Vellus hair cysts
Vellus hair cysts
Clinical features Vellus hair cysts were originally reported in children and young adults of both sexes.1–4 The sex distribution is equal and there is no racial predilection. Patients present with numerous asymptomatic, discrete, soft, flesh-colored or reddish-brown papules, 1–5 mm across, particularly over the parasternal area, although the distribution may be quite widespread.4 A generalized distribution has been documented.5 An exceptional case mimicking a nevus of Ota has been described.6 Lesions may rarely be unilateral.7 Occasional lesions are umbilicated, and squeezing may express white caseous material. Further cases have expanded the condition to include an inherited (autosomal dominant) variant, which may or may not be manifest at birth and is more likely to occur over the extensor aspects of the limbs.3,8,9 Occurrence in twins has been reported.10 A facial form, a patient presenting with a periorbital distribution, and a further patient with a single orbital lesion have been described.11–14 Spontaneous involution is not uncommon.2,15
A
Vellus hair cysts have occasionally been associated with renal failure and a number of genodermatoses including pachyonychia congenita, anhidrotic ectodermal dysplasia, hidrotic ectodermal dysplasia, and rarely, Lowe syndrome (oculocerebrorenal syndrome characterized by Fanconi-type renal failure, mental retardation, and ocular abnormalities).16–20 Occasionally, solitary lesions are encountered and may be large.21
Pathogenesis and histologic features Eruptive vellus hair cysts most probably develop as a consequence of occlusion of the infundibulum of vellus hairs with resultant cystic dilatation and retention of keratinous debris and vellus hairs.2 The primary cause of the obstruction is unknown. It has also been proposed that they represent follicular hamartomas.8 Studies indicate that both eruptive vellus hair cysts and steatocystomas express keratin 17, with the latter also expressing keratin 10.22,23 This overlap in keratin expression may help explain the underlying similarities and perhaps overlapping features of these two lesions; however, this opinion is not universal, and their exact relationship remains to be elucidated.24–26
B
The characteristic histology is that of a mid-dermal cyst containing laminated keratin and many vellus hairs (Figs 34.25 and 34.26).2,4,15 The epithelial lining consists of several layers of squamous epithelium, often with a granular cell layer. Sometimes the cyst is in continuity with the epidermis, an atrophic follicle, or a pilomotor muscle.3,4,15 Vellus hair cysts are more likely to open onto the surface in the congenital variant. Occasionally the cyst ruptures, and there is an associated foreign body giant cell reaction that may be associated with formation of cholesterol clefts.27
Differential diagnosis Eruptive vellus hair cysts show very marked clinical overlap with steatocystoma multiplex and can only be distinguished by histologic analysis.28 Steatocystoma is characterized by an epidermoid lining without a granular cell layer. The innermost aspect of the cyst wall is covered by an undulating eosinophilic cuticle. Sebaceous glands are present in the wall of the cyst or in the immediate vicinity.
Sometimes, however, patients have both types of cyst simultaneously, and occasionally there are overlapping histologic features sometimes constituting a hybrid cyst.28–30
1689 Follicular cysts
As noted above, differential keratin expression has been shown to distinguish the two cysts. Thus vellus hair cyst expresses K17 but not K10, whereas steatocystoma expresses K17 and K10.31 Interestingly, mutations in the KRT17 gene can cause both pachyonychia congenital type 2 and also a condition very similar or identical to steatocystoma multiplex.32,33 The relevance of these findings to steatocystoma simplex and vellus hair cysts, if any, remains to be determined.
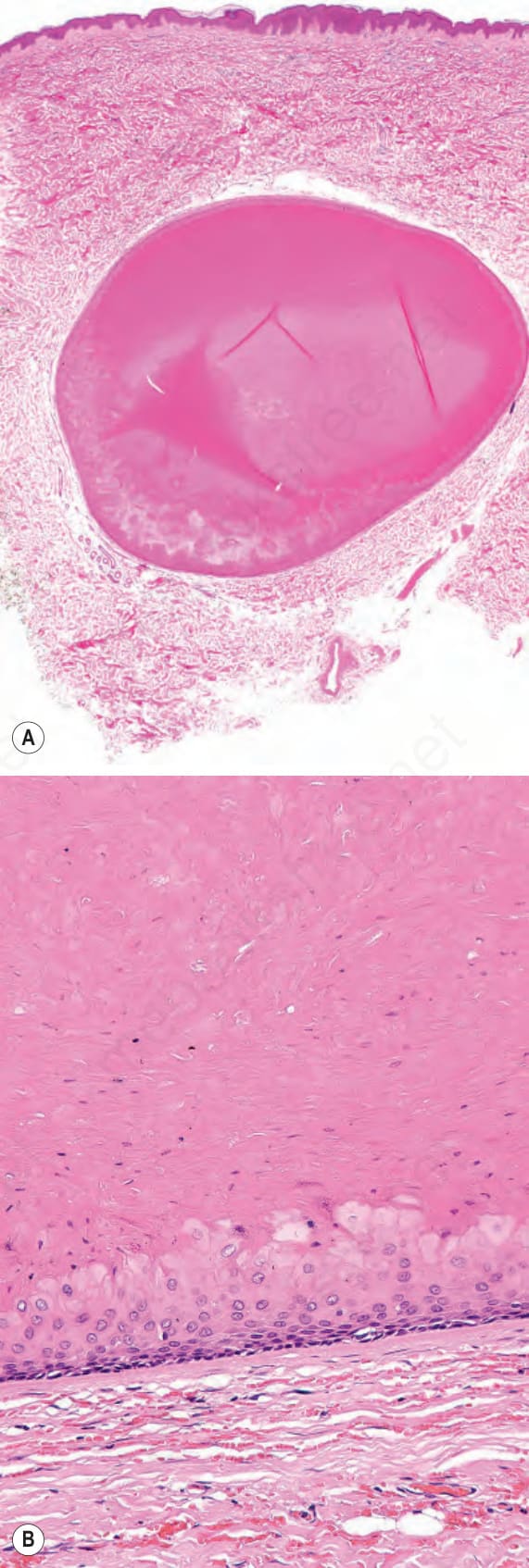
Fig. 34.21 (A, B) Trichilemmal cyst: these views show the homogeneous eosinophilic contents. Note the distinct basal cell layer.
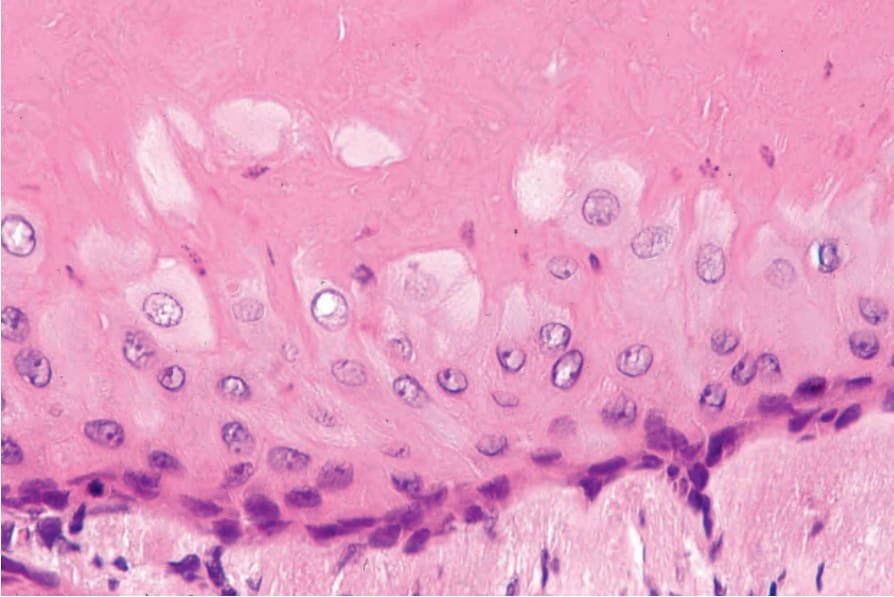
Fig. 34.22 Trichilemmal cyst: the cyst wall is composed of squamous epithelium and a granular cell layer is not present. The most superficial cells are larger, vertically orientated, and have abundant cytoplasm. Keratinization is abrupt.
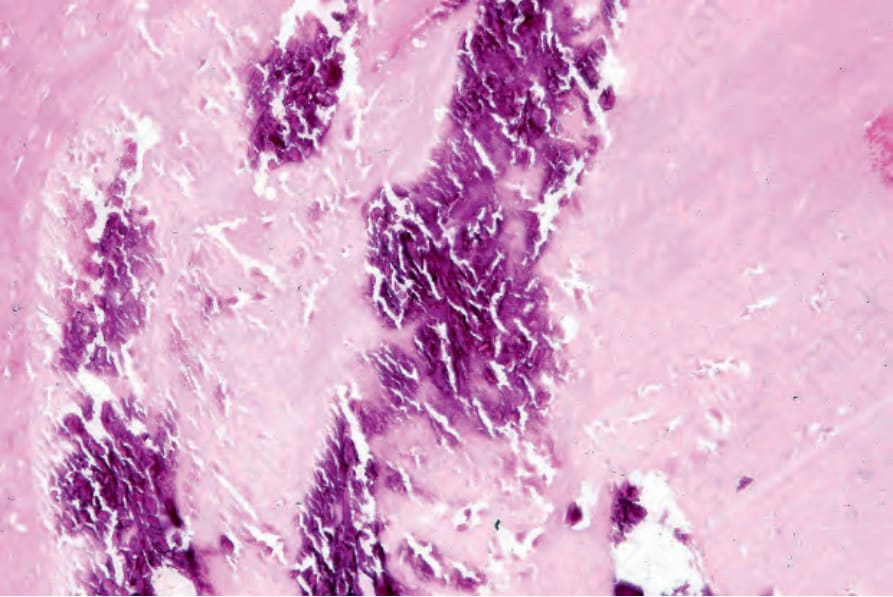
Fig. 34.23 Trichilemmal cyst: basophilic granular calcification is a frequent histologic finding.
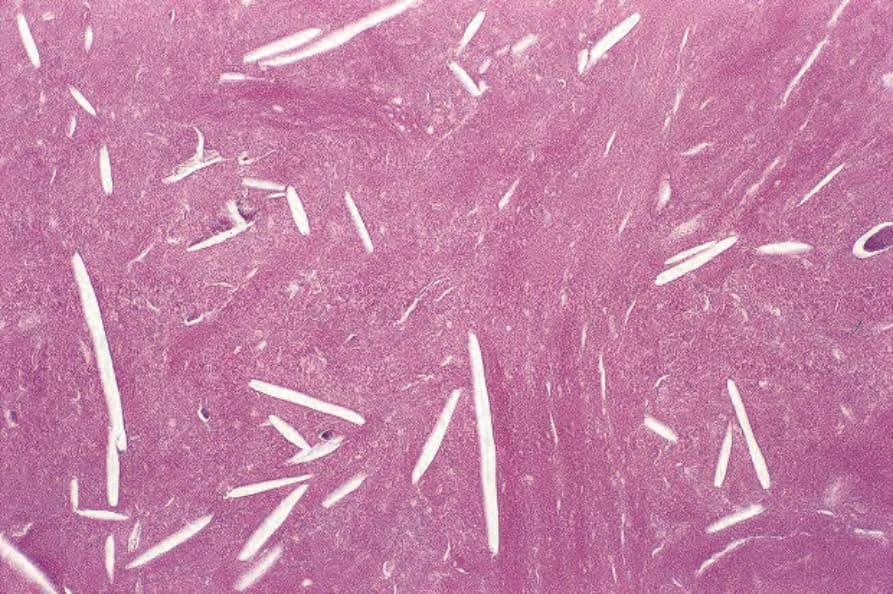
Fig. 34.24 Trichilemmal cyst: the empty spaces (cholesterol clefts) are a common feature of this lesion.
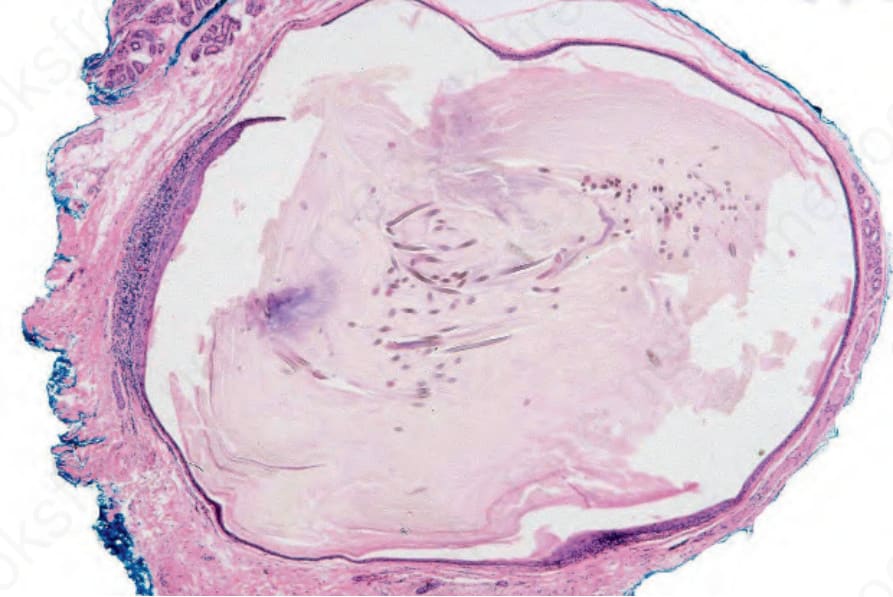
Fig. 34.25 Vellus hair cyst: this thin-walled cyst is present in the mid-dermis.
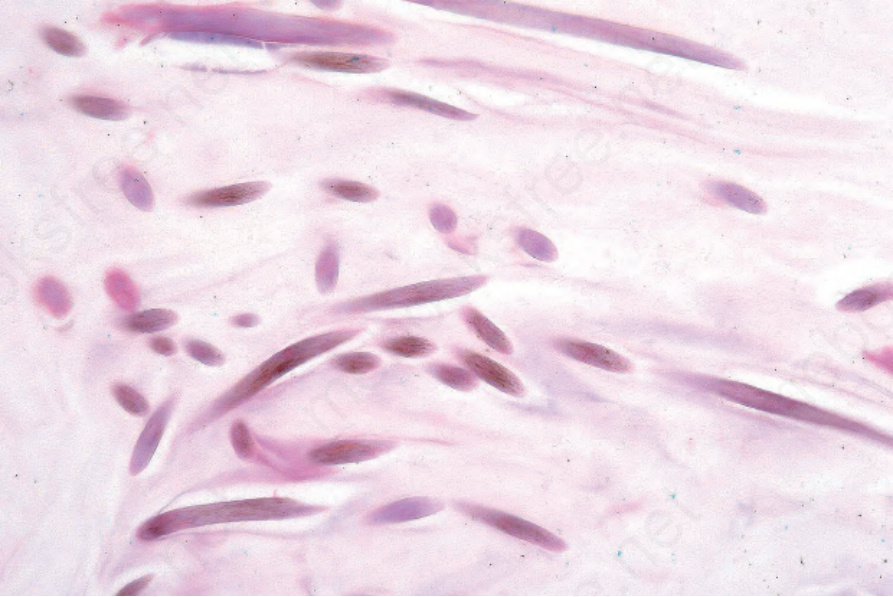
Fig. 34.26 Vellus hair cyst: on high power, the lumen contains numerous vellus hairs.