Lipoma
Lipoma
Clinical features Lipomas are the most common connective tissue tumors.1–3 They appear to occur more frequently in the obese, usually in middle and late adult life, may be multiple, especially in young adults, and are purportedly more common in females.3 This, however, may only be a reflection of the greater tendency of women to request cosmetic attention for otherwise innocuous lesions. Lipomas are very uncommon in children and when present should raise the possibility of Bannayan-Riley-Ruvalcaba syndrome.4 Congenital lipomas are very rare.5 Multiple lesions may occur in a familial setting.6 A case of multiple lipomas after total body electron beam therapy for mycosis fungoides has been reported.7 Multiple lipomas have also been described in association with rosiglitazone, a peroxisome proliferator-activator receptor (PPAR) gamma agonist, in association with systemic chemotherapy for Hodgkin lymphoma and in Cowden disease.8–10
adipose tissue) occasional vacuolated nuclei known as lochkern may be seen (Fig. 35.8). These must not be confused with lipoblasts, the most important diagnostic feature of liposarcoma, which are characterized by multiple intracytoplasmic lipid vacuoles associated with scalloping of peripherally located hyperchromatic or bizarre nuclei. In some lesions there are septa of collagen between adipose tissue lobules and they are referred to as fibrolipomas or sclerotic lipomas. A variant of lipoma with predilection for acral sites (fingers, wrists, toes) and characterized by prominent collagenous or myxocollagenous stroma, bland stellate or spindle-shaped cells and scattered adipocytes has been described as sclerotic (fibroma-like) lipoma.28 A further variant, known as fibrohistiocytic lipoma, has been reported.29 Typically, it presents in the subcutis of the trunk and shows predilection for young men. Most lesions are small and asymptomatic. Tumors are well circumscribed and consist of lobules of mature adipocytes containing focal areas with plump spindle-shaped cells arranged in a fascicular or focal storiform pattern.29 Rare lipomas may contain metaplastic bone.30 Those containing sweat glands do not represent an adenolipoma but rather entrapment of normal glands by the tumor.31–33 Lesions containing smooth muscle are rare, regarded as a distinct entity under the term myolipoma and tend to be deep seated.27,34 Secondary changes including focal areas of fat necrosis with foamy histiocytes are often seen and some cases show membranous fat necrosis.35
The lesions are found most often on the trunk, abdomen or neck, followed by the proximal extremities, and rarely on the face (particularly the forehead), scalp, hands or feet. Palmar lipomas are exceptional and may present with lesions simulating piezogenic pedal papules.11 Periungual and subungual lesions are exceptional.12,13 Trauma has been associated with induction of lipomas although it is not clear whether all of these lesions may represent pseudolipomas.14,15 The latter sometimes includes an intravascular lesion.16 Villous lipomatous proliferation of synovial membrane (lipoma arborescens) represents an infiltration of sub synovial connective tissue by adipose tissue.17 Typically, lipomas originate subcutaneously, are slow growing, mobile and painless; sometimes they are multiple. Size varies and some lesions are very large. Dermal examples are often clinically confused with fibroepithelial polyps. Although the lesions are usually well circumscribed, the less common deep variants, which may arise in muscle or in association with a tendon sheath or nerve, are generally ill defined and infiltrative.
Dermal lipomas are less well circumscribed and consist of scattered groups of mature adipocytes between collagen bundles (Figs 35.9 and 35.10). Nevus lipomatosus superficialis is histologically indistinguishable from dermal lipoma. The former term should therefore only be used, as a diagnostic term, in a specific clinical context (see below).
Differential diagnosis The diagnosis of a lipoma is usually straightforward. Distinction from an atypical lipomatous tumor (adipocytic /lipoma-like variant) is mainly based on the presence of adipocytes varying in size and shape and with hyperchromatic nuclei in the latter. In addition, atypical stromal cells are usually present in the latter. The absence of lipoblasts is not a helpful finding as they are not always present in atypical lipomatous tumor. In particularly difficult cases, immunohistochemistry with MDM2 and CDK4 may be helpful (see under atypical lipomatous tumor). Dermal lipomas can be confused with pseudolipomatosis cutis. The latter is an artifactual incidental finding distinguished from a dermal lipoma by the presence of empty, round spaces simulating adipocytes but lacking nuclei and of variable size.36
Subcutaneous lipomas are entirely benign and local excision is nearly always curative; recurrence is infrequent (less than 5%) and progression to liposarcoma virtually never occurs.
Pathogenesis and histologic features Lipomas at all locations show clonal karyotypic abnormalities in up to 75% of cases.18–25 The most common rearrangement involves the 12q1315 region affecting the HMGA2 gene. The deregulation of HMGA2 appears to play a role in the genesis of the tumor. The most common translocation is t(3;12)(q2728;q1315) leading to a fusion gene HMGA2-LPP.24,25 Many other translocations involving different chromosomes may be seen including 1p36, 1p3234, 2p2224, 2q3537, 5q33, 9p2122, 12p1113, 13q1214, and 4q2728.24,25 Other less common chromosomal aberrations include 6p2123 (sometimes involving the HMGA1B), 13q1112 and 12q2224. The only translocation associated with 6p2123 is t(3;6)(q27-28;p21~23).
The tumors are usually encapsulated, lobulated, and largely composed of univacuolated mature adipocytes, the nucleus and cytoplasm of which are compressed centrifugally (Fig. 35.1). The lobules are divided by delicate fibrous septa containing thin-walled vessels. Degenerative changes, often characterized by fibrosis, focal fat necrosis, or myxoid change, are not uncommon, particularly in long-standing or frequently traumatized cases (Figs 35.2–35.7). Prominent myxoid change and high vascularity are sometime present.26 However, the majority of lipomas with prominent myxoid change (myxolipomas) are now considered to be part of the spectrum of spindle cell lipomas.27 Foci of other fully differentiated mesenchymal elements, including bone or cartilage, can also be seen.
Although nuclear pleomorphism, hyperchromasia, and mitotic activity do not occur in lipomas, in any benign fatty lesion (or even in normal
1701 Introduction
1702 Connective tissue tumors
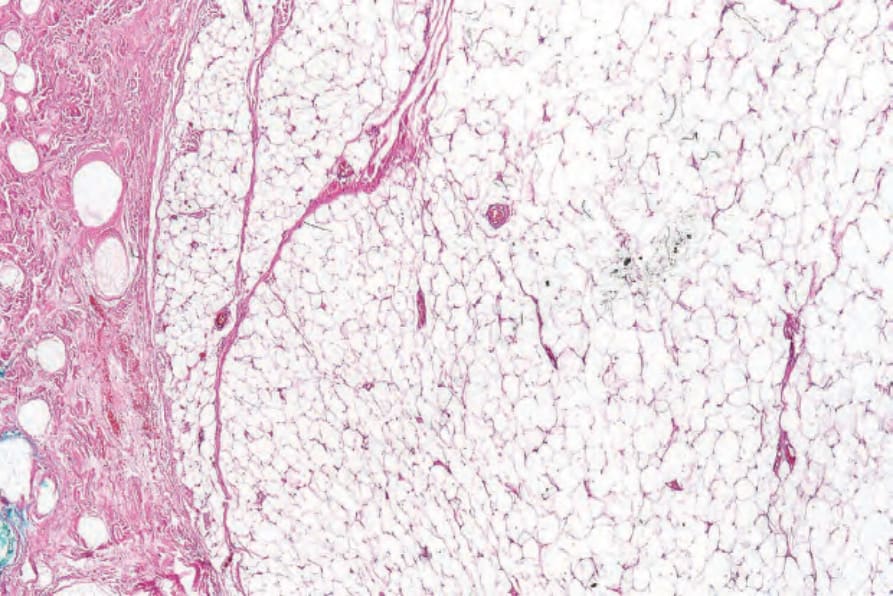
Fig. 35.1 Lipoma: low-power view showing a circumscribed encapsulated tumor composed of mature adipocytes.
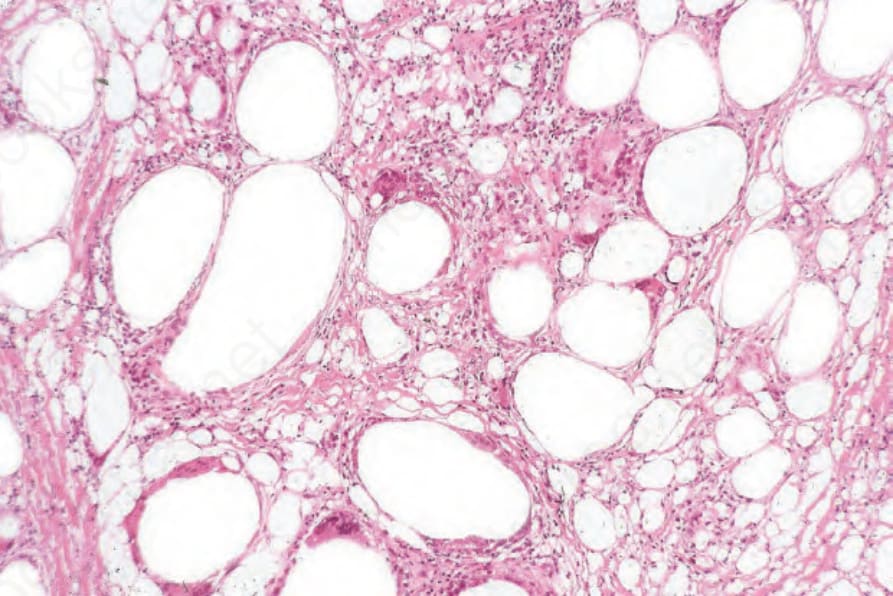
Fig. 35.2 Lipoma: post-traumatic fat necrosis.
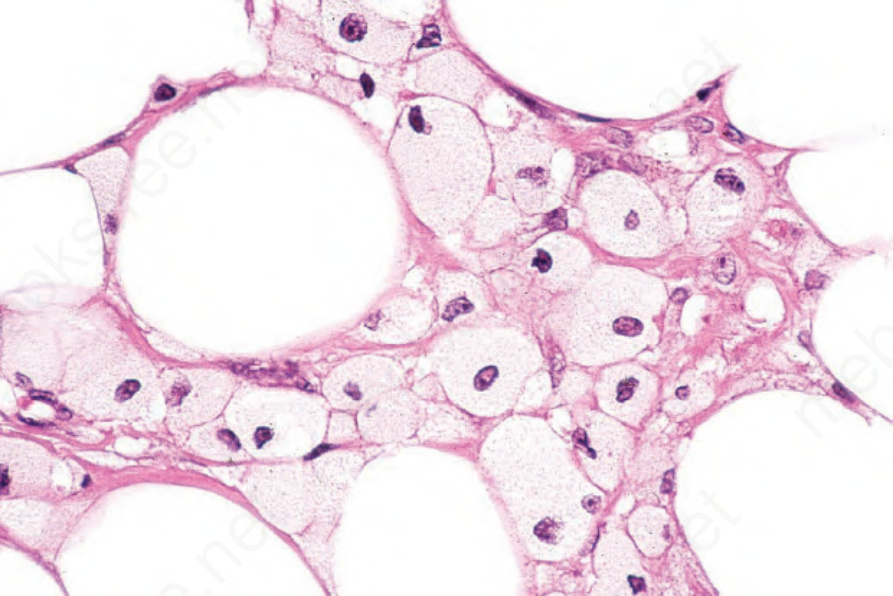
Fig. 35.3 Lipoma: note the lipid-laden xanthoma cells.
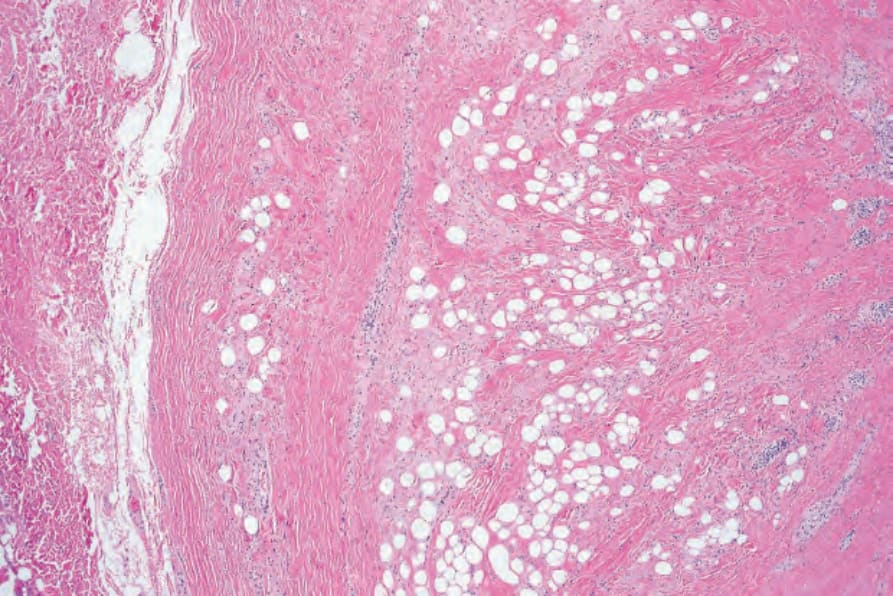
Fig. 35.4 Fibrolipoma: this term is sometimes applied to a lipoma with a prominent fibrous component.
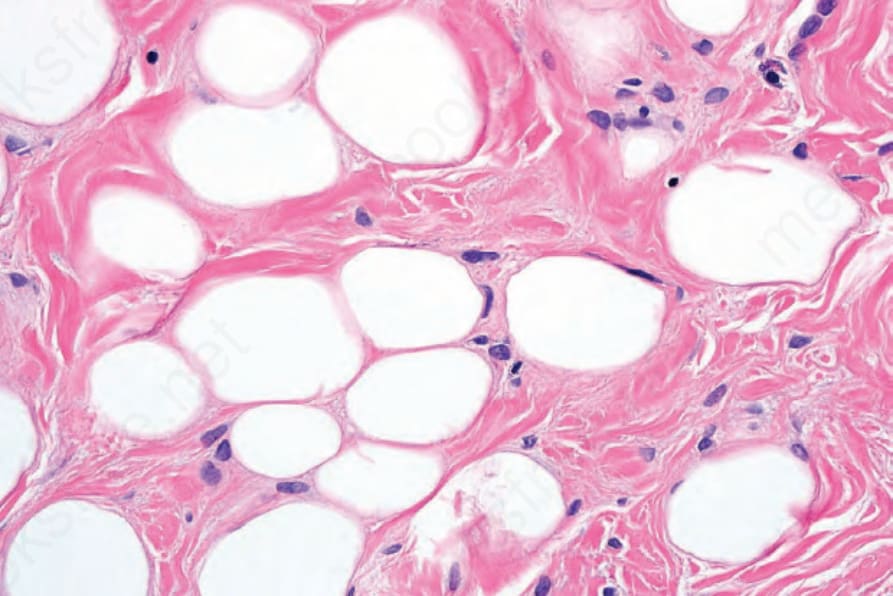
Fig. 35.5 Fibrolipoma: high-power view of Figure 35.4.
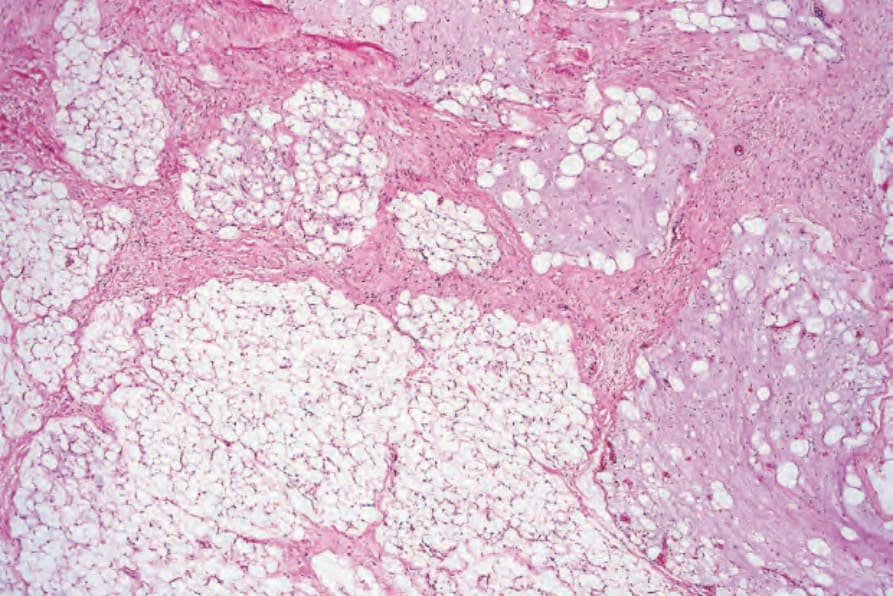
Fig. 35.6 Myxofibrolipoma: this variant of lipoma is characterized by fibrosis and foci of myxoid change. It is of no clinical significance.
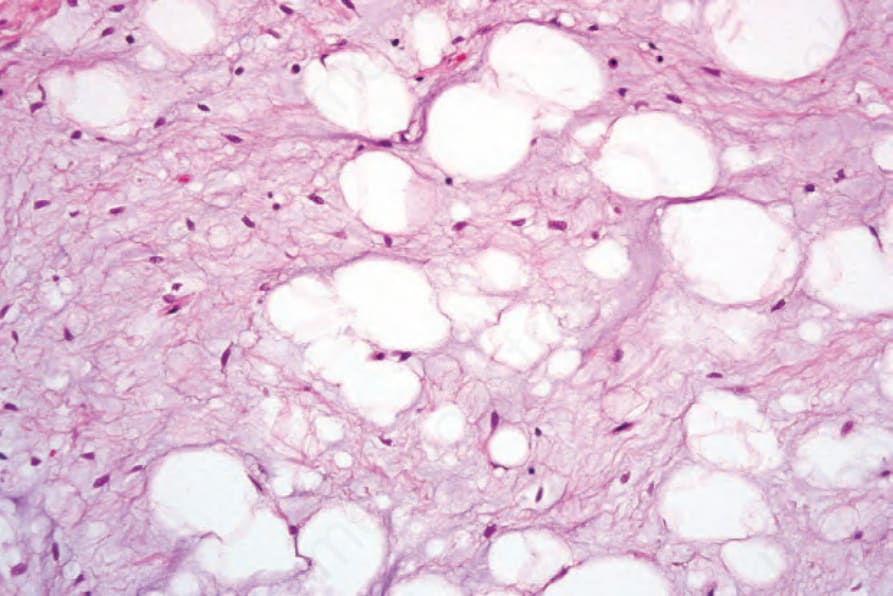
Fig. 35.7 Myxofibrolipoma: note the abundant mucinous matrix and spindled cells admixed with adipocytes.
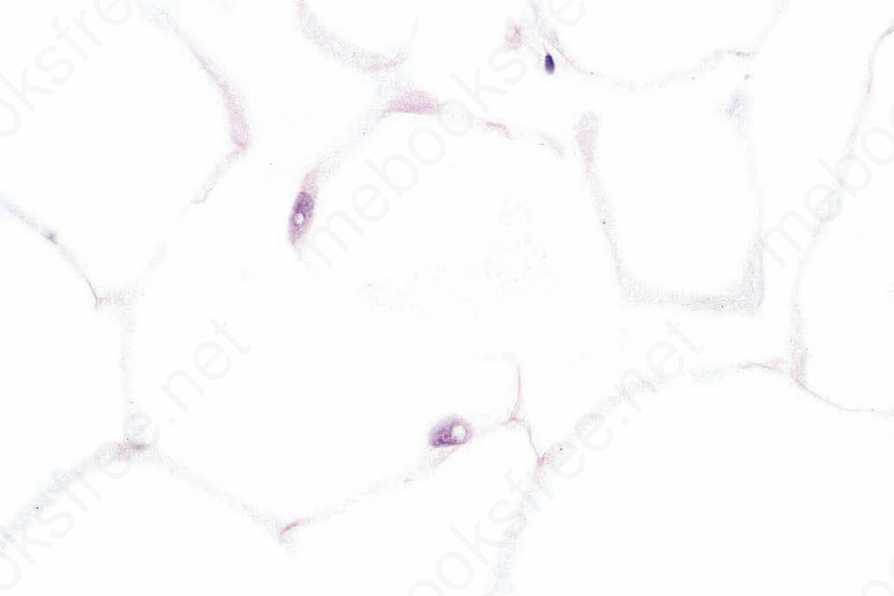
Fig. 35.8 Lipoma: intranuclear lipid ‘inclusions’ (lochkern) should not be mistaken for lipoblasts.
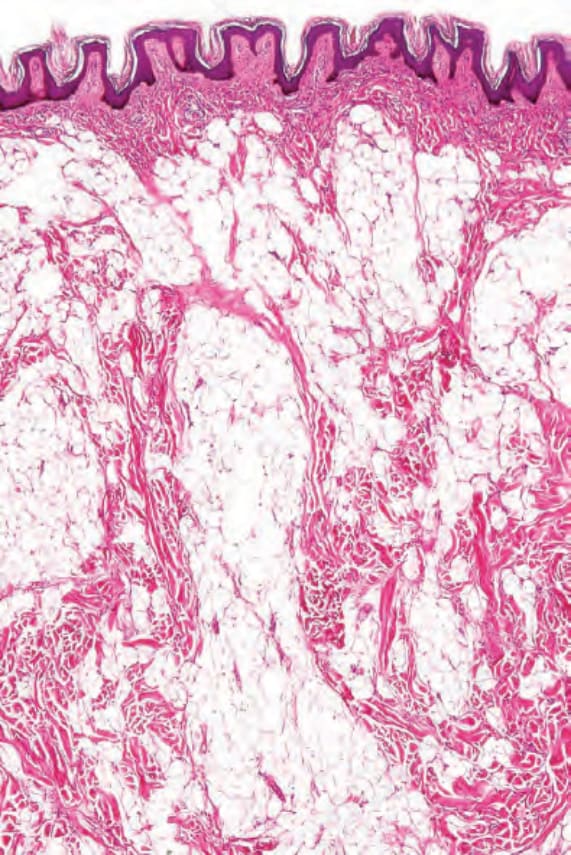
Fig. 35.9 Dermal lipoma: the dermal variant is often less well circumscribed and tends to dissect between the collagen fibers.
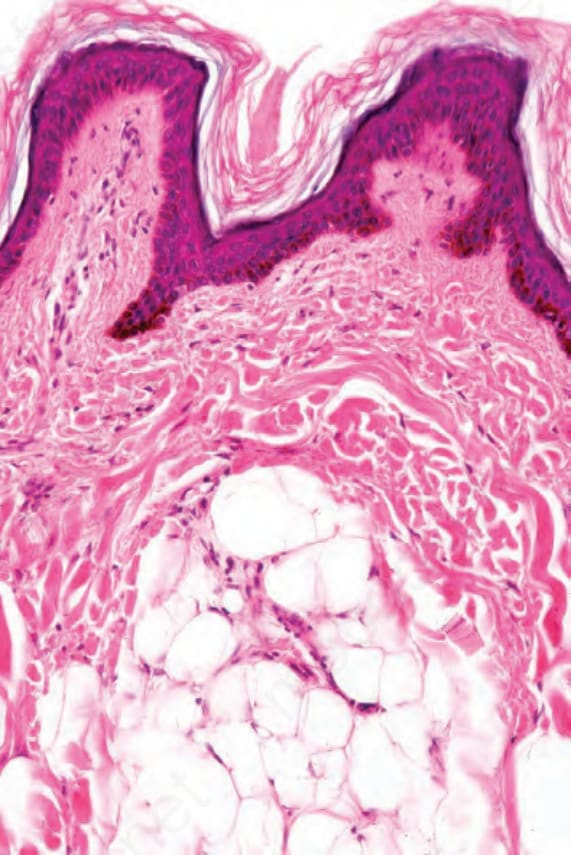
Fig. 35.10 Dermal lipoma: it is often separated from the epidermis by a grenz zone.

Fig. 35.11 Nevus lipomatosus superficialis: solitary lesions are often polypoid and have a soft consistency. By courtesy of the Institute of Dermatology, London, UK.