Dermoid cyst
Dermoid cyst
Clinical features Dermoid cysts result from the sequestration of cutaneous tissues along embryonal lines of closure.1–5 The most common clinical appearance is that of a single nontender small subcutaneous nodule at birth on the lateral aspect of the upper eyelid (Fig. 34.27). Although slow enlargement is the rule, sometimes a sudden increase in size may occur, bringing the lesion to attention at a later age. Other potential sites of dermoid cysts include the midline of the neck, nasal root, nose, forehead, the mastoid area, anterior chest, and scalp.3,6–8 The last is a particularly important site as the lesion may very occasionally show intracranial extension (dumbbell dermoid).3,4 Midline occipital lesions are most often affected.3 Dermoid cysts may also
1690 Cutaneous cysts
A
B
present on mid chest, sacrum, perineum, scrotum, penis, and ear.5,9 Dermoid cysts are also encountered in the oral cavity and deeper noncutaneous sites.
Infection of a cranial dermoid cyst is a serious development as it may be complicated by central nervous system involvement.3 Squamous cell carcinoma very rarely develops in the wall of the cyst.10,11 Exceptionally, the development of carcinosarcoma has been described.12 There are occasional reports of familial dermoid cysts, including one family associated with midline cleft lip.13–15
Pathogenesis and histologic features The unilocular cysts are usually subcutaneous and may be attached to the periosteum. They are lined by stratified squamous epithelium with associated
hair follicles and sebaceous glands (Fig. 34.28). Trichilemmal differentiation is exceptionally seen in the lining of the cyst.16 Eccrine sweat glands are present in 35% of cases and apocrine glands in 15%. Smooth muscle can be present but – in contrast to benign cystic teratoma – cartilage and bone are not described. Some authors propose an embryological origin for these cysts, particularly in the nasal form.17
Antenatal diagnosis has been reported.13
Differential diagnosis Dermoid cyst should be distinguished from congenital dermoid fistula, which presents at birth as a superficial fistula tract (Figs 34.29 and 34.30).18–20
1691 Glandular cysts

Fig. 34.27 Dermoid cyst: note the swelling adjacent to the upper eyelid – the external angular dermoid cyst. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
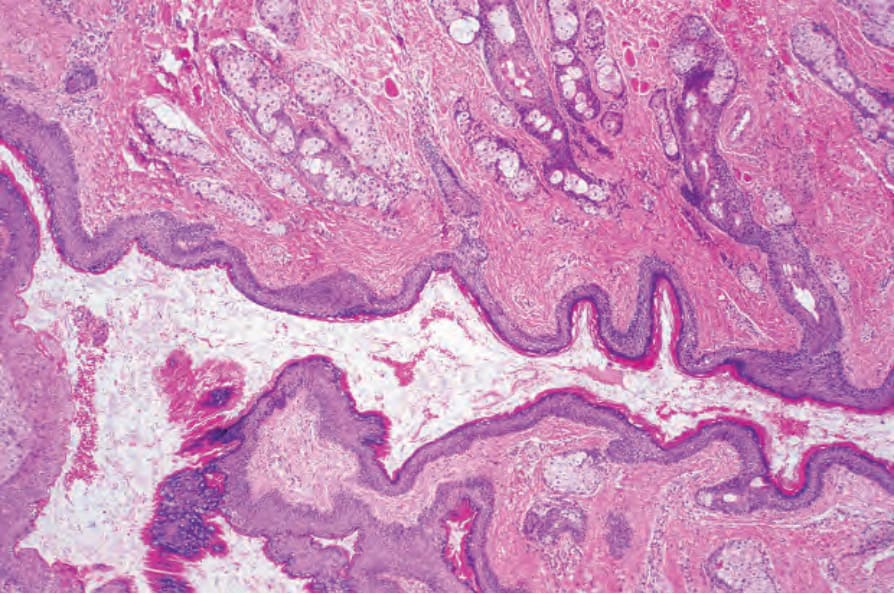
Fig. 34.28 Dermoid cyst: the cyst is lined by stratified squamous epithelium. Note the numerous sebaceous glands.
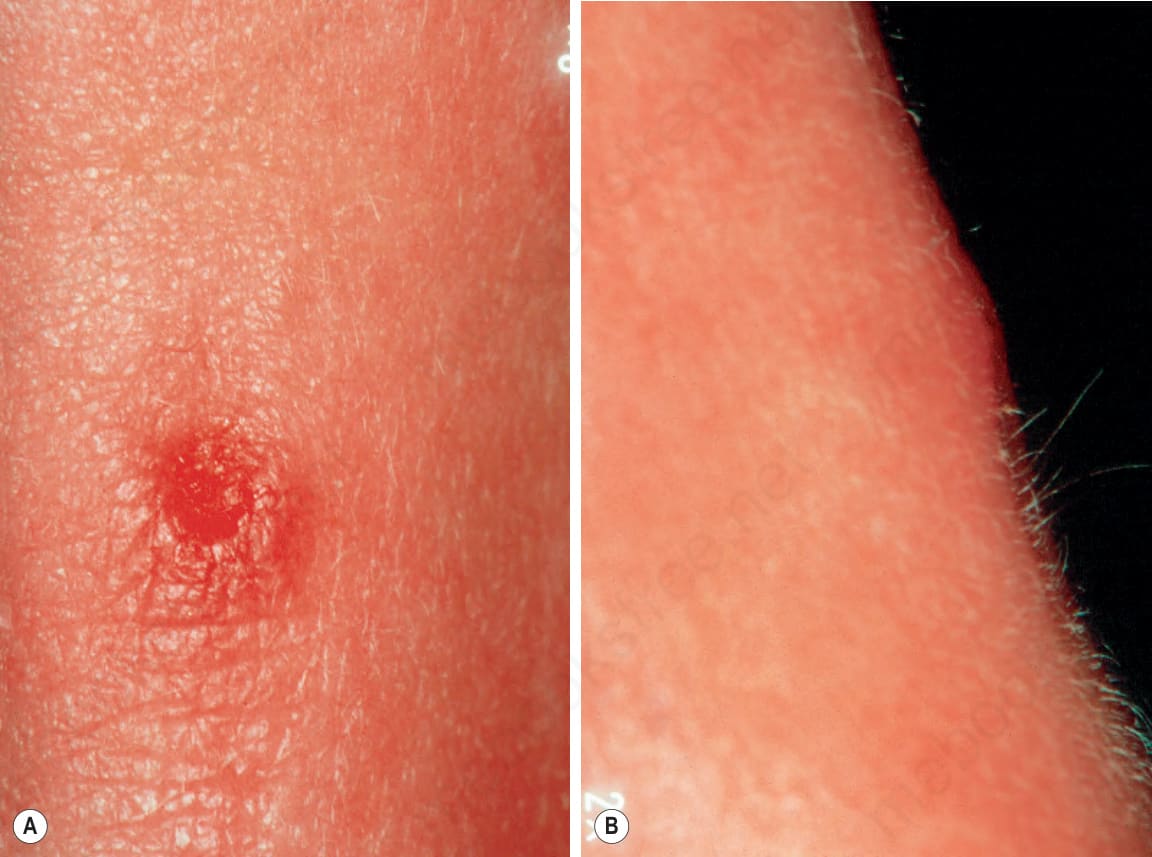
Fig. 34.29 Median nasal dermoid fistula: (A) on the dorsum of the nose is an erythematous crateriform depression; (B) the presence of protruding white hairs is characteristic. By courtesy of D. Shuttleworth, MD, Chichester, UK.
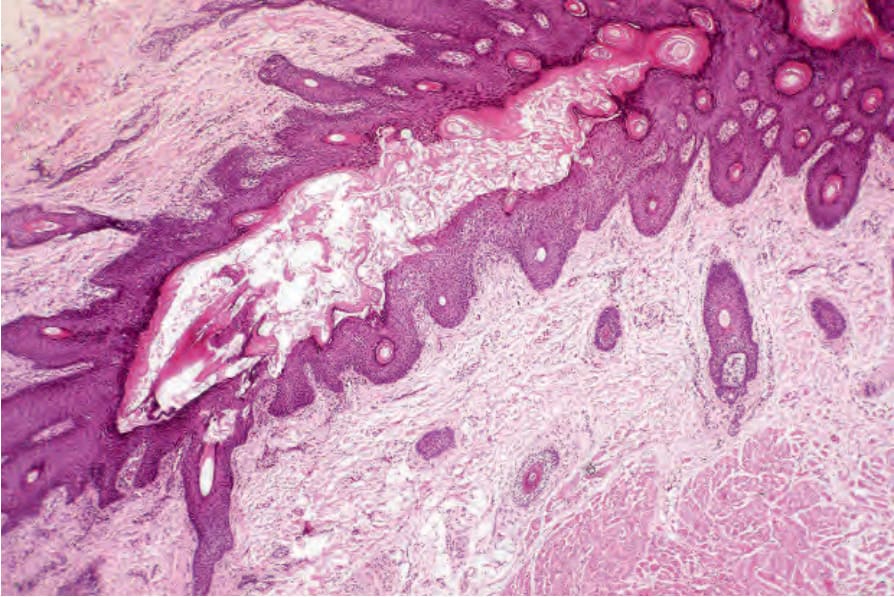
Fig. 34.30 Median nasal dermoid fistula: the fistula, which communicates with the surface epidermis, is lined by hair-bearing epithelium. By courtesy of D. Shuttleworth, MD, Chichester, UK.
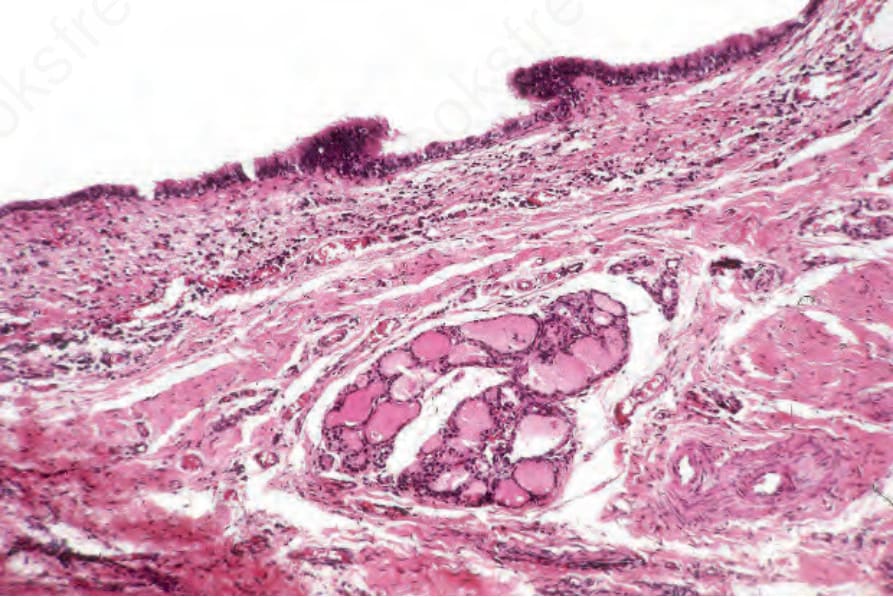
Fig. 34.31 Thyroglossal duct cyst: the cyst is lined by tall columnar epithelium. Note the colloid-containing thyroid follicles.