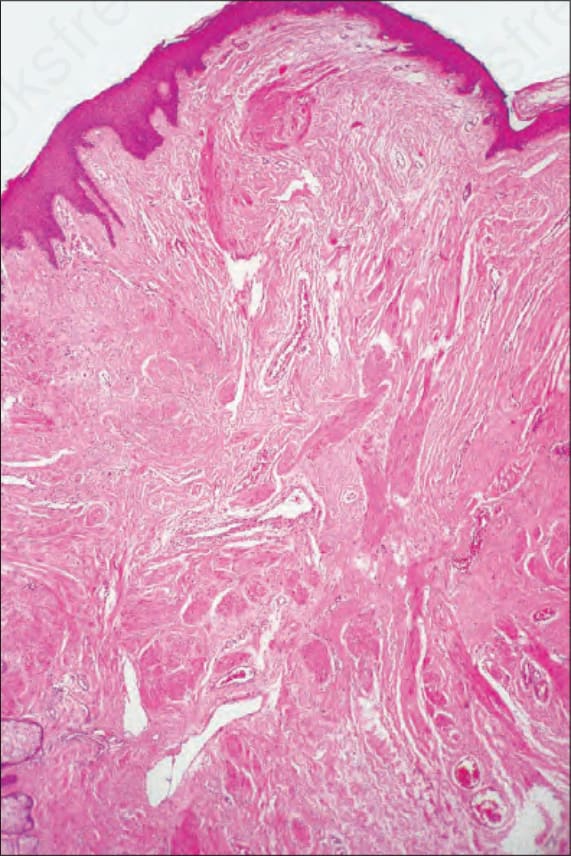
Fig. 35.416 Nipple leiomyoma: as with the pilar variant, the tumor is composed of a poorly circumscribed proliferation of mature smooth muscle cell infiltrate.