Verrucous cyst
Verrucous cyst
Clinical features The verrucous cyst is a variant of epidermoid cyst associated with HPV infection.1–5 Adults are affected, and lesions may present at a wide variety of sites although the face, back, and (to a lesser extent) the arms and chest are most often involved.5 The sexes are affected equally. The cysts show no particular distinguishing clinical features.4
Pathogenesis and histologic features Verrucous cysts are associated with HPV infection as determined by polymerase chain reaction.3,4 Thus far, HPV antigens have not been identified with immunohistochemistry. The subtype is unknown in most cases, but a single lesion with the HPV type 59 has been described.6 HPV16 was demonstrated in a case of invasive squamous cell carcinoma arising from a verrucous cyst.7 An unusual case of multiple verrucous cysts associated with epidermodysplasia verruciformis-associated HPVs (20, 24, alb-7, and 80) and epidermodysplasia verruciformis-like epidermal lesions in the setting of idiopathic CD4 lymphopenia (immunosuppression) has been described.8
Pathogenesis and histologic features Follicular dilatation and hyperkeratosis (follicular plugging) are common features of facial skin. The development of an acne microcomedone is a further extension of that process. The fully developed blackhead contains abundant laminated keratin and cellular debris (Fig. 34.13). A large sebaceous gland with a small hair may be attached to the widely distended but patent follicle. If the lesion persists, the sebaceous gland and hair commonly atrophy (Fig. 34.14). A histologic section through a closed comedone will often miss the blocked connection with the epidermis, and sometimes a blackhead may appear as an intradermal cyst.
Histologically, verrucous cyst shows focal features of a typical epidermoid cyst and rarely features of a trichilemmal cyst.9 The greater part of the cyst wall, however, is lined by papillomatous, acanthotic squamous epithelium with hyperkeratosis, parakeratosis, and conspicuous hypergranulosis. Keratohyaline granules are enlarged and irregular, and occasionally koilocytes are seen.2,3,5 In some lesions, the epithelium consists of an admixture of basaloid and squamous cells, and squamous eddies are prominent.3 A lymphohistiocytic infiltrate is sometimes present in the surrounding dermis.
Differential diagnosis Solar comedones (Favre-Racouchot disease) occur as a clinical triad of cysts, comedones, and elastosis around the orbit and malar areas of elderly patients, and are due to prolonged exposure to sunlight (Fig. 34.15) or very rarely secondary to radiotherapy.2,3 Rarely, a plaquelike lesion may be seen.4 Squamous cell carcinoma may rarely develop within a lesion.5 Large thin-walled open and closed comedones are present in the upper dermis, accompanied by marked solar elastosis.6 A small series of cases of what is regarded as a variant of Favre-Racouchot disease and including epidermoid cysts with vellus hairs and solar elastosis and presenting on the ears has been described.7
Open and closed comedones are also a feature of the congenital conditions familial comedones and familial dyskeratotic comedones. Both of these have an autosomal dominant mode of inheritance; the former is characterized by a greater number of lesions and an absence of dyskeratosis.8–10.
1685 Follicular cysts
A
represent primary lesions when no cause can be identified or secondary variants usually following skin trauma or other injury.
Primary milia are seen in up to 50% of newborns and present on the face, upper trunk, and extremities.3 These typically regress spontaneously. Children and adults can also be affected, when lesions are most often apparent on the face (forehead, eyelids, and cheeks) and the external genitalia (Fig. 34.16).3 Possible association of persistent infantile milia with steatocystoma multiplex and eruptive vellus hair cysts has also been suggested.4
B
Rarely, late-stage follicular mucinosis and discoid lupus erythematosus may feature large thin-walled comedones as the dominant histologic component.

Fig. 34.11 Acne vulgaris: (A) typical open comedones (blackheads); (B) close-up view. (A) By courtesy of R.A. Marsden, St George’s Hospital, London, UK; (B) by courtesy of the Institute of Dermatology, London, UK.

Fig. 34.12 Acne: numerous closed comedones (whiteheads) are present on this patient’s cheek and chin. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
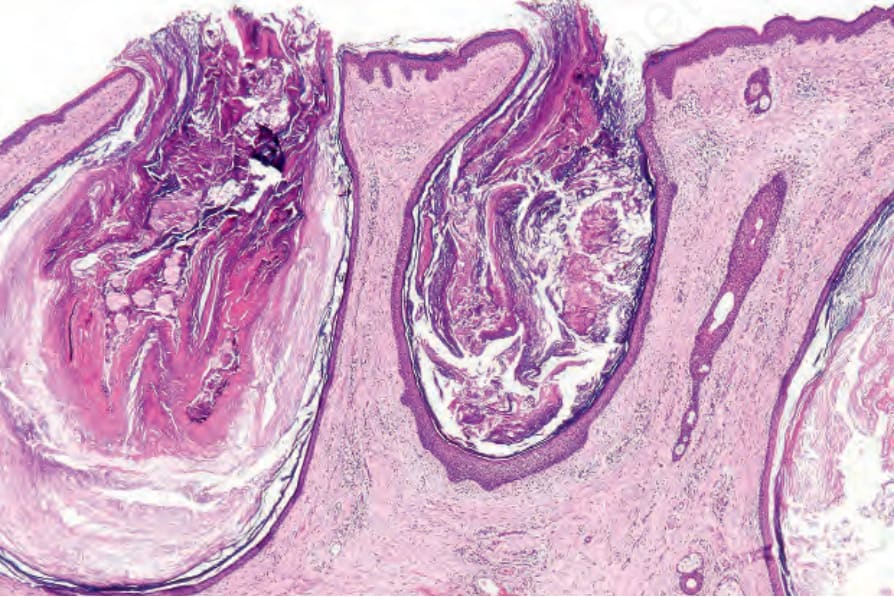
Fig. 34.13 Open comedone: the lesion consists of a cystically dilated hair follicle containing abundant keratin.
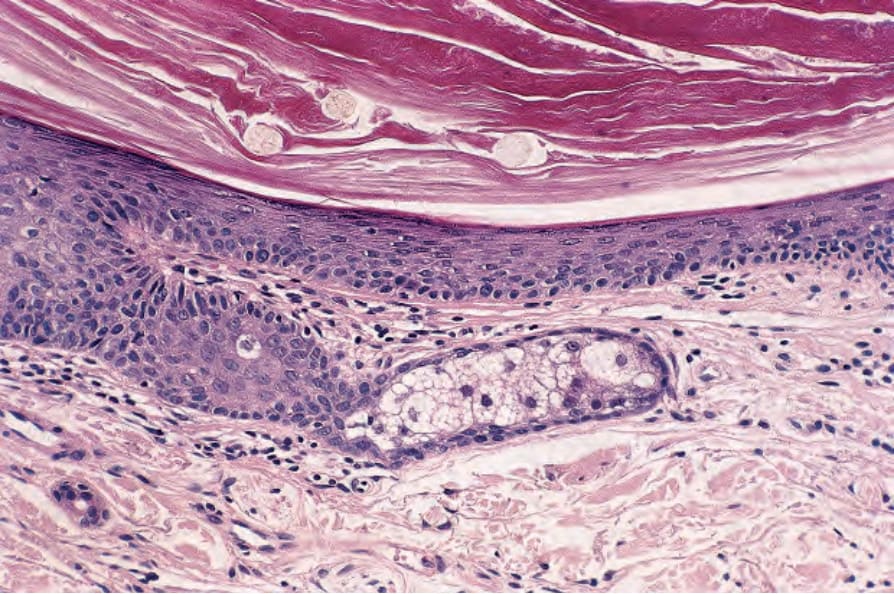
Fig. 34.14 Open comedone: the wall is composed of squamous epithelium. In addition to keratin, there are three pale-staining vellus hairs. Note the atrophic sebaceous gland.
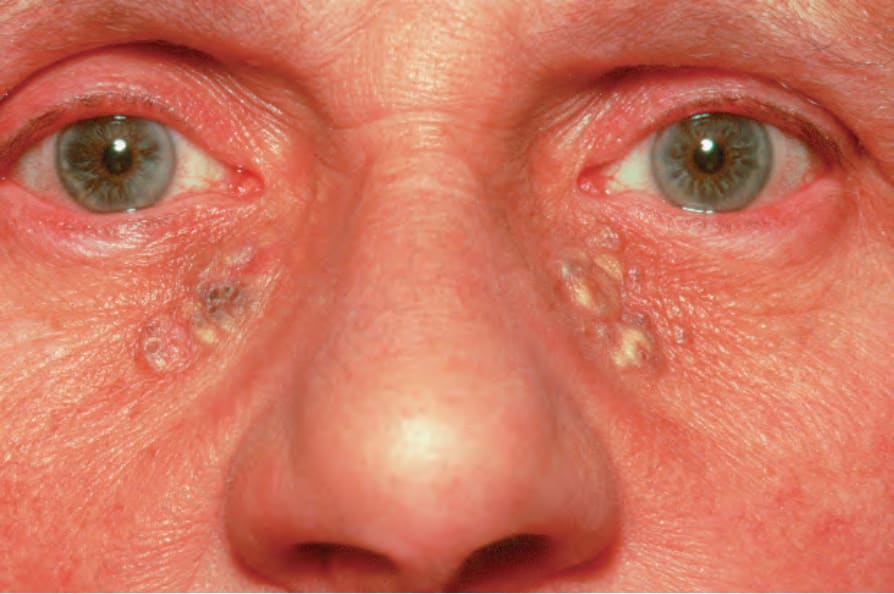
Fig. 34.15 Solar comedones: note the presence of blackheads and multiple yellow cysts.

Fig. 34.16 Milia: numerous typical pale small spherical lesions are present. The cheek is a characteristic site. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.