Cutaneous ciliated cyst
Cutaneous ciliated cyst
Clinical features The term cutaneous ciliated cyst (cutaneous Müllerian cyst) most often refers to a solitary lesion which presents shortly after the menarche on the limb (including the digits) of young females (12–42 years).1–13 The thigh, buttock, calf, and foot are affected, in decreasing order of frequency. The cysts are located in the deep dermis and/or subcutaneous tissue and are usually asymptomatic.4 Occasionally, they become inflamed and painful and sometimes they rupture. Identical lesions have been described on the abdominal wall.14,15
It is lined by stratified squamous or pseudostratified ciliated columnar epithelium (Fig. 34.32). Its wall typically contains lymphoid tissue in which germinal centers are usually conspicuous.3 Occasionally, seromucinous glands may also be evident.2 A case of nasopharyngeal branchial cleft cyst harboring a lymphoma and rare cases with a squamous cell carcinoma and papillary thyroid carcinoma (probably arising from ectopic thyroid tissue) have been reported.8–14 In such cases, it is important to rule out a cystic lymph node metastasis from a primary elsewhere. It is important not to confuse a branchyal cyst with a rare cystic metastasis of a well-differentiated ciliated HPV-related carcinoma.15
Lesions have occasionally been described in males and at atypical sites including the back, shoulder, scalp, cheek, and scrotum.16–24 These might better be classified as separate, distinct entities.
Pathogenesis and histologic features Two theories have been proposed to explain the development of ciliated cysts. Those lesions which present on the limbs of young females are generally thought to be of Müllerian (paramesonephric) derivation, their presence representing a migration abnormality of fetal development (heterotopia).2,3 In support of this hypothesis, authors have cited the close proximity of the paramesonephric duct to the developing limb bud, the striking predilection for females, the histologic similarity between the lining epithelium and that of the fallopian cord, and the absence of sweat glands in the near vicinity of the cyst wall.13 Cysts arising at other sites and in males may represent metaplasia of the lining of a preexistent simple cyst of sweat duct derivation or else an entirely different histogenesis (see differential diagnosis).5
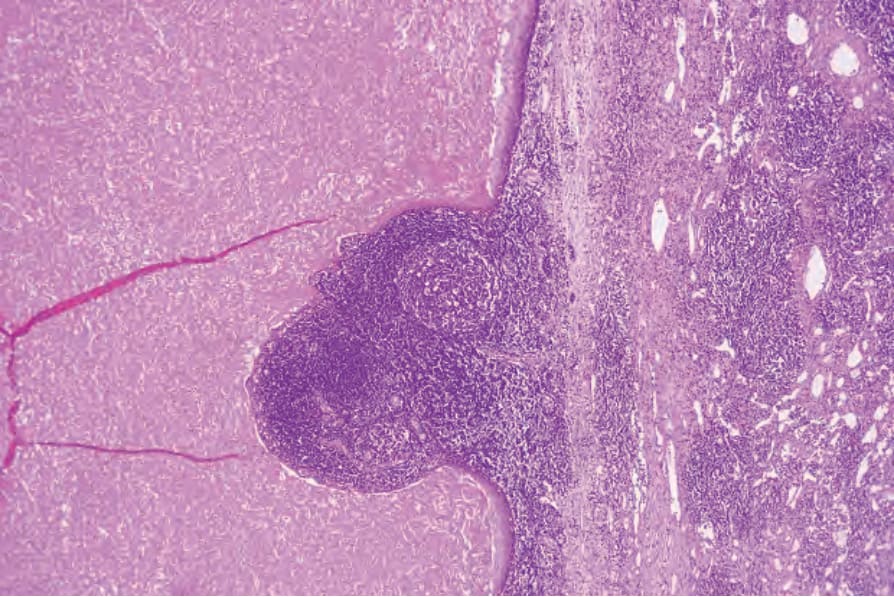
Fig. 34.32 Branchial cyst: the wall is composed of stratified squamous epithelium. Note the intense lymphocytic infiltrate.