Umbilical polyp and granuloma
Umbilical polyp and granuloma
Pathogenesis and histologic features When first described, mucinous syringometaplasia was thought to represent a benign tumor – muciparous epidermal tumor.1 Currently, however, it is generally believed to represent a metaplastic phenomenon principally affecting the superficial eccrine ducts and very rarely the apocrine duct.9 The etiology is unknown although chronic trauma, pressure, and inflammation have been suggested as possible causes.6,7
The congenital umbilical polyp represents persistence of the distal-most segment of the vitelline (omphalomesenteric) duct, which connects the small intestine of the early fetus to the yolk sac. It usually disappears by about the seventh week of gestation. The most common manifestation of persistence is Meckel diverticulum, and the most serious consequence is an intestinal– umbilical fistula.1 Cutaneous manifestations include polyps, sinuses, and cysts.2–5,6 Less often, an umbilical polyp may arise from urachal remnants (urachal sinus or cyst).7
Clinical features The lesions are usually noticed at birth, but presentation of sinuses and cysts may be delayed for days or years. Exceptionally, the lesion may not appear until late adulthood.8 There is a marked predilection for males (6:1). The patient commonly presents with a bright red, 1- to 4-cm diameter pyogenic granuloma-like polyp on the umbilicus; secretions sometimes cause it to feel rather sticky or mucinous, and there may be damage to the surrounding skin, caused by acid or enzymes.2,3
Histologically, it is usually characterized by an epidermal invagination which is continuous at its base with eccrine ducts lined by nonkeratinizing squamous and mucin-containing epithelium (Figs 34.42 and 34.43).5–7 These latter are sometimes seen in the epidermis, and goblet cells are often evident.6 There is no significant pleomorphism and mitoses are sparse or absent.6,8 The adjacent epidermis is hyperkeratotic, focally parakeratotic, and markedly acanthotic.7 The underlying dermis commonly contains a heavy chronic inflammatory cell infiltrate with conspicuous plasma cells; fibrosis is often present.6 In some cases, the ducts are continuous with the underlying dermal eccrine sweat ducts.5 In one case, the changes extended to the eccrine secretory coil.3 In other cases, no such continuity is demonstrable.1,7,8
The mucin-containing cells are positive for diastase–PAS, mucicarmine, colloidal iron (with and without hyaluronidase), and Alcian blue at pH 1 and 2.5.5,7
The umbilical granuloma represents a granulation tissue polyp which sometimes develops in the umbilicus soon after separation of the cord. It is likely to be related to infection and presents as a 1.0-cm diameter or greater red polypoid lesion.
Histologic features The polyp is associated with abrupt transition from stratified squamous to glandular epithelium of gastric, small intestinal, or colonic type (Figs 34.44 and 34.45).9 Smooth muscle components of the bowel wall are sometimes present. Pancreas has also been identified.8 Urachal lesions are composed of transitional cell epithelium.
The granuloma is composed of inflamed vascular granulation tissue.
1697 Pseudocyst of the auricle
A
B
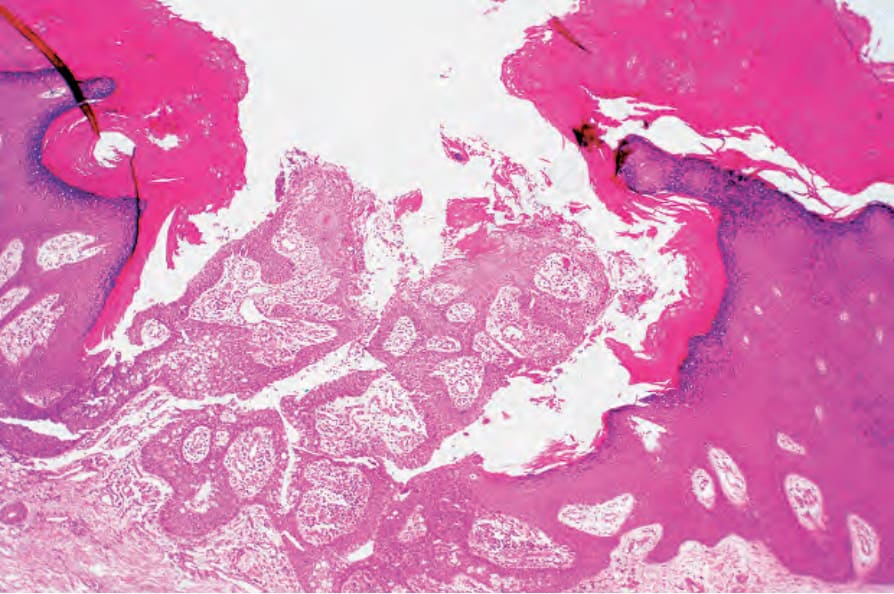
Fig. 34.42 Mucinous syringometaplasia: this lesion comes from the palm of the hand. Within the center of the defect are two epithelial-lined papillae. By courtesy of J. Grant, MD, Worthing Hospital, Worthing, UK.
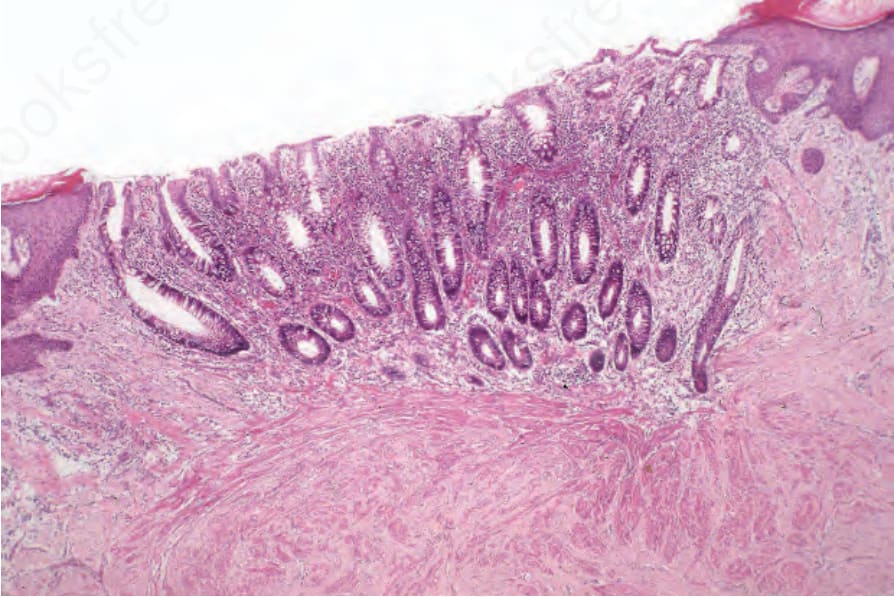
Fig. 34.44 Congenital umbilical polyp: in this example, the surface of the polyp is covered by large intestinal mucosa. Note the tubular glands. The fascicles of smooth muscle deep to the epithelium represent muscularis mucosae.
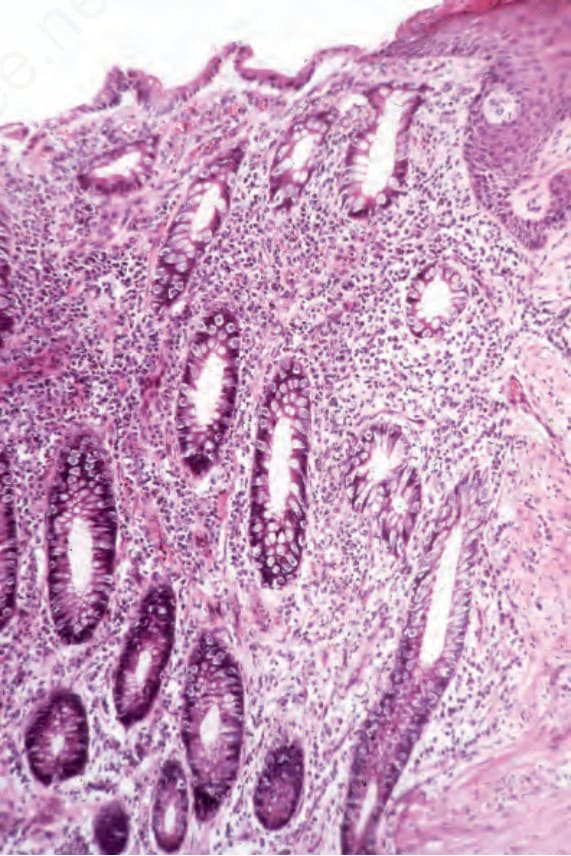
Fig. 34.45 Congenital umbilical polyp: note the continuity between the columnar and squamous epithelium.
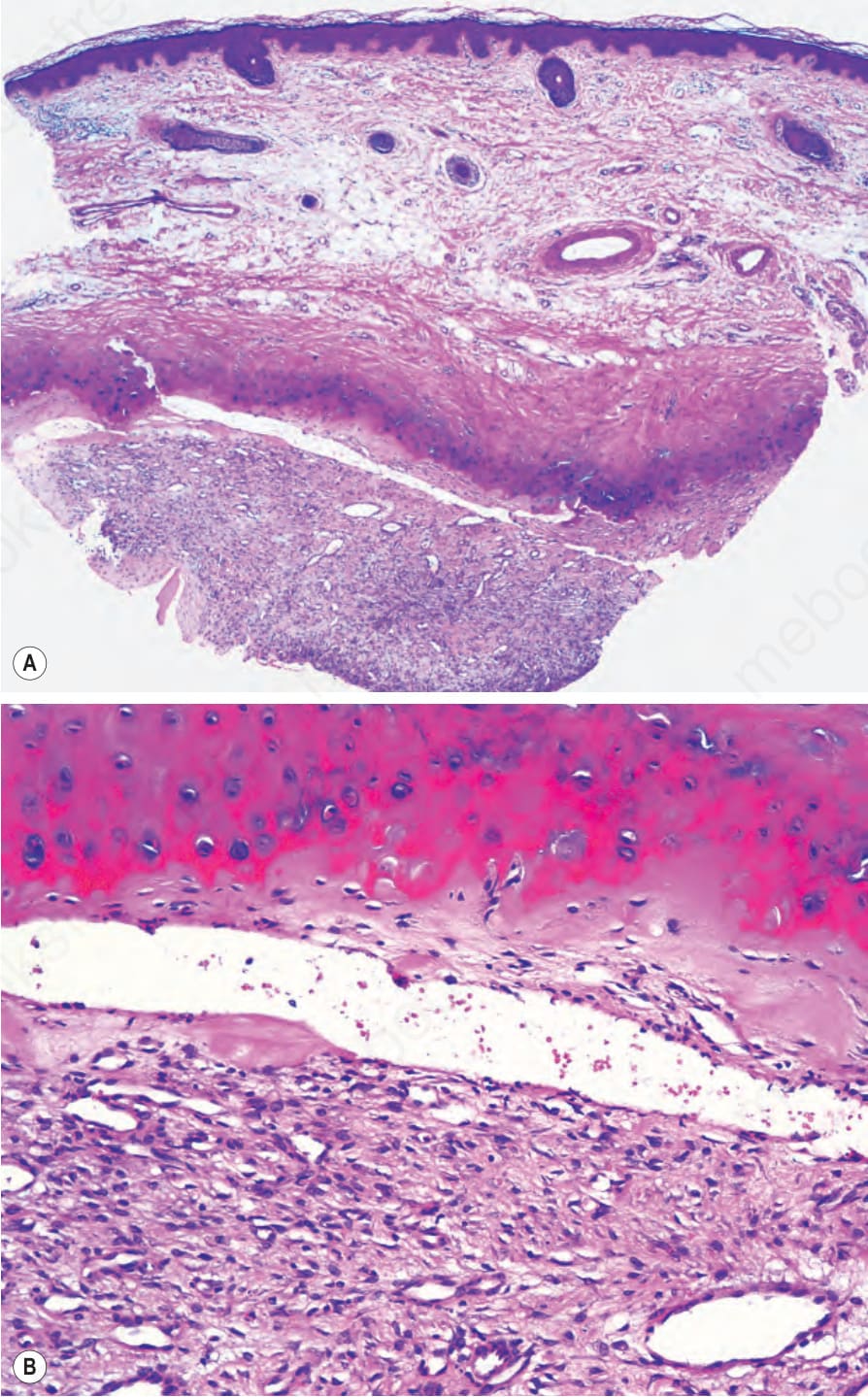
Fig. 34.46 Pseudocyst of the auricle: (A) cystic space within the cartilage; (B) the cavity is occupied by granulation tissue.