Milia
Milia
Clinical features Milia are common superficial keratinous cysts that present as white or yellow dome-shaped nodules measuring 1–3 mm in diameter.1,2 They may
Secondary milia may complicate a wide range of conditions including follicular mucinosis, folliculotropic mycosis fungoides, lichen sclerosus, radiotherapy, herpes zoster infection, leishmaniasis, severe burns, dermabrasion, chemical peeling, cutaneous local steroid therapy, adverse drug reactions (e.g., benoxaprofen), contact dermatitis, tattoos, and in a case of generalized granuloma annulare with a photosensitive distribution.3,5–17 Rarely, an association with bullae in systemic AL amyloidosis has been reported.18 Multiple follicular cysts and milia resulting in cutis verticis gyrate have been described after brain radiotherapy during vemurafenib therapy for melanoma.19 Lesions have also been described on the face and trunk during treatment with vemurafenib.20 Milia are also a feature of a number of subepidermal blistering disorders including dystrophic
1686 Cutaneous cysts
Transverse nasal crease is a rare embryologic anomaly that presents at the junction of the middle and lower third of the nose.29 The clinical presentation varies from a subtle erythematous line to a hypopigmented indentation. It has been suggested that what has been described as transverse nasal milia represents a clinical variant of transverse nasal crease.29
epidermolysis bullosa, epidermolysis bullosa acquisita, porphyria cutanea tarda, pseudoporphyria, and bullous pemphigoid.21 Milia may exceptionally occur in dominant dystrophic epidermolysis bullosa at sites of intact skin and not in association with scarring, suggesting that it may represent a primary manifestation of the disease.22 They may also be a feature of a variety of familial dermatoses including Rombo syndrome (facial anetoderma vermiculatum, telangiectasia, milia, hypotrichosis, acral erythema, cyanosis, and tendency to develop trichoepitheliomas and basal cell carcinomata), Bazex-Dupré-Christol syndrome (follicular atrophoderma, congenital hypotrichosis, basal cell carcinomas), familial multiple cylindromas, trichoepitheliomas, milia and spiradenomas (Brooke-Spiegler syndrome), Basan syndrome (diffuse congenital milia, transient neonatal acral bullae, and absence of dermatoglyphics), oral-facial-digital syndrome type 1, atrichia with papular lesions, hereditary vitamin D-dependent rickets type II, basal cell nevus syndrome, generalized basaloid follicular hamartoma syndrome, Nicolas-Balus syndrome (eruptive syringomas, milia, and atrophoderma vermiculata), KID syndrome, and hypotrichosis with light-colored hair and facial milia, and pachyonychia congenital type II.23–26 Generalized congenital milia cysts have also been described in an infant with trisomy 13 syndrome.27 Congenital familial milia with no other associations may also be rarely seen.28
Rarely, milia present as a localized plaque variant (milia en plaque).3,30–36 Such lesions are most often described around the ears. A small number of cases involving the eyelids have been documented, and there is one supraclavicular example.31 One case that developed in a background of pseudoxanthoma elasticum has been described.32 A further example in association with lupus erythematosus and another one in association with cryotherapy have also been reported.37,38 In the small number of documented cases, the sex incidence is equal, and a wide age range has been affected (12–62 years). A congenital case has been described.39 Bilateral lesions are exceptional.40,41 There is no racial predilection.33 Patients present with an edematous, erythematous plaque studded with numerous milia. Based on a single case with trichoepithelioma-like changes in the background, it has been suggested that this entity represents a variant of follicular hamartoma.42
Very occasional examples of eruptive milia have been described including rare cases in children.4,43–45 Recently, these have been classified into spontaneous and autosomal dominant familial variants.46 They may also represent a component of a genodermatosis.4
Pathogenesis and histologic features Milia consist of miniature epidermoid cysts located in the superficial dermis just underneath the epithelium (Fig. 34.17). Attachment to a vellus hair follicle is often seen in the newborn variant. Secondary lesions may be related to hair follicles or eccrine sweat ducts. The latter are typically seen in milia associated with scarring blistering diseases. Primary lesions may also be associated with the eccrine duct.47 Milia cysts occurring on palms and soles are likely derived from eccrine sweat ducts.48
The etiology of milia en plaque is unknown, although spectacles, earrings, and perfume have been suggested as possible causes.33–35 In this variant, a background dense T-cell lymphocytic infiltrate is typically present.33,34
1687 Follicular cysts
a finger have been reported.5 Proposed criteria for the diagnosis of hereditary trichilemmal cysts include: (1) lesions in at least two first-degree relatives or on three first- or second-degree relatives in two consecutive generations. (2) At least one of the affected persons diagnosed before the age of 45. (3) The presence of multiple or giant (> 5 cm) or unusual histologic features including proliferating cysts or ossification.6 A case of two female siblings presenting with multiple calcified trichilemmal cysts and alopecia universalis has been described.7 They present as smooth, yellowish, dome-shaped intradermal swellings and are more common in females (Fig. 34.19). In contrast to epidermoid cysts, they are characteristically devoid of a punctum. It should be noted that the term ‘sebaceous cyst’ favored by many clinicians is a misnomer because such lesions represent either epidermoid or trichilemmal cysts. Typically, the cyst is encapsulated and uncomplicated lesions readily ‘shell out’ at surgery.4 Acute inflammation is uncommon, and when it does occur it is usually of nonbacterial origin; its presence makes excision more difficult, with an increased likelihood of rupture. Exceptional cases of a lesion presenting with filiform hyperkeratosis, comedo-like lesions, and multiple trichilemmal cysts following Blaschko lines, have been described as trichilemmal cyst nevus (nevus trichilemmocysticus) and regarded as a complex organoid epidermal nevus.8,9 A case of multiple giant trichilemmal cysts, one of which displayed transformation to a squamous cell carcinoma, has been reported.10 Some lesions may be associated with the development of proliferating trichilemmal tumors (see Chapter 31).11
Histologic features The cyst is surrounded by a fibrous capsule against which rests a layer(s) of small dark-staining basal cells. These merge with characteristic squamous epithelium composed of pale keratinocytes, which increase in height as they mature and transform abruptly into solid eosinophilic-staining keratin without forming a granular cell layer (Figs 34.20–34.22). Occasionally, small foci of epidermal keratinization (i.e., with a granular cell layer) may also be identified. Calcification occurs in 25% of lesions, regardless of the age or size of the cyst, and cholesterol clefts occur in up to 90% (Figs 34.23 and 34.24).1,4 Osseous metaplasia may occur and exceptionally, extramedullary hematopoiesis has been described.12,13 Secondary inflammation is manifest as an influx of inflammatory cells into the lumen of the cyst, in contrast to the granulomatous response that may surround an epidermoid cyst. In a small percentage of cases, there is budding of tiny daughter cysts from the parent.14 Very rarely, sebaceous and apocrine differentiation are found in the cyst wall.15 Exceptional cases of other neoplasms such as Merkel cell carcinoma colonizing or arising in a trichilemmal cyst have been reported.16,17 Carcinoma in situ and squamous cell carcinoma may also rarely develop within trichilemmal cysts.10,18
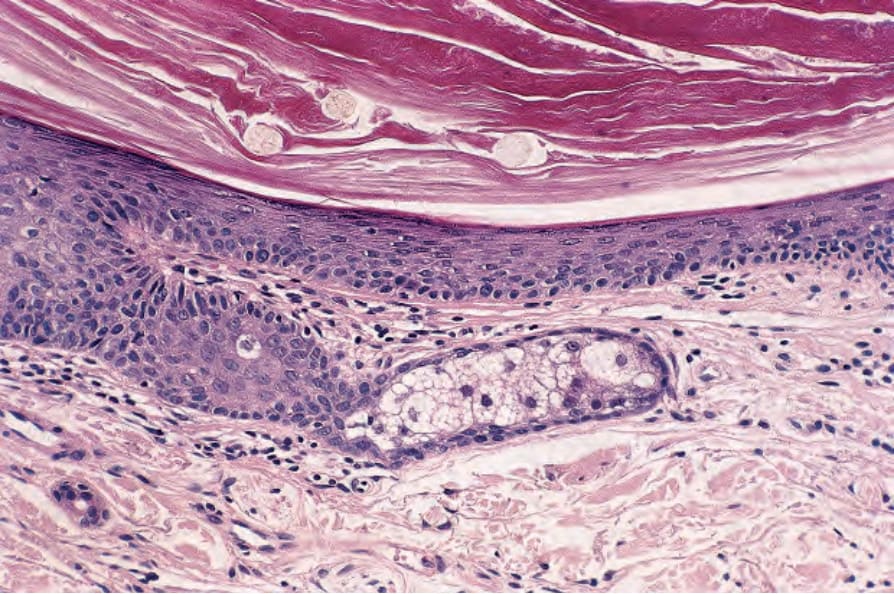
Fig. 34.14 Open comedone: the wall is composed of squamous epithelium. In addition to keratin, there are three pale-staining vellus hairs. Note the atrophic sebaceous gland.
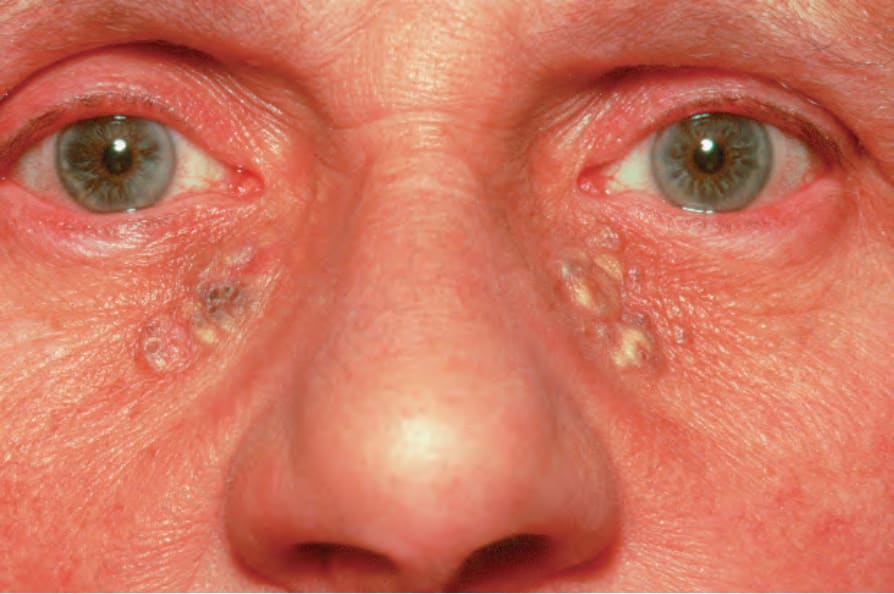
Fig. 34.15 Solar comedones: note the presence of blackheads and multiple yellow cysts.

Fig. 34.16 Milia: numerous typical pale small spherical lesions are present. The cheek is a characteristic site. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
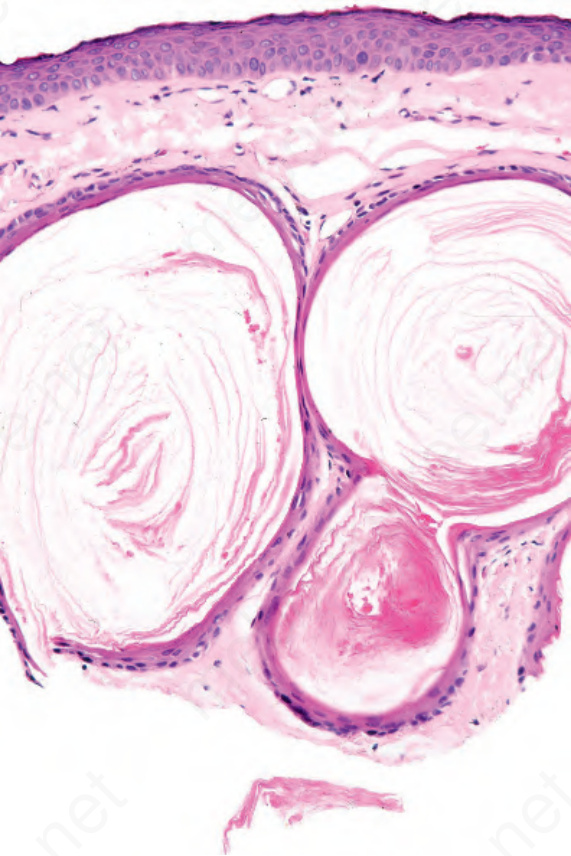
Fig. 34.17 Milia: the cysts are lined by keratinizing stratified squamous epithelium. A granular cell layer is present.
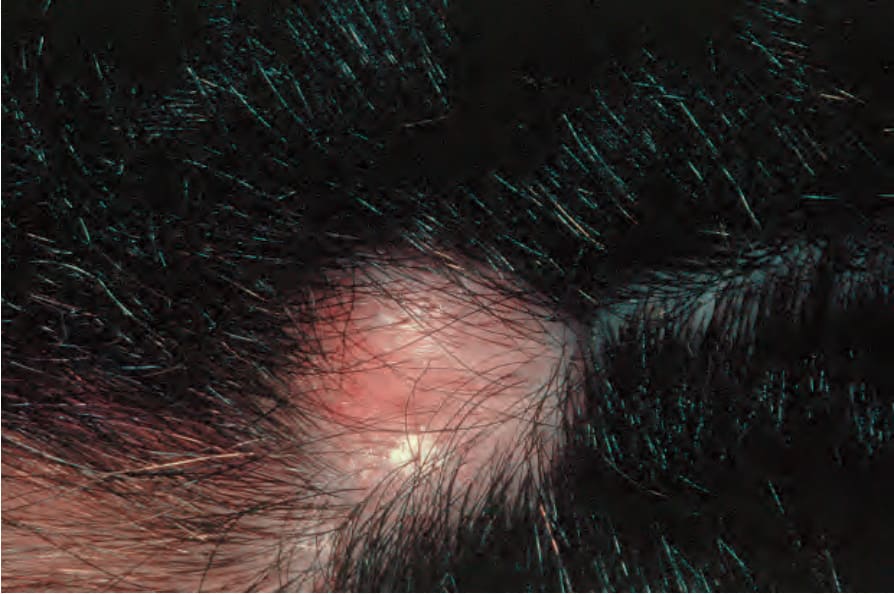
Fig. 34.18 Trichilemmal cyst: note the characteristic dome-shaped swelling on the scalp, a typical site. By courtesy of A. du Vivier, MD, King’s College Hospital, London, UK.

Fig. 34.19 Trichilemmal cyst: there are yellowish circumscribed nodules on the upper eyelids. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 34.20 Trichilemmal cyst: this shows the typical macroscopic appearance of cheesy lamellated contents.
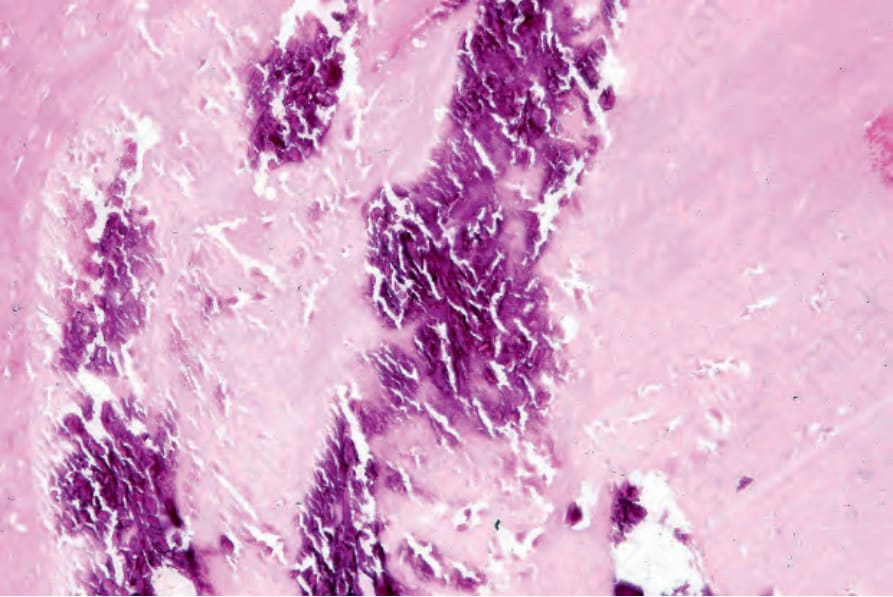
Fig. 34.23 Trichilemmal cyst: basophilic granular calcification is a frequent histologic finding.