Thyroglossal duct cyst
Thyroglossal duct cyst
Clinical features The thyroglossal duct cyst, which is a congenital anomaly representing a vestigial remnant of the tubular thyroid gland precursor, may present at any age including adulthood (predominantly in the fifth decade of life), but children in the first decade of life are most often affected.1–10 Lesions are more common in males in children and in females in adults.10 It is commonly found in the midline of the neck in the region below the hyoid bone as a fluctuant swelling up to 3 cm in diameter. It characteristically moves with swallowing.11 The development of an associated sinus is a not uncommon complication more frequently seen in children.10,12 An exceptional case of a recurrent lesion presenting with cutaneous blisters has been reported.13
Pathogenesis and histologic features Bronchogenic cysts are believed to form from buds or diverticula that separate from the foregut during the development of the tracheobronchial tree; they may be intrapulmonary or peripheral. Cutaneous bronchogenic cysts may result from subsequent sequestration outside the chest cavity following fusion of the mesenchymal bars of the sternum or else from active migration prior to fusion.13,14 Lesions overlying the scapula likely arose before the scapula developed, at the sixth week of gestation.6
Very occasional familial variants have been reported.14 Most of these have displayed an autosomal dominant mode of inheritance although recessive forms are also recognized.15–17 Although the number of documented families is small, there appears to be a predilection for females.14
Recurrence following surgery is low, varying from 2% to 6% of cases.14,18
Pathogenesis and histologic features Thyroglossal duct cysts, which are variably lined by cuboidal, columnar, or stratified squamous epithelium, are frequently accompanied by an epithelial-lined tract.1 Ciliated epithelium is also often present. The epithelial lining may be exclusively respiratory, squamous, or more often, in about half of the cases, a mixture of both.10 In around 1% of cases, no epithelial lining is seen.10 The adjacent tissues may show mucous glands, thyroid follicles (in 71% of cases), and a heavy lymphocytic infiltrate (Fig. 34.31). Occasionally, skin appendages (including hair follicles and sebaceous and sweat glands) are additionally found, resulting in histologic overlap with a dermoid cyst – the so-called mixed or hybrid cyst.2,6 Smooth muscle is not present but skeletal muscle and adipose tissue are commonly seen.10 In most cases, the hyoid bone is identified.10
The cutaneous bronchogenic cyst is situated within the dermis or subcutaneous tissue, and usually its lining is thrown into small folds. The epithelium is invariably pseudostratified cuboidal or columnar and ciliated, with mucus-secreting goblet cells in about 50% of cases.2,13 Nonciliated cuboidal, columnar, and stratified squamous epithelium may also be identified. Smooth muscle supports the mucosa in 8% of cases.1,12,13 Lymphoid follicles are found in only 25% of cases and then appear to be part of a secondary inflammatory response.1 Seromucinous glands are also sometimes present.2,5,12 Cartilage is evident in a minority of cases.4,6,10,13 Not all of these features are necessarily present in any one particular cyst, and the diagnosis may then be in part dependent on clinicopathological correlation.8,9
Occasionally, histologic examination may reveal ectopic thyroid gland, thyroid adenoma, and in approximately 1% to 3% of cases, carcinoma.10,19–26 The last are most often papillary adenocarcinoma, but follicular and squamous variants have also been described.10,11 They sometimes represent an incidental finding following excision.
1692 Cutaneous cysts
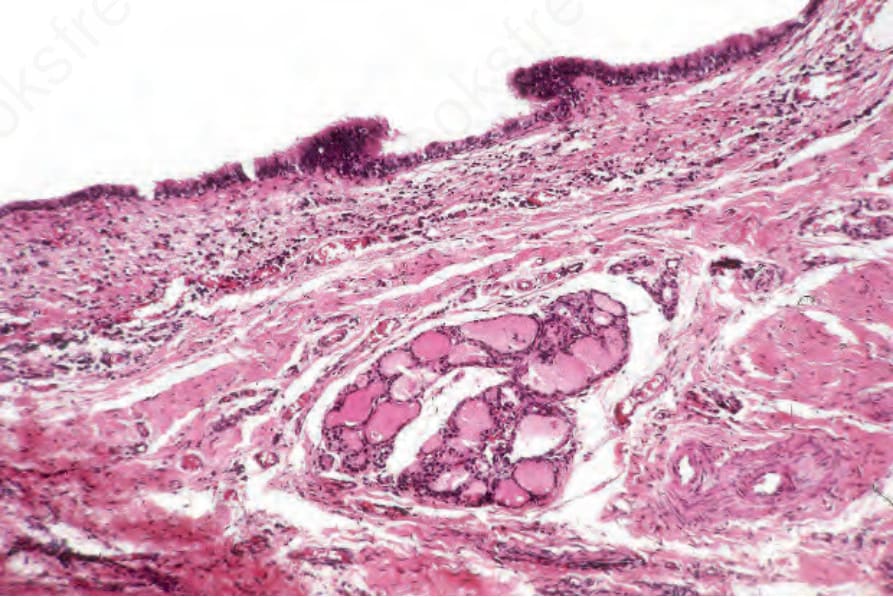
Fig. 34.31 Thyroglossal duct cyst: the cyst is lined by tall columnar epithelium. Note the colloid-containing thyroid follicles.
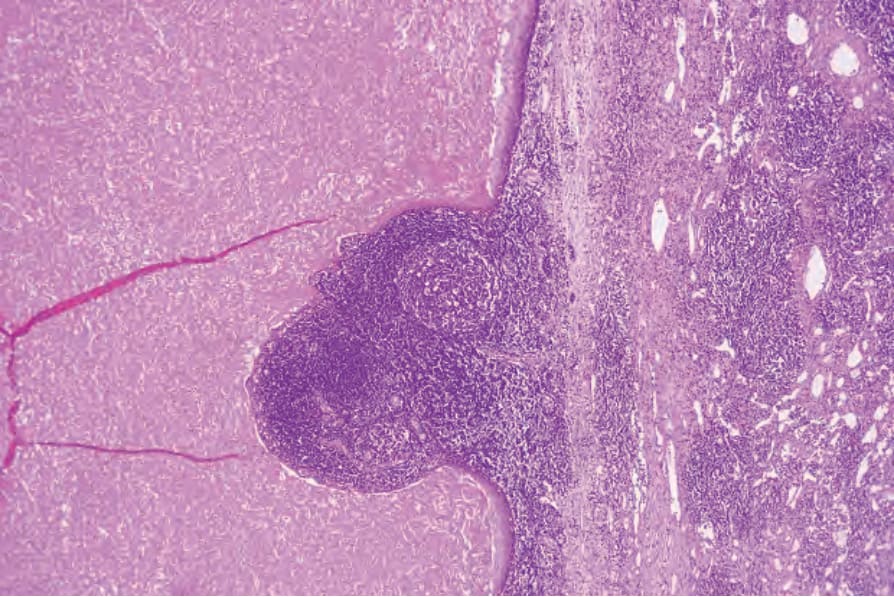
Fig. 34.32 Branchial cyst: the wall is composed of stratified squamous epithelium. Note the intense lymphocytic infiltrate.