Epidermoid cyst
Epidermoid cyst
Clinical features Epidermoid (epidermal, infundibular) cysts, which occur particularly on the face, neck, and upper trunk, are believed to result from damage to the pilosebaceous units.1 The vulval labia majora and scrotum are also sites of predilection. Rare lesions develop in non-hair-bearing areas like the soles (see below).2 Young and middle-aged adults are most often affected, and the sexes are involved equally. Epidermoid cysts present as smooth dome-shaped swellings a few millimeters to a few centimeters across (Fig. 34.1). A punctum is usually present (Fig. 34.2).
Pathogenesis and histologic features Lesions develop as a result of obstruction of the upper part of the hair follicle or secondary to trauma (inclusion cysts).
Epidermoid cysts are unilocular, spherical, and are lined by an epidermis-like epithelium including a granular cell layer (Figs 34.4–34.6).1 Exceptional multilocular lesions may occur.20 The cyst contents of laminated keratin are believed to represent follicular infundibular derivation (the nonimplantation variant). In older lesions, the lining is often somewhat attenuated. Lichenoid inflammation of the wall indistinguishable from lichen planus may be seen. Acute inflammation may result in the subsequent disruption of the cyst wall, with the development of an intense foreign body giant cell reaction (Fig. 34.7). Sometimes this may be so marked that it completely destroys the cyst, and only focal dermal collections of keratin fragments remain (Fig. 34.8). It is not clear whether bacteria play an important role in the development of inflammation in epidermoid cysts. A study from Japan found an increased incidence of anaerobes in inflamed lesions as opposed to those without inflammation.21 It remains to be established, however, whether this is the result of colonization or a true infection. Occasionally, the cyst lining may show epidermoid and focal trichilemmal keratinization. In the rare hybrid cyst, there is epidermoid keratinization in the
The presence of multiple lesions may suggest the possibility of Gardner syndrome, which includes polyposis coli, jaw osteomas, and intestinal fibromatoses in addition to cutaneous cysts.3,4 Less frequently, patients may manifest lipomas, pilomatrixomas (including epidermoid cysts with pilomatrical lining), and leiomyomas. Multiple lesions also occur in Gorlin-Goltz syndrome (see Chapter 24) and may be the first manifestation of the disease.5 Subconjunctival epidermoid cysts appear to occur exclusively in patients with this syndrome.6
Multiple and often large epidermoid cysts are sometimes seen as a complication of ciclosporin therapy in transplantation recipients.7,8 Multiple
1681 Follicular cysts
Keratinizing Glandular
Epidermoid Bronchogenic
Proliferating epidermoid Thyroglossal duct
Hybrid cyst Branchial
Verrucous Cervical thymic
Epidermoid cyst of the sole Ciliated
Comedonal Median raphe
Milia
Trichilemmal
Vellus hair
Steatocystoma
Dermoid
superficial half of the cyst and trichilemmal in the lower.22 Exceptionally, a pigmented variant containing multiple terminal hair shaft fragments may be encountered (pigmented follicular cyst).23,24 A case with numerous keratin spherules has been reported.25
In patients with Gardner syndrome, the cyst lining occasionally shows focal basaloid cell proliferation with ghost cell change, as seen in pilomatrixoma (Fig. 34.9).26,27 Lesions outside this context may occur, including a case in a background of nevus sebaceous.28,29 Thus, while highly suggestive, these cannot be considered pathognomonic.
The cysts in Gorlin-Goltz syndrome are usually hybrid with features of epidermoid cyst and steatocytoma.30
A case of multiple epidermoid cysts with lesions of angiofibroma in tuberous sclerosis patients associated with obstruction/trauma has been reported.31
Epidermoid cysts not uncommonly coexist with melanocytic nevi. This is of particular importance, as the resulting increase in size of the cyst may raise clinical suspicion of melanoma.32,33 Most nevi are banal and dermal,
but cysts associated with compound nevi, congenital nevi, dysplastic nevi, blue nevi, and spindle cell nevi of Reed have also been documented.33
Malignant tumors may rarely develop within the wall of an epidermoid cyst including basal cell carcinoma, squamous cell carcinoma, and squamous cell carcinoma in situ (Fig. 34.10).34–41 There are also rare case reports describing an epidermoid cyst in association with Paget disease and cutaneous neuroendocrine carcinoma (Merkel cell carcinoma).42–44 There have been a reported case of melanoma arising in a lesion, an in situ melanoma associated with an adjacent cutaneous melanoma colonizing an epidermoid cyst, and there is a single further report of a melanoma in situ arising in a noncutaneous cerebellopontine angle epidermoid cyst.45–47 Pilomatrixoma (in the absence of Gardner syndrome) in conjunction with an epidermoid cyst has also been documented.48,49 Because epidermoid cysts with malignant change cannot be clinically reliably distinguished from their extremely common benign counterpoints, histologic examination of all such cysts is recommended.50
1682 Cutaneous cysts
A
A
B
B
1683 Follicular cysts
A
B
A
B
Epidermoid cysts showing features of a range of cutaneous dermatoses have been described.51 These include pemphigus, psoriasis, lichen planus, and Darier disease.52–54 Changes of epidermolytic hyperkeratosis and involvement by molluscum contagiosum have also been described.55,56 Human papillomavirus (HPV) associations are described below (see verrucous cyst and epidermoid cyst of the sole).

Fig. 34.1 Epidermoid cyst: a typical dome-shaped swelling with two puncta. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 34.2 Epidermoid cyst: close-up view of a punctum. By courtesy of the Institute of Dermatology, London, UK.

Fig. 34.3 Epidermoid cyst: this implantation variant is at a characteristic site. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
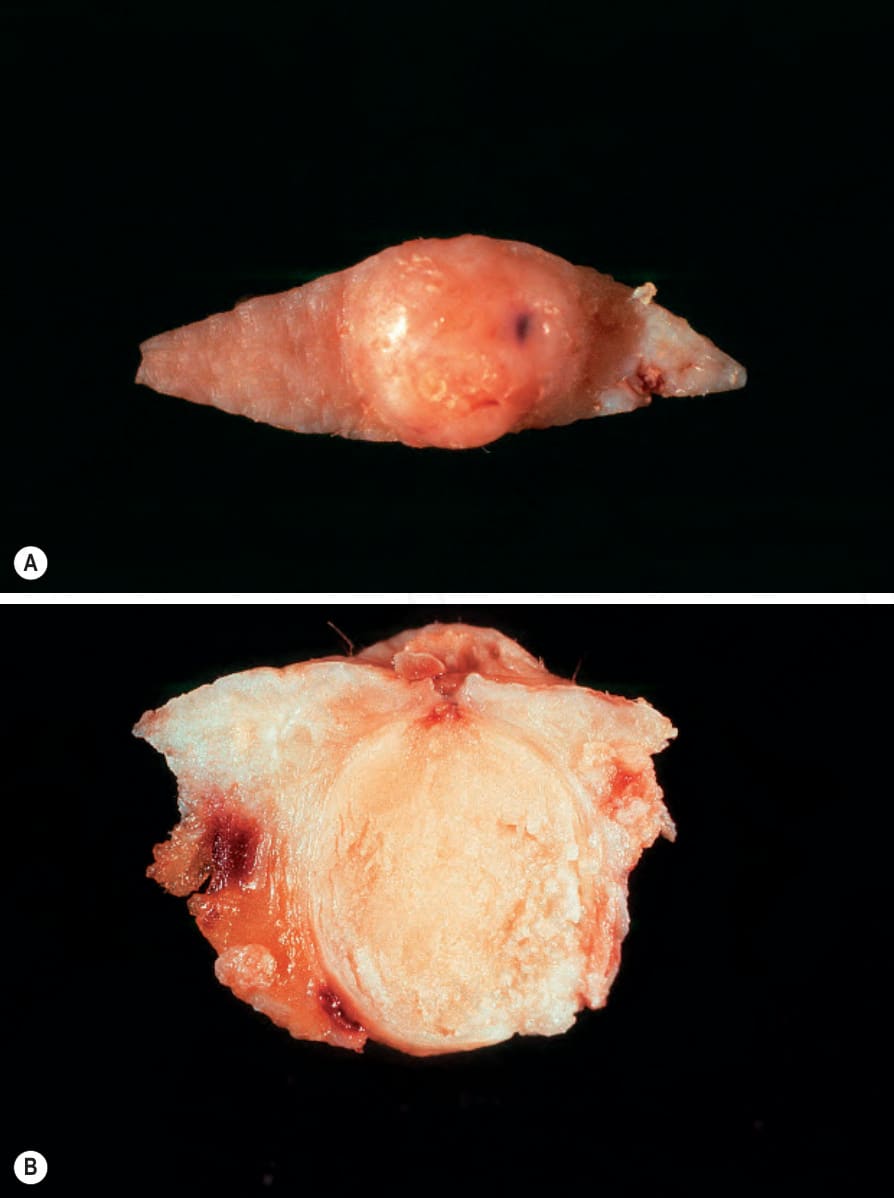
Fig. 34.4 (A, B) Epidermoid cyst: in this excision specimen, the punctum is clearly visible.
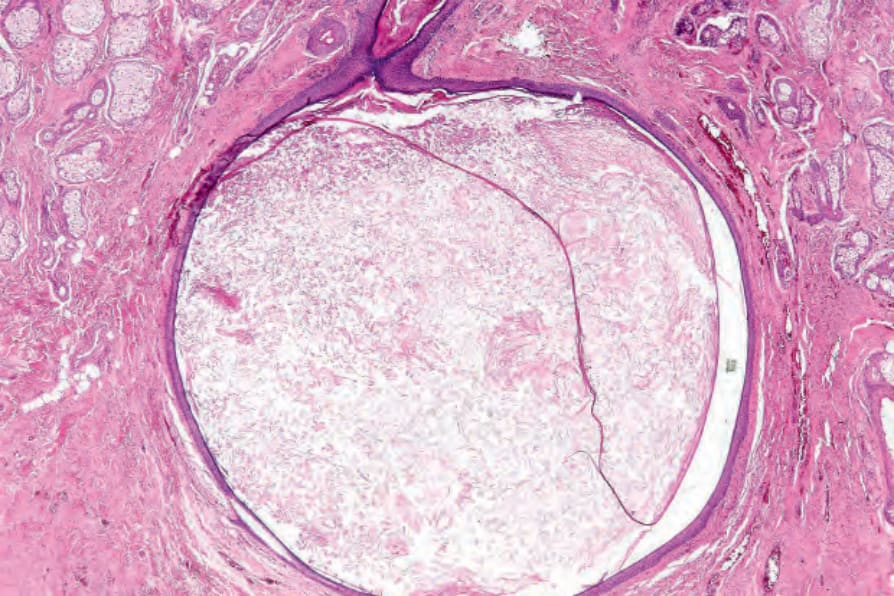
Fig. 34.5 Epidermoid cyst: a solitary lesion is present in the dermis.
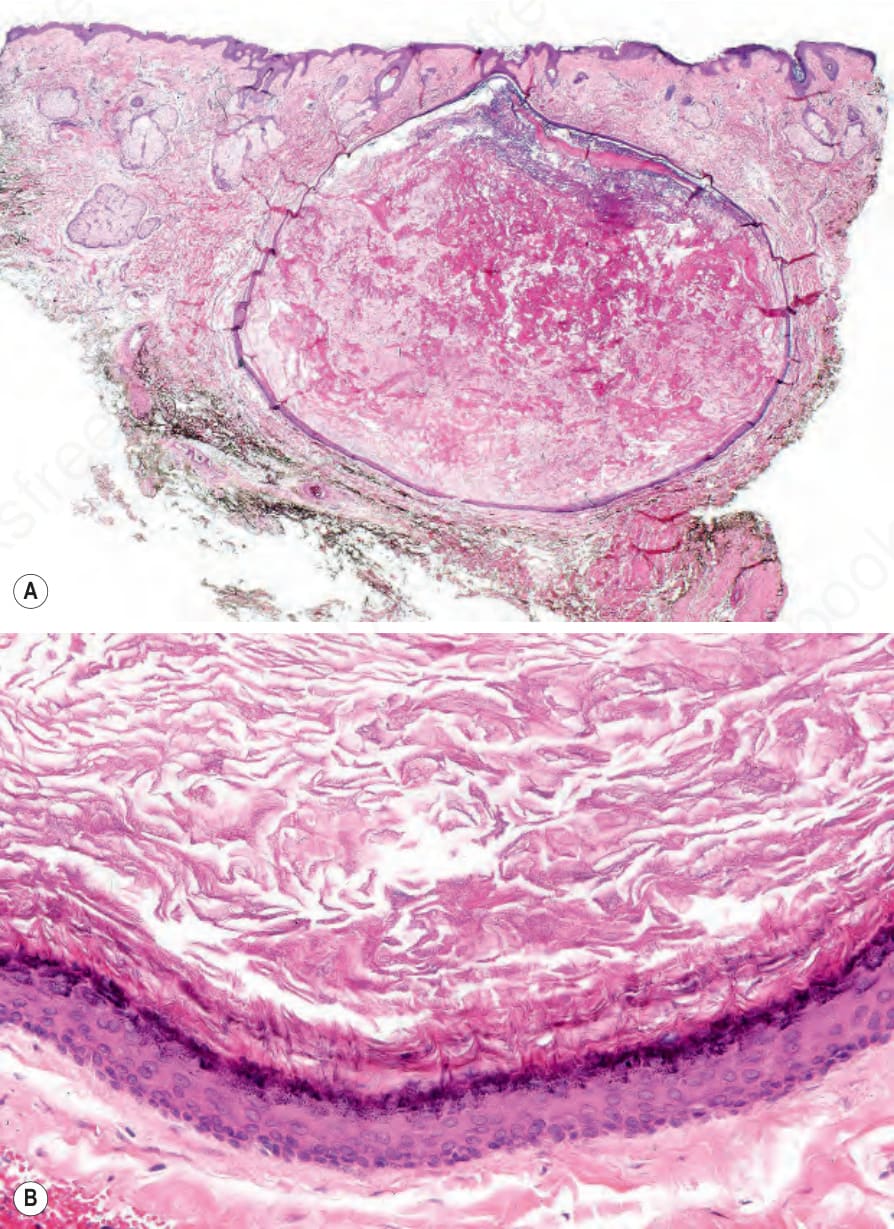
Fig. 34.6 Epidermoid cyst: (A) in this example, the punctum is present; (B) the cyst wall is composed of squamous epithelium and includes a granular cell layer. Note the laminated keratin.
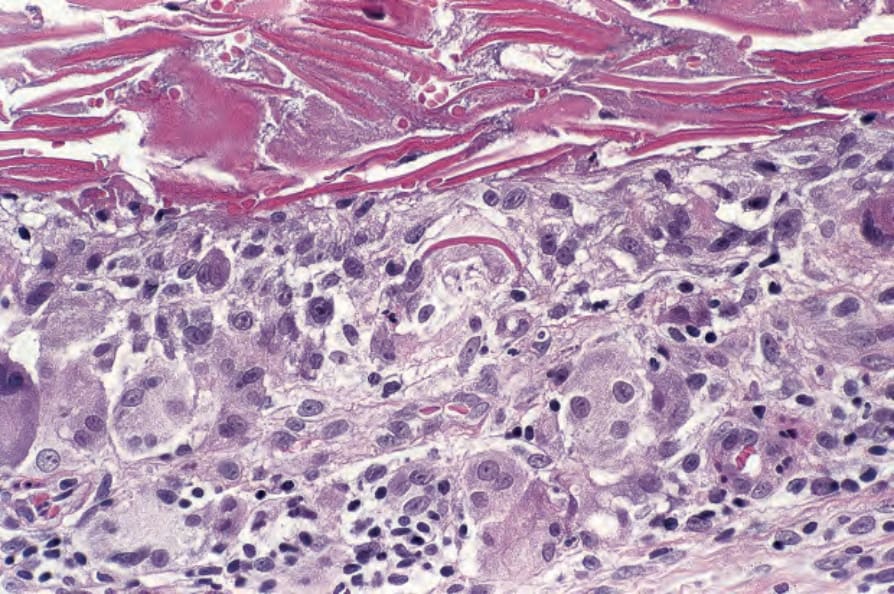
Fig. 34.7 Epidermoid cyst: rupture is associated with a foreign body granulomatous response. In the center of the field, a giant cell contains a keratin fragment.
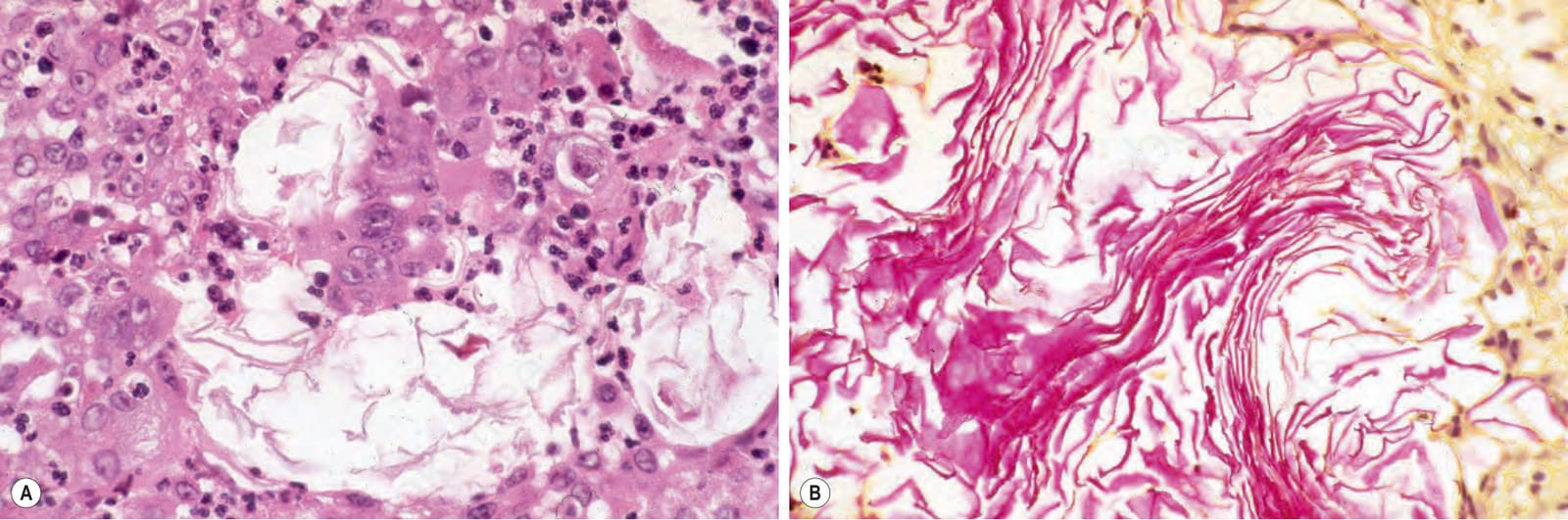
Fig. 34.8 Epidermoid cyst: (A) in this almost healed lesion, residual keratin lamellae, as seen in the center of the field, are all that is left of the ruptured cyst; (B) these may be highlighted by the Lendrum phloxine tartrazine reaction.
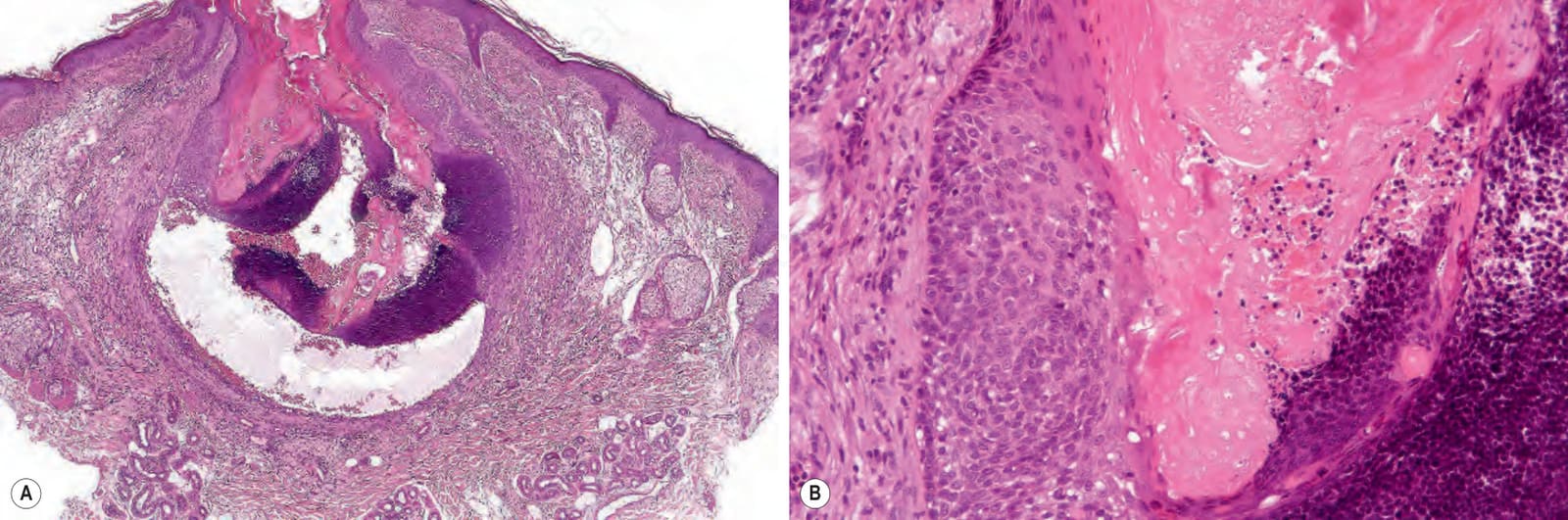
Fig. 34.9 (A, B) Epidermoid cyst: the lower half of the cyst wall shows matrical differentiation.
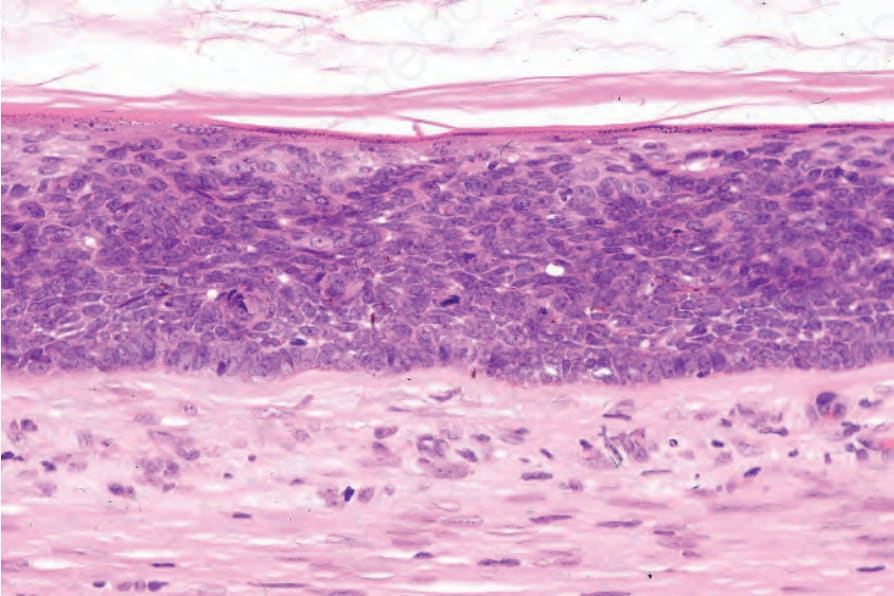
Fig. 34.10 Epidermoid cyst: in this example, the epithelial wall shows the features of carcinoma in situ.
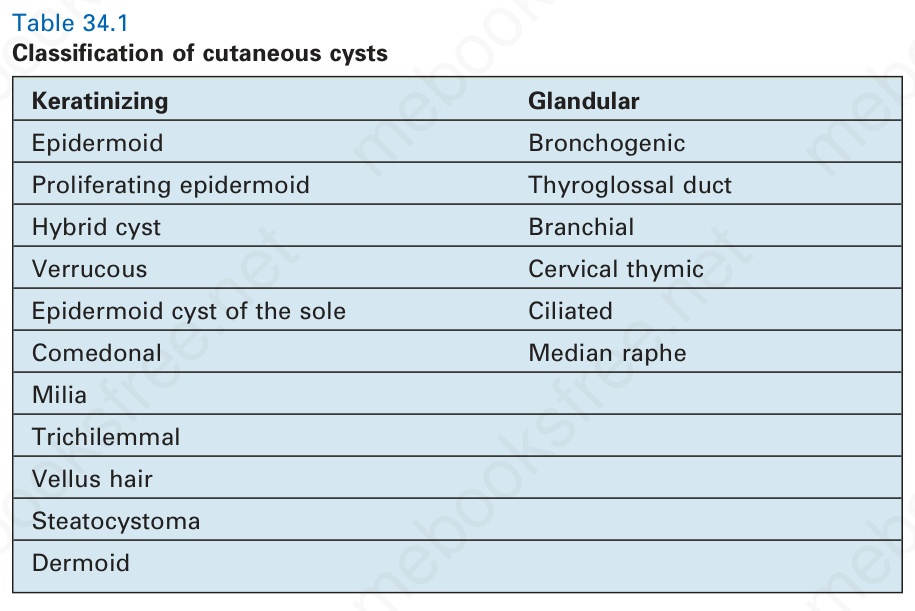
Table 34.1 Classification of cutaneous cysts