Median raphe cyst
Median raphe cyst
Clinical features Median raphe cysts (genitoperineal raphe cyst, parameatal cyst) are usually up to 1 cm across, contain clear fluid, and are most often noticed in the first three decades of life as an asymptomatic nodule, sometimes translucent, on the ventral aspect of the penis.1–10 Rare lesions present as a cordlike or canal-like induration.11 The glans is the most commonly affected site.5 Lesions may also be seen along the ventral surface of the scrotum and on the perineum.12–17 Perianal lesions are exceptional.18 The cyst does not communicate with the urethra. Recurrences are uncommon.1 Rarely, cysts develop in association with split median raphe.19
A
Pathogenesis and histologic features The cyst is generally believed to result from anomalous fusion of the genitourethral folds and urethral plate, with resultant misplaced nests of urethral epithelium in the ventral midline.11 Alternatively, some examples may result from misplaced periurethral glands (mucoid cyst) or aberrant urethral buds.2,5 Similar malfusion of the labial–scrotal folds results in scrotal and perineal variants.12
Histologically, the cyst lining is variable. In most reports it consists of pseudostratified columnar epithelium, 1–4 cells thick (Fig. 34.35).1,2,5 Uncommonly, diastase-resistant, periodic acid-Schiff (PAS)-positive mucinous, and stratified squamous epithelia are present (Fig. 34.36).1,8,13 Glandular
B
1694 Cutaneous cysts
A
formation is very rare.20 Metaplastic ciliated variants and admixed goblet cells are very occasionally seen.9,10,13 Exceptionally, pigmented variants associated with intraepithelial dendritic melanocytes may be encountered.6,21 One publication described linear small epidermoid cysts extending along the median raphe of the scrotum to the anal verge of a male infant. These may have resulted from entrapped squamous epithelial rests during the development of the raphe scroti.12
The epithelial cells are CK7 and CEA positive, and CK20 negative.7,8 Focal neuroendocrine differentiation characterized by chromogranin and synaptophysin expression has been documented in two cases.8
Differential diagnosis The midline site, the predominant pseudostratification, and the lack of both decapitation secretion and a myoepithelial layer distinguish median raphe cyst from apocrine cystadenoma. In addition, median raphe cysts do not express human milk fat globulin 1 (HMFG-1).7
B
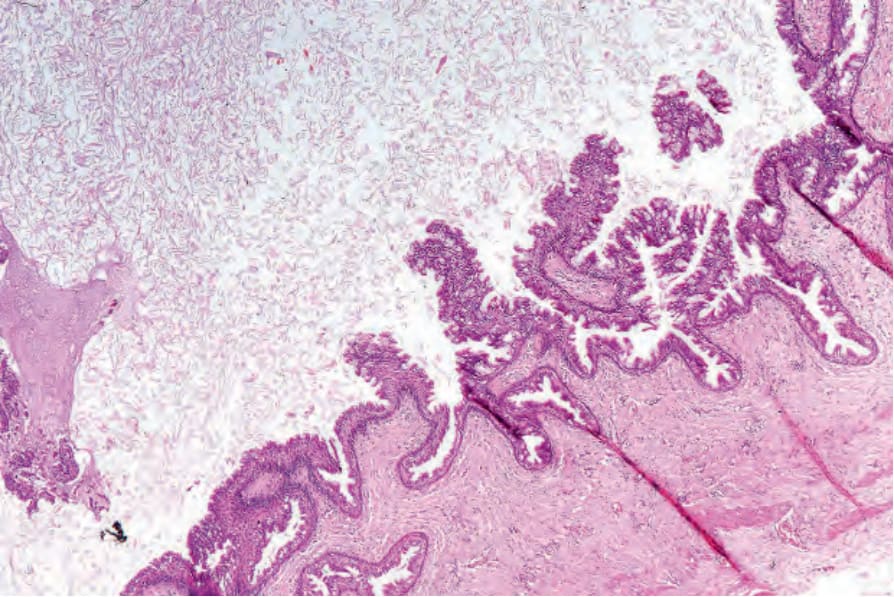
Fig. 34.35 Median raphe cyst: low-power view showing papillary processes covered by columnar epithelium.
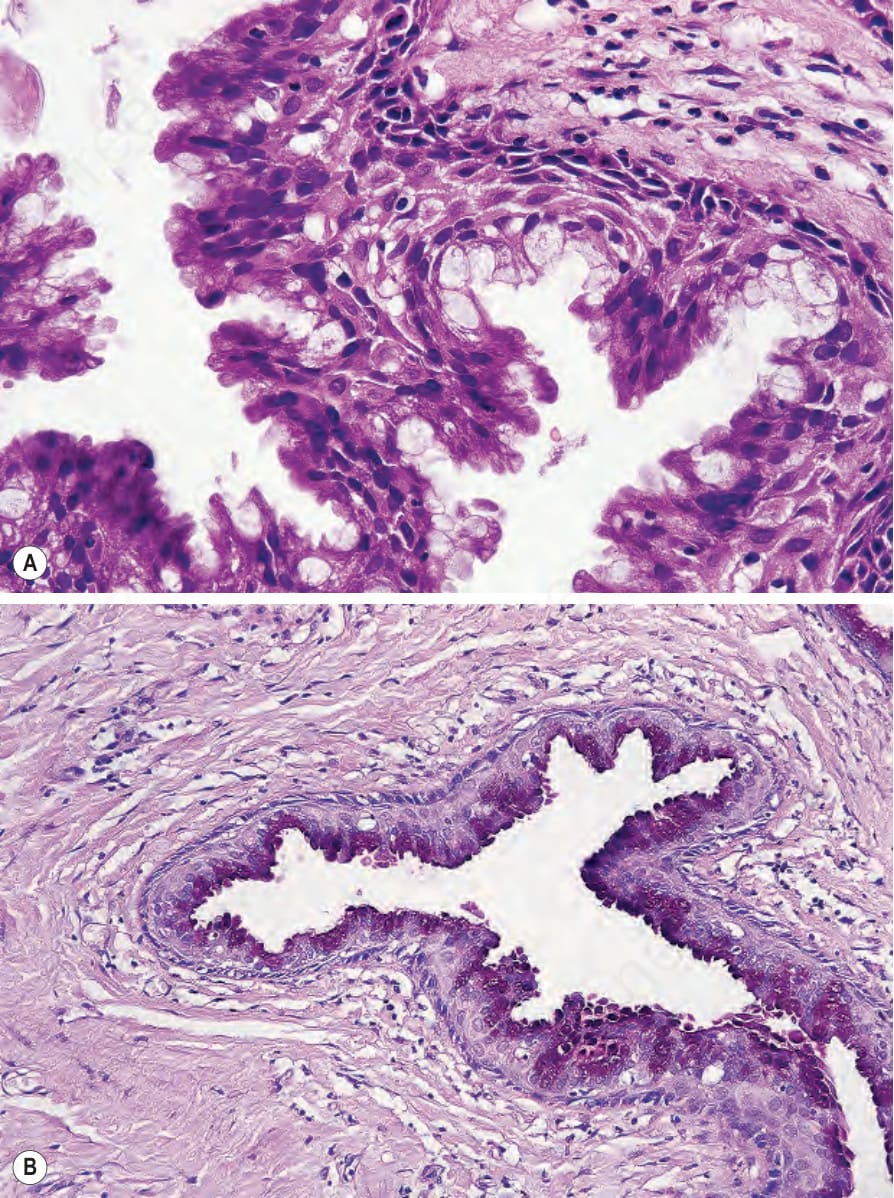
Fig. 34.36 Median raphe cyst: (A) the cyst is focally lined by mucus-containing epithelium; (B) the latter is PAS positive (diastase resistant).
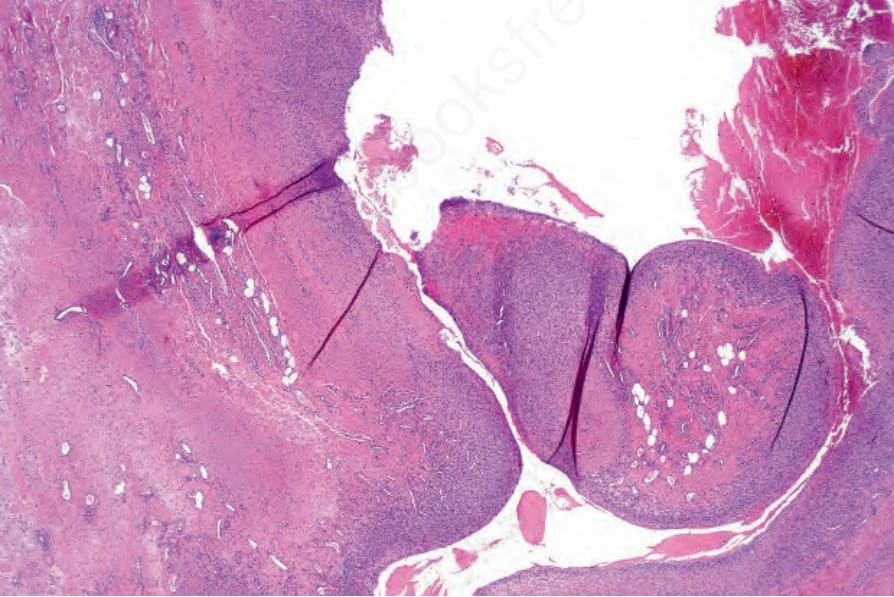
Fig. 34.37 Metaplastic synovial cyst: this example presented as a fistulous tract following abdominal surgery. Villous processes are evident.