Pilonidal sinus
Pilonidal sinus
Clinical features Pilonidal sinus (jeep disease) is a fairly common condition which shows a predilection for males (3–4:1) and presents most often in the second two decades.1–4 Caucasians are predominantly affected.3 The disease is very uncommon in blacks and exceptionally rare in Asians.3 Although patients may very rarely be asymptomatic, the typical history is of a chronic painful draining sinus or multiple sinuses affecting the base of the spine or the intergluteal cleft.2 Similar lesions have been described on the ear, scalp, chest, umbilicus, penis, vulva, anal canal, and axilla.5–12 Similar interdigital variants may be encountered in barbers, hairdressers, sheep shearers, cow milkers, and dog groomers as a reaction to hair embedded in the dermis.13–19 A subungual form has also been documented.20
1695 Mucinous syringometaplasia
A
There are a small number of reports of malignancy supervening in chronic sacrococcygeal pilonidal sinus with an estimated incidence of around 0.1%.21–24
Pathogenesis and histologic features The sacrococcygeal variant appears to develop as a consequence of the patient’s own hair penetrating the skin directly or via dilated follicular ostia.2–4 Free hair in the gluteal cleft rubs against the adjacent skin and the friction from movement of the buttocks propels the shaft through the epithelium into the dermis where a foreign body granulomatous reaction results. It also results in a nidus for secondary infection and abscess formation.3 Epstein-Barr virus-infected lymphocytes predominantly with a B phenotype have been found in more than half of the cases of pilonidal sinus in a study.25 This is not thought to be related to the pathogenesis of the disease.
B
Superficially, the sinus is often lined by stratified squamous epithelium but toward the deeper reaches the wall consists of granulation and scar tissue surrounding intensely inflamed dermis containing one or more hair shaft fragments (Figs 34.39 and 34.40). Abscesses are commonly present, and foreign body multinucleate giant cells are usually conspicuous. Secondary infection with bacteria including Actinomyces may be seen.26
diagnosis or misdiagnosis.8 Lesions may appear at a variety of sites on the head and neck, but the chin, submental region, and the cheek are most often affected (Fig. 34.41).1 The lesion typically heals when the dental infection is cured.
Histologic features Biopsy findings are non-specific and include a mixed inflammatory cell infiltrate with abscess formation and scarring, sometimes associated with a foreign body granulomatous component.
The rare malignancies are generally well-differentiated squamous cell carcinomas.27 Morbidity and mortality are significant with local recurrence and metastasis in around a third of cases.21 Immunosuppression can augment or complicate malignant degeneration.22 Verrucous carcinoma has also been noted.23 Very occasionally, basal cell carcinoma has been described and there is one example of adenocarcinoma.28,29
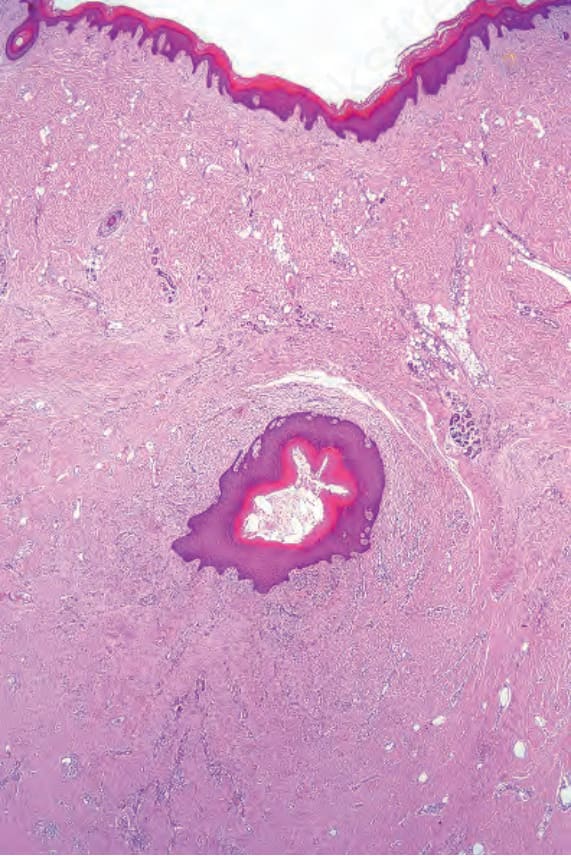
Fig. 34.39 Pilonidal sinus: the sinus is lined by stratified squamous epithelium. Note the surrounding scar tissue, chronic inflammation, and hemosiderin deposition.
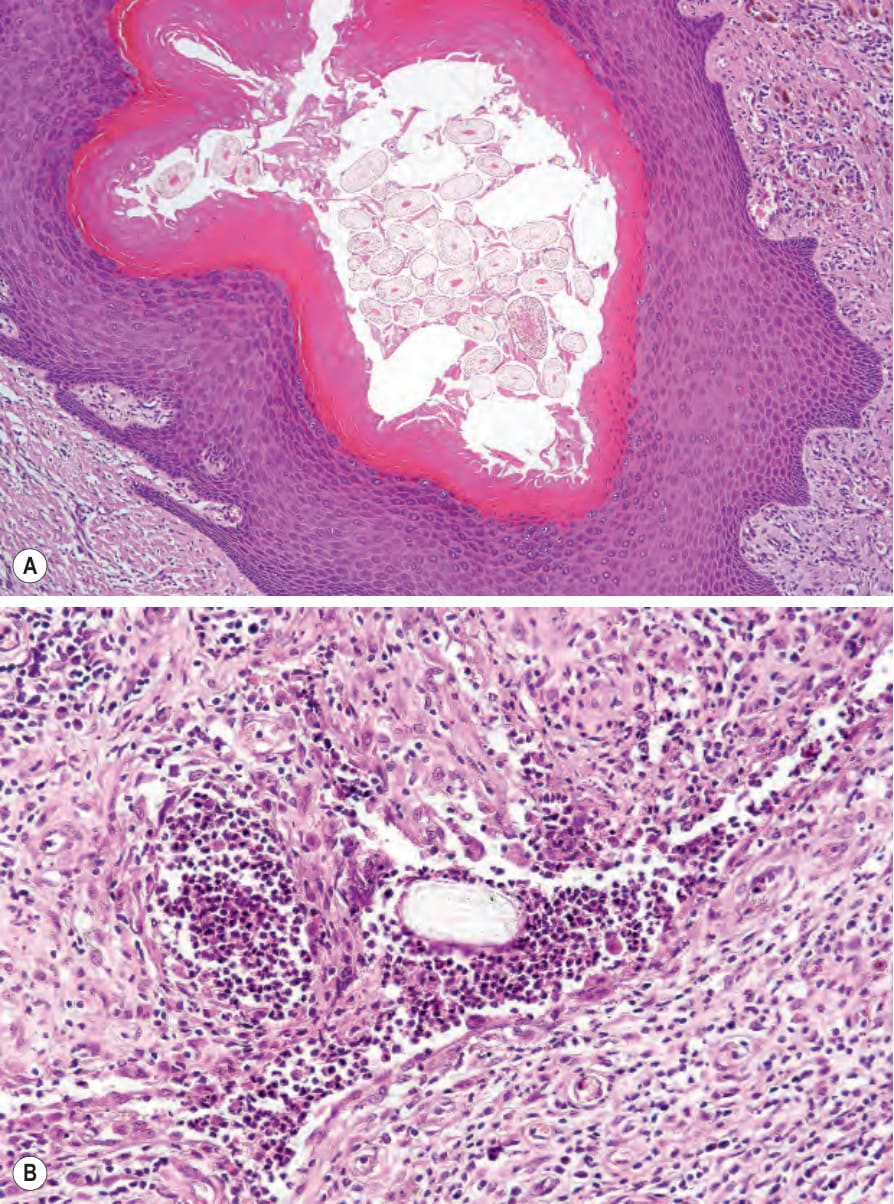
Fig. 34.40 (A, B) Pilonidal cyst: multiple hair shaft fragments are evident.

Fig. 34.41 Dental sinus: the chin is a commonly affected site. By courtesy of the Institute of Dermatology, London, UK.