Hidradenoma
Hidradenoma
Clinical features Hidradenoma (clear cell hidradenoma, solid–cystic hidradenoma, clear cell myoepithelioma, eccrine acrospiroma), which generally occurs on the head and neck or limbs (although any site may be affected), usually presents as a solitary, slowly growing, solid, or cystic nodule (Fig. 33.130).1–6 The overlying skin may be flesh colored, erythematous, or blue.1 Lesions typically measure about 1–2 cm in diameter and present most often in middle-aged adults or the elderly (range 3–93 years), with a slight predominance in females.6 Giant variants measuring up to 12.0 cm in diameter have been documented.7,8 Exceptionally, children are affected.9–11 The tumors are sometimes symptomatic, with spontaneous oozing, hemorrhage, tenderness, pruritus, and burning.1 Recurrences are uncommon.3
Pathogenesis and histologic features The histogenesis of this tumor is uncertain. In keeping with an eccrine derivation, the tumor has been shown to contain large quantities of succinic dehydrogenase, amylophosphorylase, and leucine aminopeptidase.2 Additionally, earlier reports showed that clear cell hidradenoma did not express markers of apocrine differentiation including GCDPF-15 and GCDFP-24.12,13
1651 Hidradenoma
A
B
However, this has been contested and a small series of cases was published in which GCDPF-15 was expressed.14 On the basis of follicular continuity, decapitation secretion, mucin production, and the latter immunohistochemical finding, it has been proposed that clear cell variants are of apocrine derivation whereas only a minority of tumors composed of poroid and cuticular cells are of true eccrine derivation/differentiation (poroid hidradenoma).5,14 A reproducible chromosomal translocation t(11;19)(q21;p13) involving the CRTC1 and the MAML2 genes has been reported in salivary gland tumors such as mucoepidermoid carcinoma and Warthin tumor and has also been detected in approximately 50% of hidradenomas.15–18 This fusion appears to be particularly prevalent in tumors with clear cell features.18,19 At least a subset of the remaining tumors has been found to harbor the chromosomal translocation t(6;22) involving the EWS and the POU5F1 genes.20
The tumor is circumscribed, but unencapsulated, and is composed of lobulated, sometimes cystic masses of cells in the upper or mid-dermis (Figs 33.131 and 33.132). Some tumors are associated with follicular structures whereas others display connection to or even replace the overlying epidermis, reminiscent of eccrine poroma. On occasions, the tumor may extend into the subcutaneous fat. The tumor has a biphasic cellular population: in some areas, it is composed of round, fusiform, or polygonal cells with eosinophilic cytoplasm and a round or oval vesicular nucleus showing nuclear grooves and conspicuous nucleolus, sometimes arranged in whorls; elsewhere, it consists of cells with clear cytoplasm containing a small, dark, often eccentrically located nucleus (clear cell hidradenoma) (Figs 33.133 and 33.134).1,2,4,21,22 Transition between the two cell types is common. The
proportions and overlap of the two cell types vary within an individual tumor. Glycogen may be demonstrated in most of the tumor cells, but is in greater abundance in the clear cell areas (Fig. 33.135). The tumors are usually mitotically inactive. Tumor lobules may be intimately associated with dermal sweat glands or ducts, and occasionally the latter may be seen to be continuous with islands of tumor cells.1 As mentioned above, focal apocrine decapitation secretion can be seen. Some tumors may show squamous differentiation, squamous eddy formation, or keratinization.22,23 Mucin-rich goblet cells are an occasional finding, and rarely mucinous change is extensive (mucinous hidradenoma) (Fig. 33.136).24 Sebaceous differentiation may also be a feature.14,25–27 Exceptionally, hidradenoma has been demonstrated in continuity with mucinous syringometaplasia.28
1652 Tumors of the sweat glands
A
B
Ductlike structures are present in most tumors. These may appear as differentiated structures lined by a layer of cuboidal cells (Fig. 33.137). On other occasions, the tumor contains variably sized cystic cavities, sometimes comprising the vast bulk of the lesion (solid–cystic hidradenoma). Such cysts are lined by flattened cells and probably represent cystic degeneration. Ductal differentiation is also seen as foci of squamous cells surrounding irregular lumina complete with a diastase-resistant, PAS-positive cuticle resembling the acrosyringium (Fig. 33.138). The tumor lobules are surrounded by a definite stroma, which may be fibrovascular, collagenous, or even hyalinized (Fig. 33.139). Some tumors appear highly vascular, resulting in perivascular pseudorosettes and, occasionally, hemangiopericytoma-like areas. Occasionally, tumors may appear pigmented due to increased melanin pigment and colonization by pigmented dendritic cells.29,30 Exceptional prominent intraneural growth has been reported in a case.31 The tumor cells express AE1/AE3, EMA, and CEA.12,15 The last two are of particular value in highlighting ductal differentiation.
1653 Hidradenoma
Comment Occasionally, benign-appearing tumors show focal atypical features including nuclear pleomorphism and hyperchromatism, macronucleoli, giant cell forms, and prominent mitotic activity (two or more mitoses per 10 high-power fields) (Figs 33.140 and 33.141).32 These appearances correlate with an increased risk of recurrence and possible malignant biological potential (atypical hidradenoma).33 Wide re-excision and careful follow-up are therefore advisable for these worrisome lesions. In addition, high MIB-1 proliferative index (> 11%) and phosphorylated histone H3 of > 0.7% have been proposed to be associated with malignant rather than atypical hidradenoma.34 Conversely, lymphovascular invasion and tumor deposits in locoregional lymph nodes have recently been reported in otherwise benign-appearing hidradenomas. With long-term follow-up, no adverse outcome was observed in these patients, and the findings likely represent the so-called benign metastasis. In practice, these findings should, however, be treated with caution and the tumors be regarded as atypical hidradenomas or as hidradenomas of uncertain malignant potential.35,36
A
B
1654 Tumors of the sweat glands
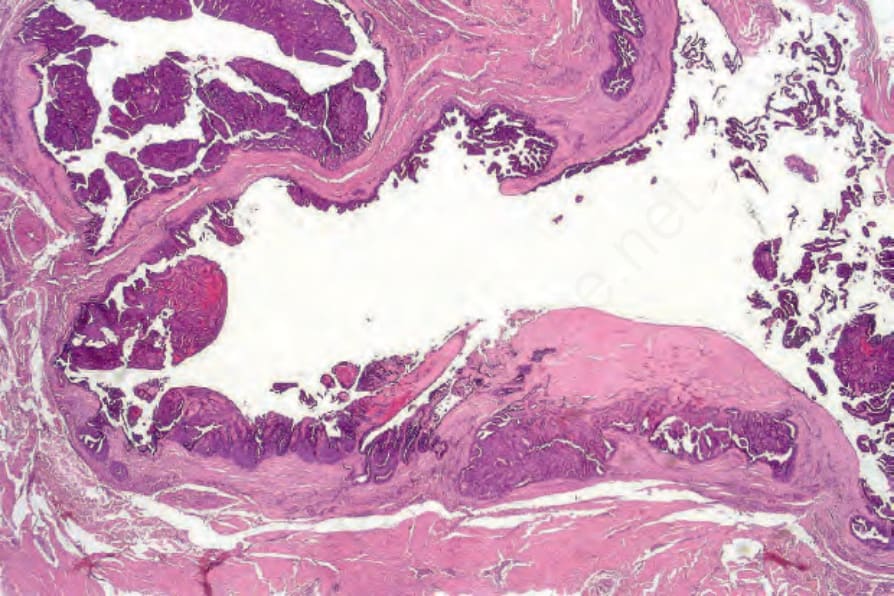
Fig. 33.127 Digital papillary adenocarcinoma: this example is partially cystic. Note the papillary processes covered by multiple layers of basophilic epithelium.
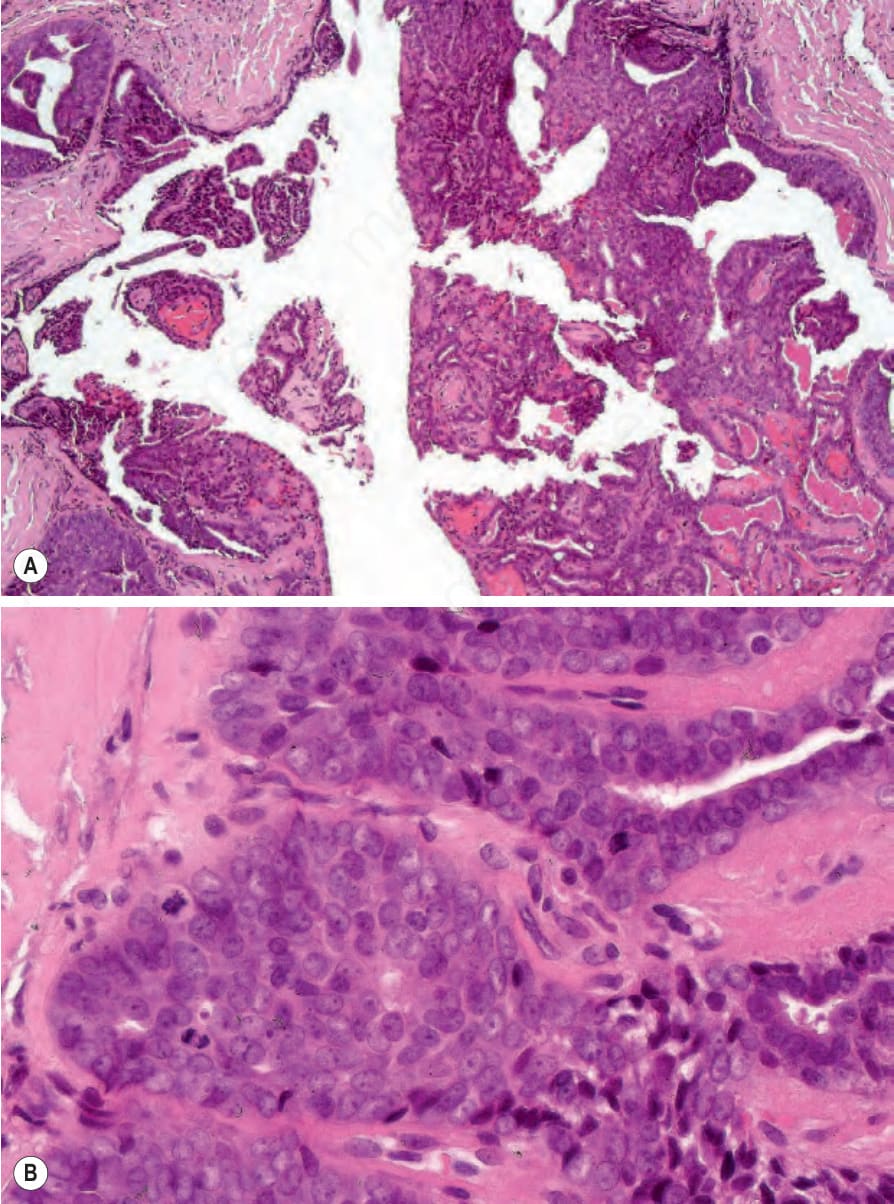
Fig. 33.129 Digital papillary adenocarcinoma: (A) medium-power view showing papillary processes; (B) there are prominent nucleoli and multiple mitoses are present.

Fig. 33.130 Eccrine hidradenoma: this lesion presents as a solitary nodule most often on the head and neck or limbs. By courtesy of the Institute of Dermatology, London, UK.
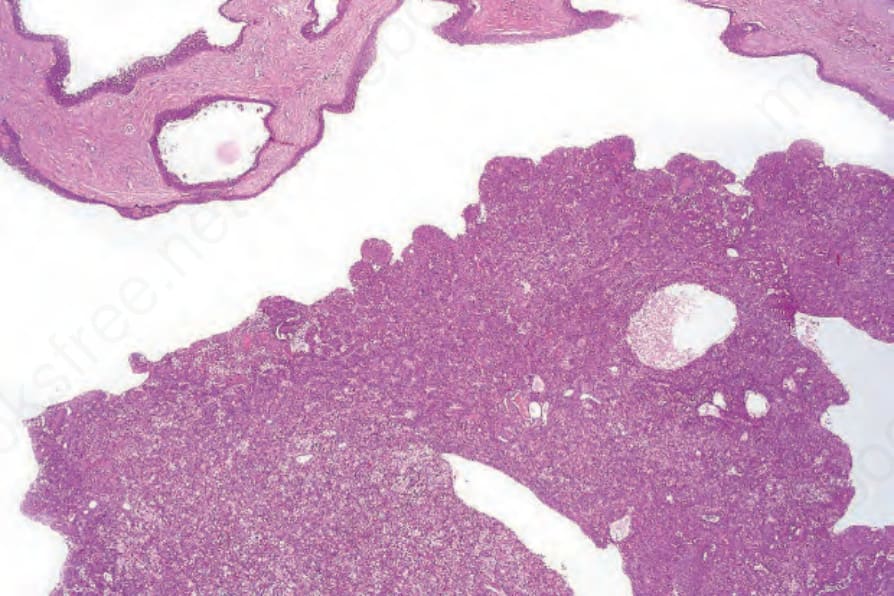
Fig. 33.131 Eccrine hidradenoma: this example shows multiple, variably sized cysts in addition to a solid component (solid-cystic hidradenoma).
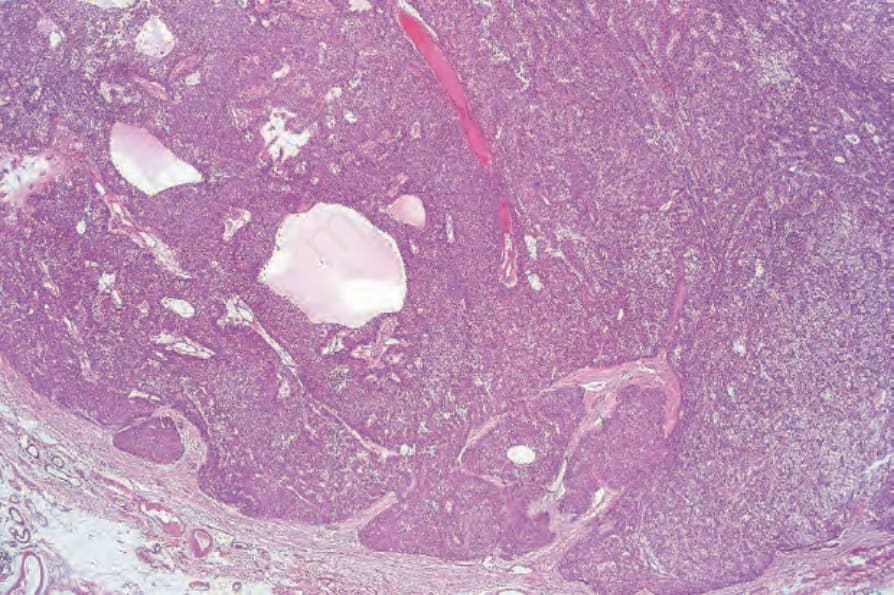
Fig. 33.132 Eccrine hidradenoma: low-power view of a circumscribed dermal tumor nodule.
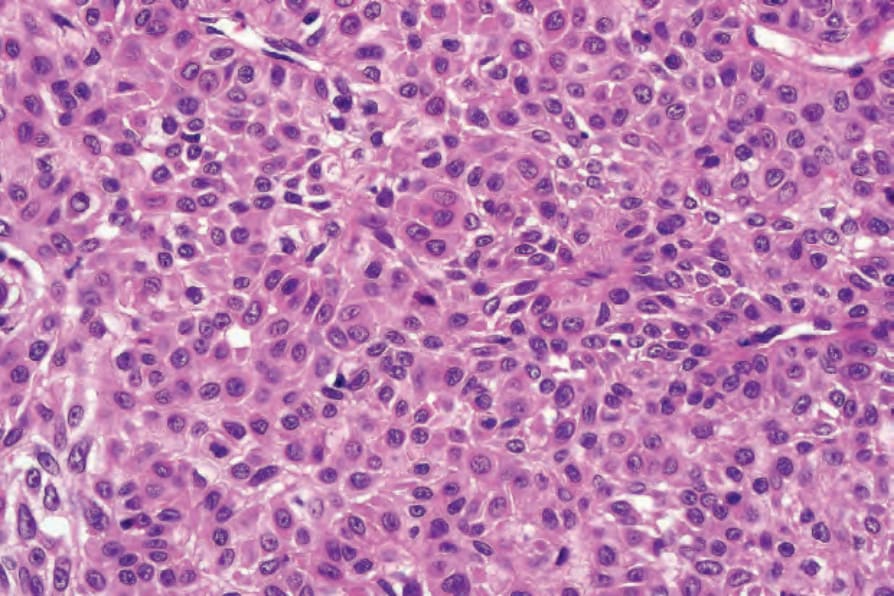
Fig. 33.133 Eccrine hidradenoma: high-power view showing uniform cells with eosinophilic cytoplasm.
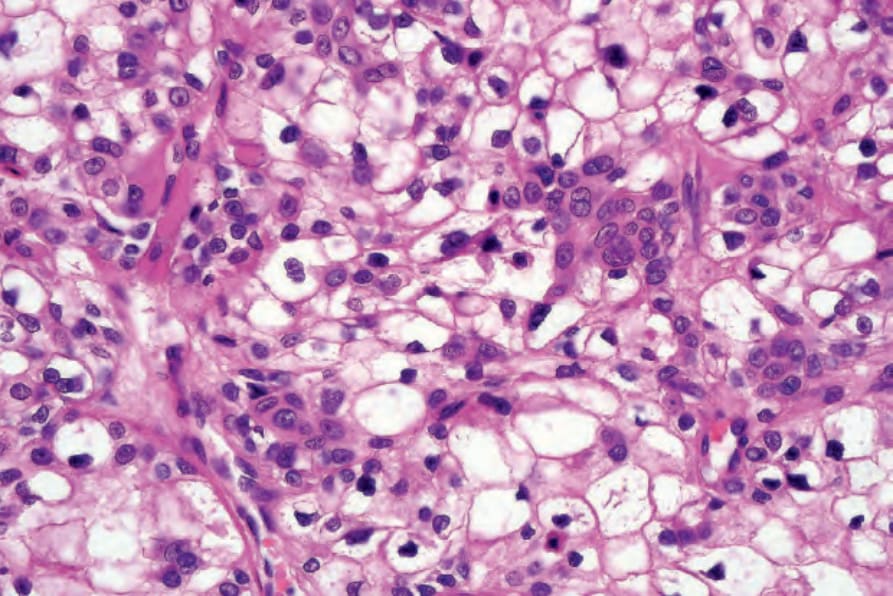
Fig. 33.134 Eccrine hidradenoma: in this field, the tumor consists of an admixture of cells with eosinophilic cytoplasm and glycogen-rich clear cell forms.
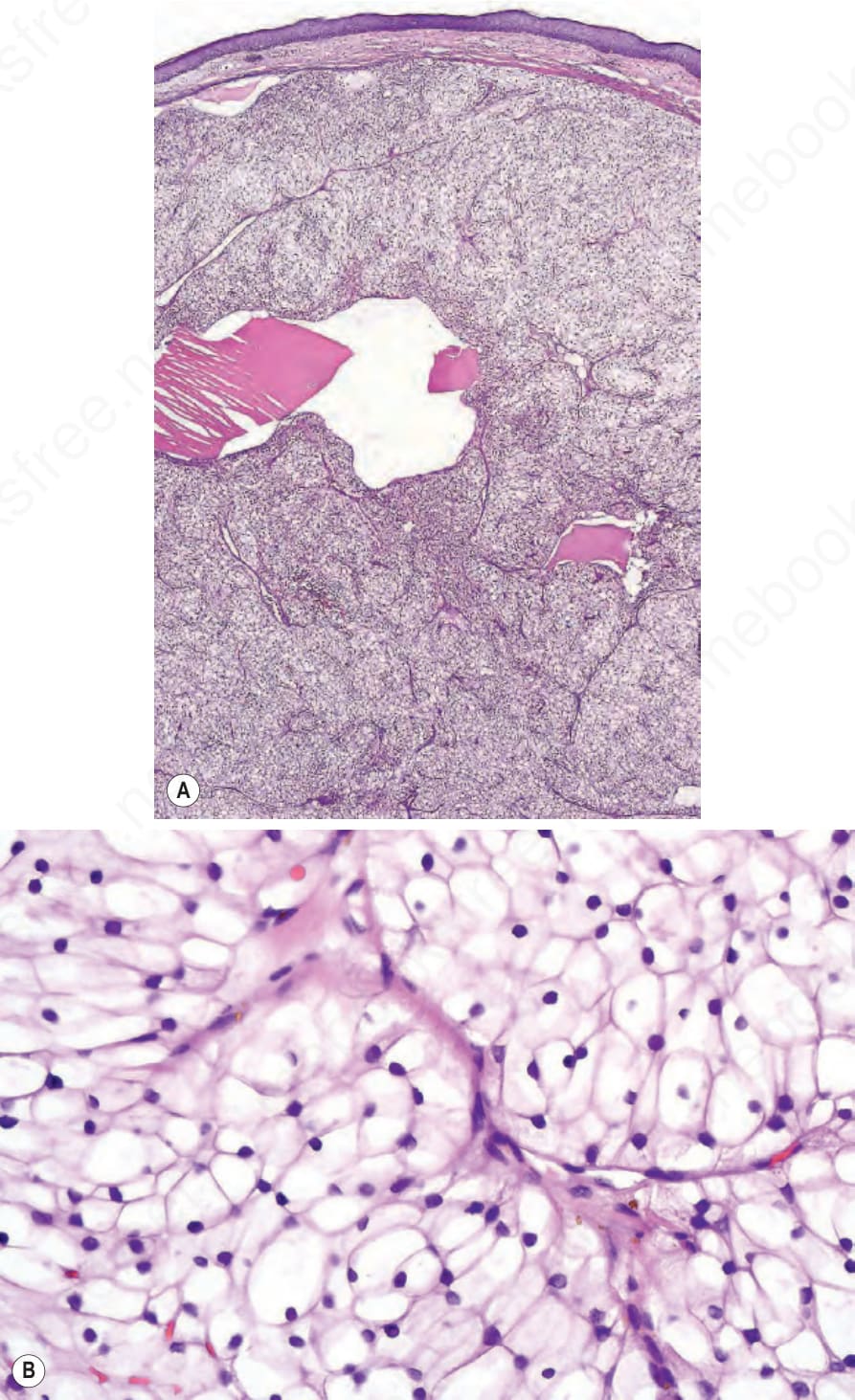
Fig. 33.135 (A, B) Eccrine hidradenoma: clear cell variant. The cells have clear cytoplasm and small hyperchromatic nuclei. The cytoplasm is PAS positive, diastase sensitive.
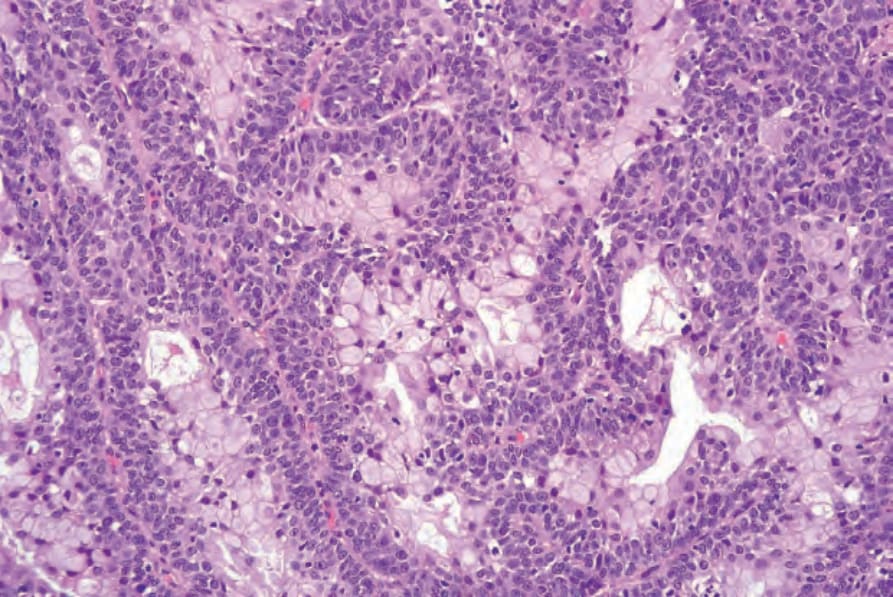
Fig. 33.136 Eccrine hidradenoma: in this field, there is mucinous metaplasia, which is an uncommon feature.
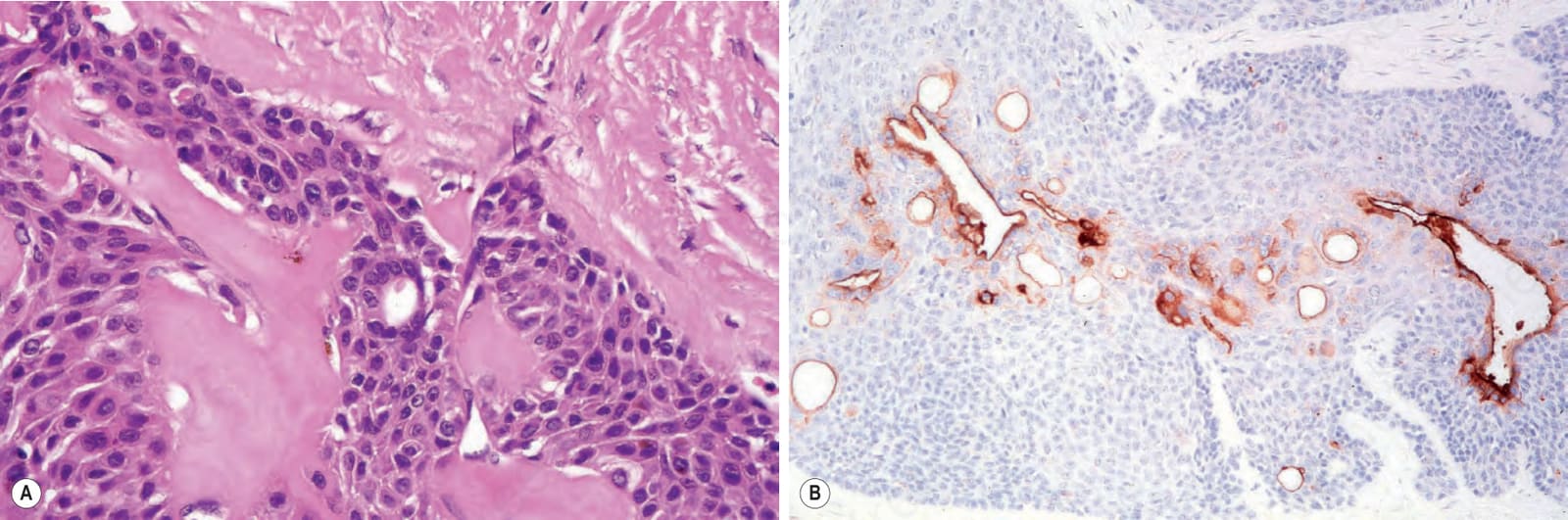
Fig. 33.137 Eccrine hidradenoma: (A) ductal differentiation as shown in this field is usually evident; (B) the ducts can be highlighted with EMA or CEA immunohistochemistry (EMA).
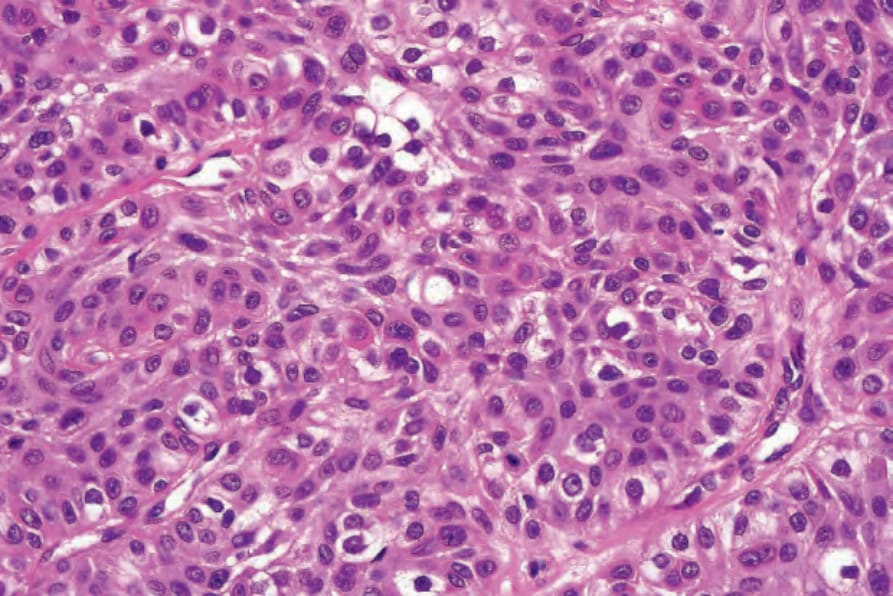
Fig. 33.138 Eccrine hidradenoma: note the intracytoplasmic lumen with eosinophilic cuticle.
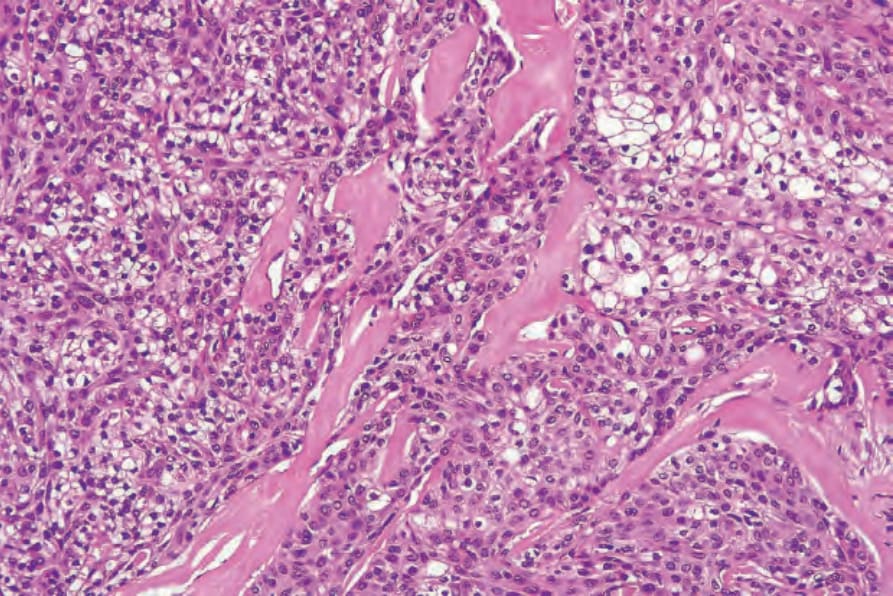
Fig. 33.139 Eccrine hidradenoma: in this field, the stroma is markedly hyalinized.
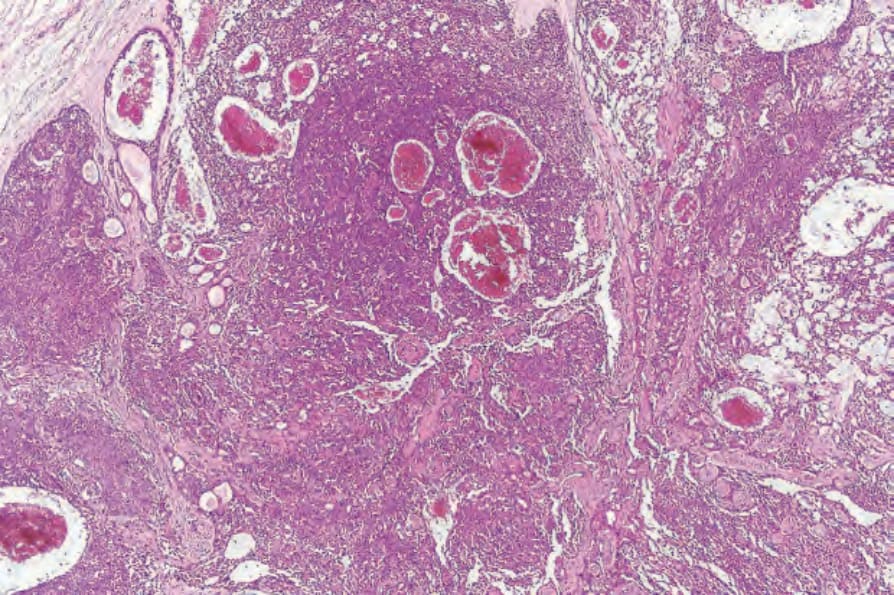
Fig. 33.140 Atypical eccrine hidradenoma: low-power view showing hemorrhage.