Syringoma
Syringoma
Clinical features Syringomas are common tumors and present most often as multiple, symmetrically distributed, usually asymptomatic, small papules (1–3 mm) on the lower eyelids and upper cheeks (Fig. 33.119).1,2 They appear at puberty or in early adult life and show a marked female predominance. Individual papules are firm and skin colored or slightly yellow (Fig. 33.120). Syringomas may, however, manifest a wide variety of clinical presentations. They may occur singly or in multiples on the scalp, forehead, neck, axillae, chest, abdomen, buttocks, extremities, or genitalia (male and female), periorally, or rarely, in a linear nevoid unilateral, segmental, or plaquelike pattern.1,3,4–26
A
B
A
B
1645 Syringoma
A
B
A
B
1646 Tumors of the sweat glands
A giant variant measuring up to 1 cm has also been described, and presentation as milia is an unusual finding.27–31 Patients with vulval syringomas often have coexisting eyelid lesions, and vulval pruritus is a frequent presenting symptom.12
An eruptive variant has been described in which successive crops of papules appear on the anterior surfaces of young people.32,33 Characteristic sites of involvement include the neck, chest, axillae, antecubital fossae, upper extremities, lower abdomen, and groins.32,34 Occasional familial examples have been recorded.34–39 Eruptive syringomas are more common in Orientals and are present in 18% of mature patients with Down syndrome.40–43 They may rarely be associated with milium cysts and vermiculate atrophoderma (Nicolau and Balus syndrome).44
A
Pathogenesis and histologic features Histochemical and electron microscopic studies have shown that the syringoma represents an adenoma of the acrosyringium, the intraepidermal eccrine sweat duct.45,46 Immunohistochemical studies further confirm differentiation of this tumor toward the acrosyringium or dermal eccrine duct.47–51 The epithelium of a syringoma therefore contains succinic dehydrogenase, phosphorylase, and leucine aminopeptidase.
The tumor is composed of interconnecting epithelial strands and ducts dispersed in a fibrous stroma within the upper dermis (Fig. 33.121). The ducts are lined by two layers of flattened cuboidal cells. There may be a cuticle lining the lumina, which frequently contains eosinophilic granular debris. Sometimes the ducts are associated with an epithelial strand, giving rise to the characteristic tadpole configuration (Figs 33.122 and 33.123). Occasionally, single glycogen-rich ductal cells are seen, and rarely all of the ductal cells contain glycogen, giving rise to the clear cell variant of syringoma. This appears to be particularly associated with diabetes mellitus.52,53
B
The milium-like variant of syringoma is characterized histologically by large epithelial-lined cysts containing keratinaceous material and located within superficial dermis.28 The features are otherwise characteristic of syringoma, and the keratin-filled cysts are immunoreactive against CEA.
Differential diagnosis Syringoma must be distinguished from desmoplastic trichoepithelioma, which typically features numerous keratocysts. Although there is obvious histologic overlap with eccrine epithelioma, the clinical features are quite different.2 Eccrine epithelioma, which is a much more extensive tumor that may involve the subcutaneous fat, is associated with a markedly desmoplastic stroma. Syringoma-like features are not usually extensive and infiltration of the perineural space is often observed. Mitoses are not a feature of syringoma. Distinction from microcystic adnexal carcinoma may be impossible in small biopsies, and clinicopathological correlation is therefore crucial.
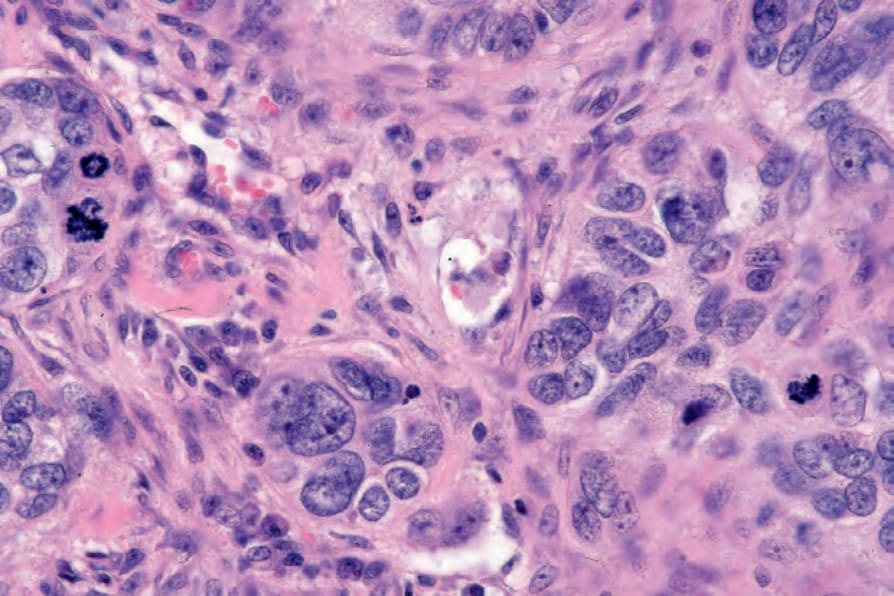
Fig. 33.107 Eccrine porocarcinoma: conspicuous mitoses are present.
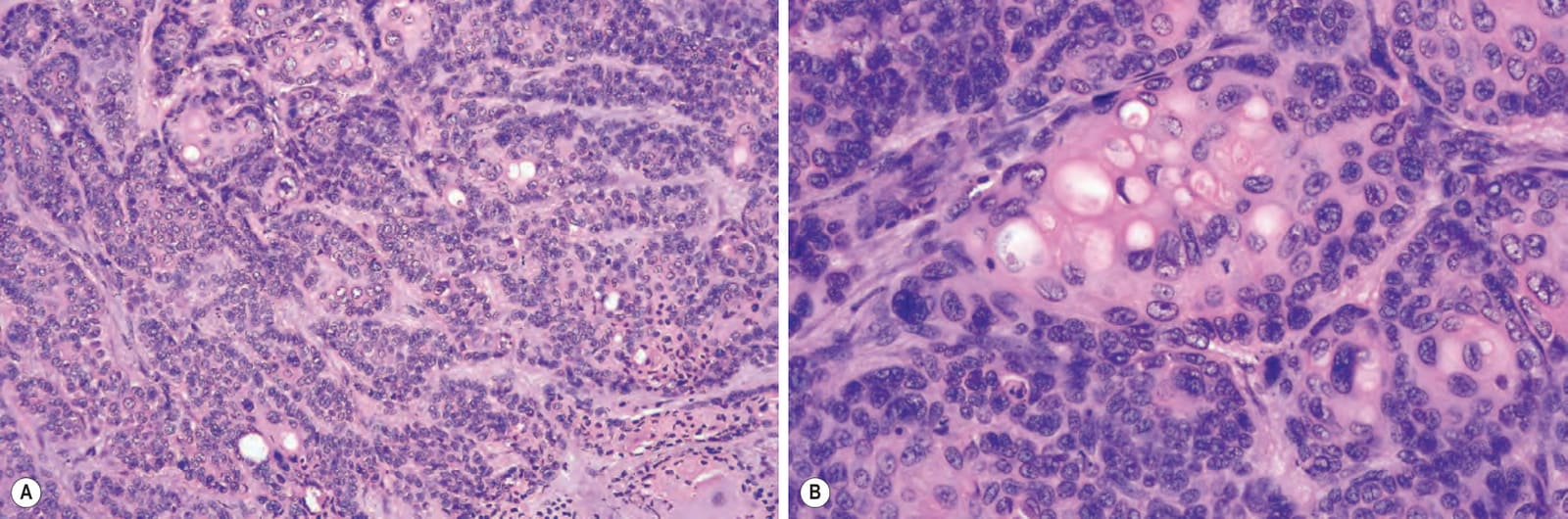
Fig. 33.108 (A, B) Eccrine porocarcinoma: ductal differentiation is an essential diagnostic feature.
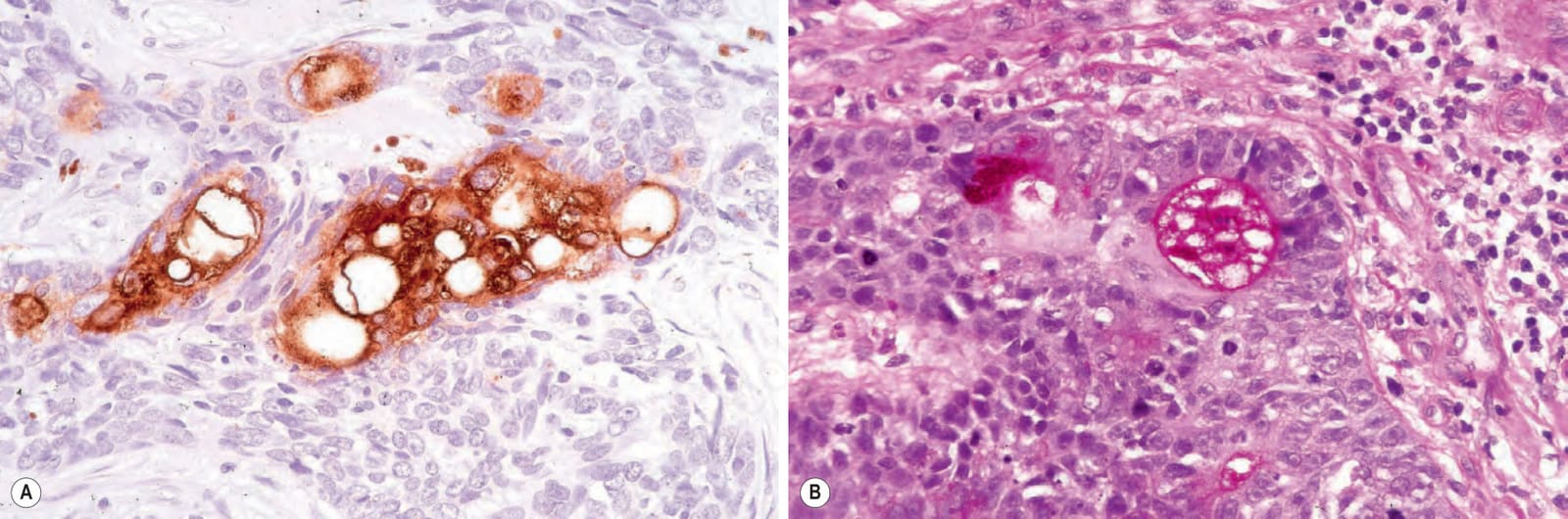
Fig. 33.109 Eccrine porocarcinoma: (A) ductal differentiation and intracytoplasmic lumina can be highlighted with EMA or CEA immunohistochemistry (EMA); (B) the luminal border of the duct is diastase resistant, PAS positive.
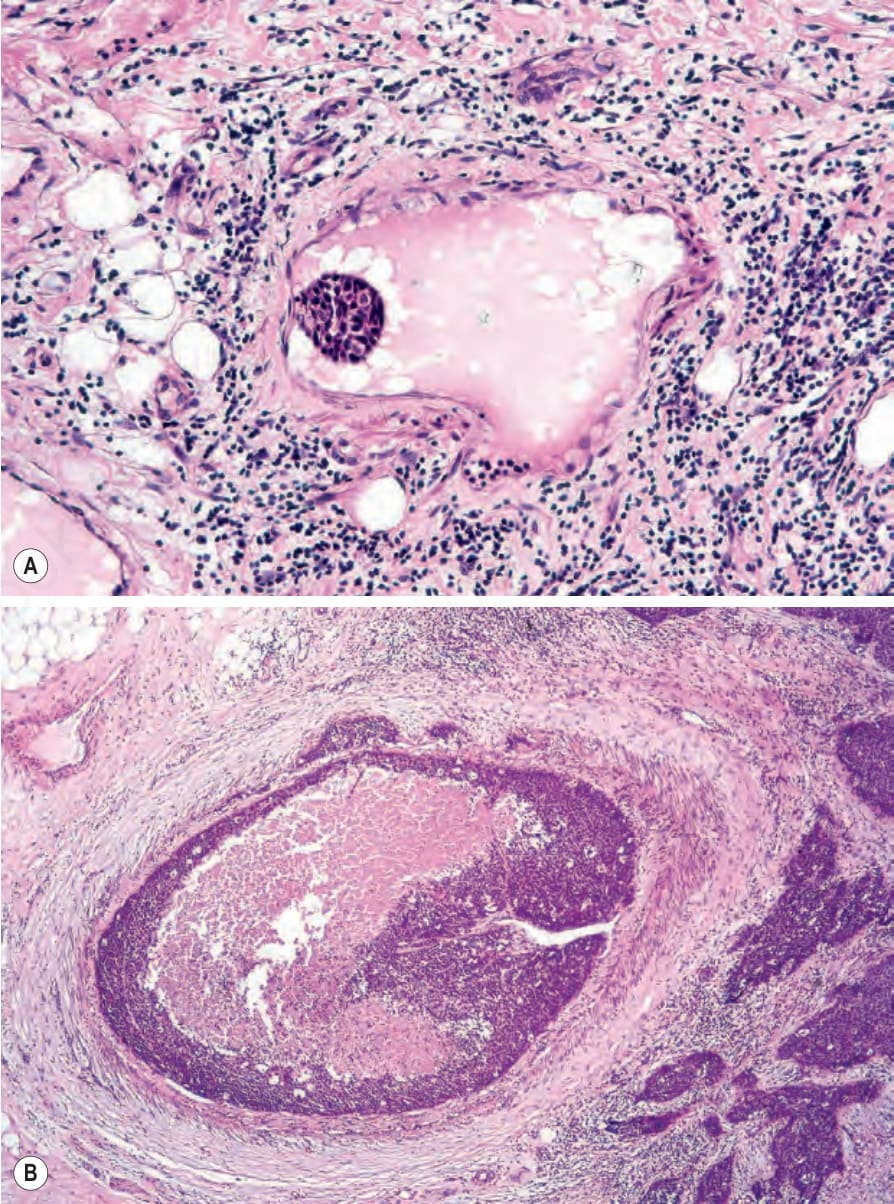
Fig. 33.110 (A, B) Eccrine porocarcinoma: lymphovascular invasion.
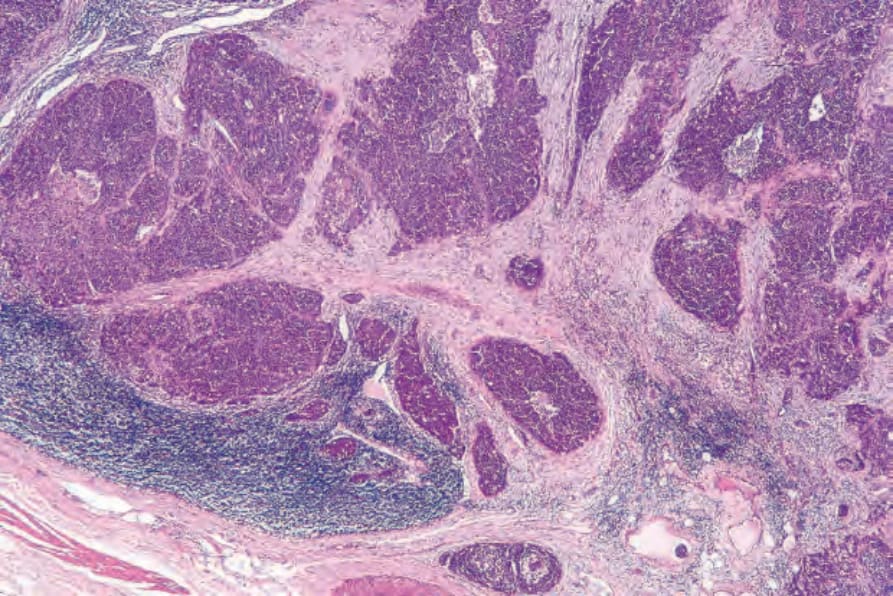
Fig. 33.111 Eccrine porocarcinoma: lymph node metastasis from the same patient as shown in Fig. 33.108B.
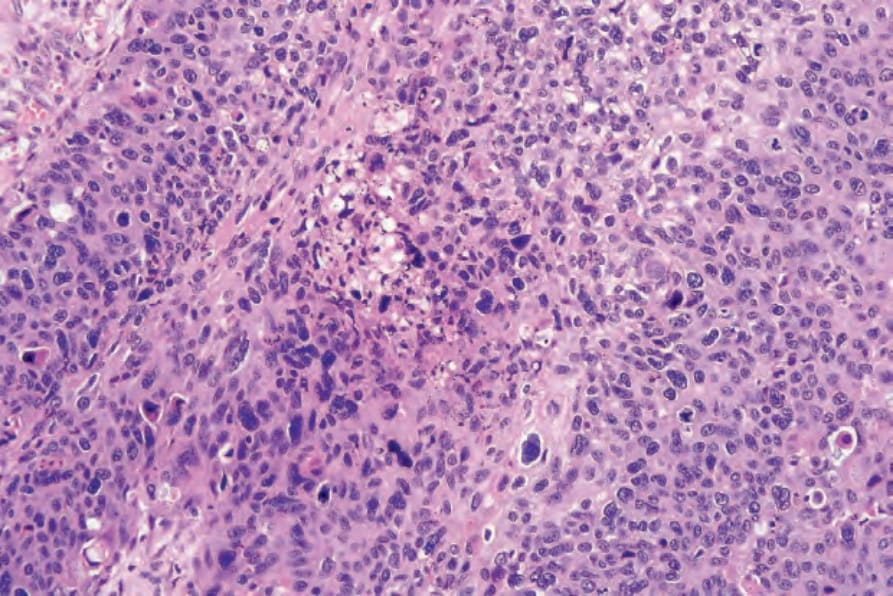
Fig. 33.112 Eccrine porocarcinoma: high-grade tumors commonly show areas of necrosis.
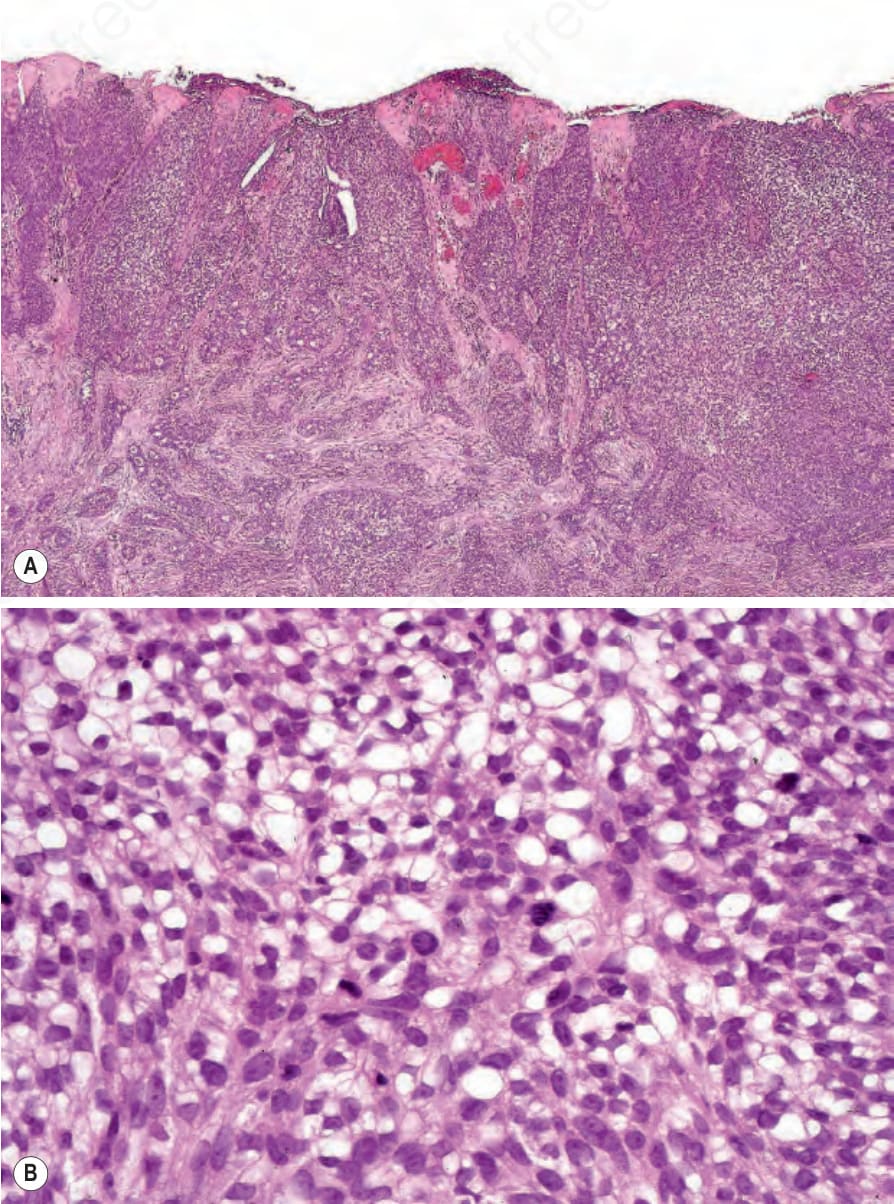
Fig. 33.113 Clear cell eccrine porocarcinoma: (A) there is striking cytoplasmic vacuolation; (B) high-power view.
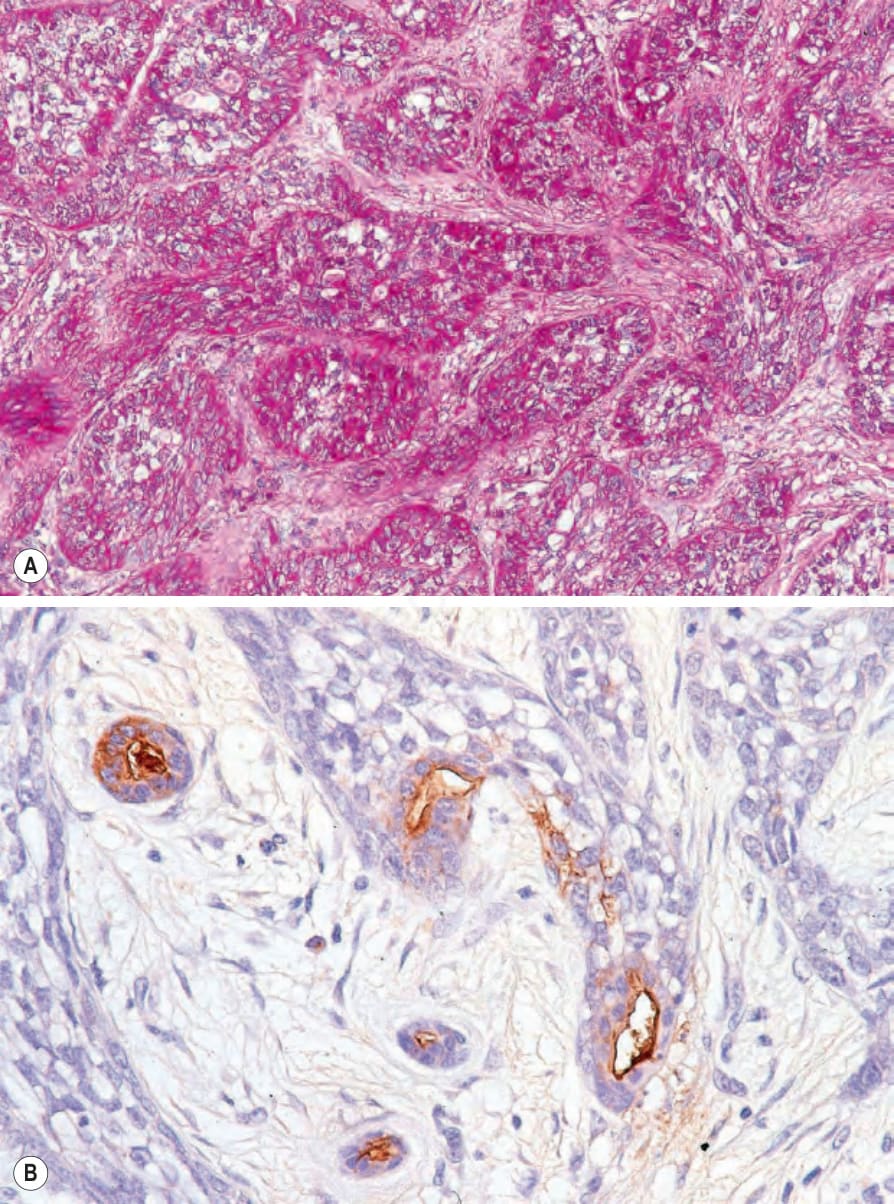
Fig. 33.114 Clear cell eccrine porocarcinoma: (A) the tumor cells are PAS positive; (B) EMA.
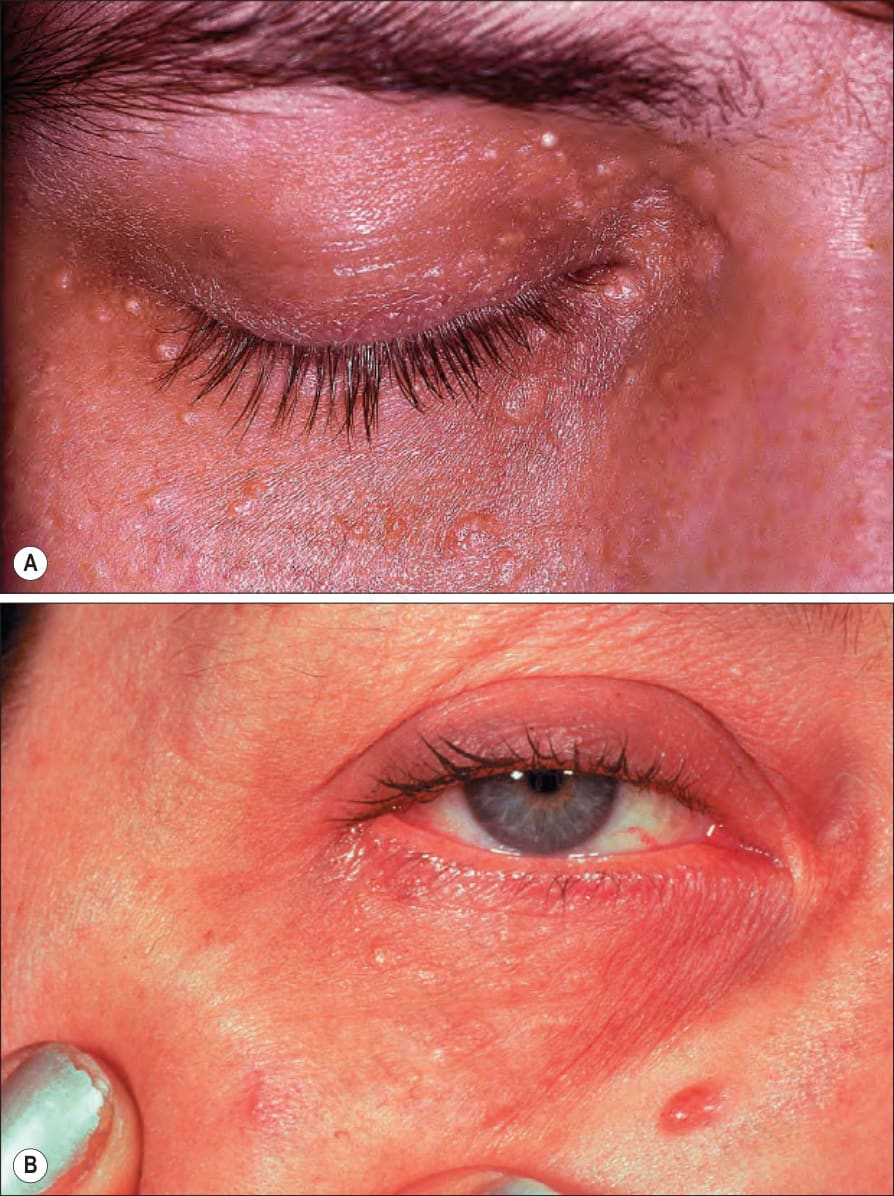
Fig. 33.119 (A, B) Syringoma: note the typical periorbital distribution of these small papules. (A) By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK; (B) by courtesy of the Institute of Dermatology, London, UK.

Fig. 33.120 Syringoma: there is extensive involvement of the cheek. From the collection of the late N.P. Smith, MD, Institute of Dermatology, London, UK.
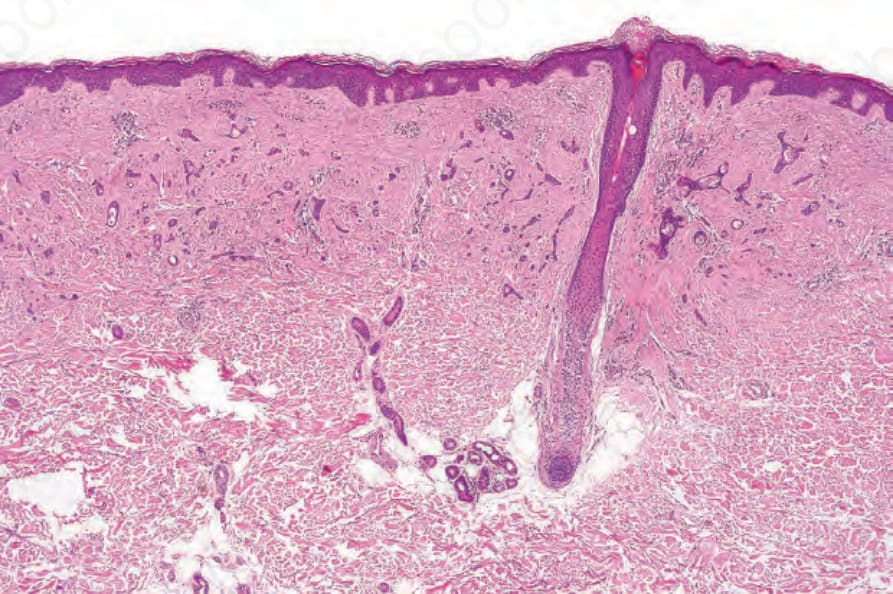
Fig. 33.121 Syringoma: characteristic epithelial strands and small cysts are present in the dermis. There is a dense, sclerotic fibrous stroma.
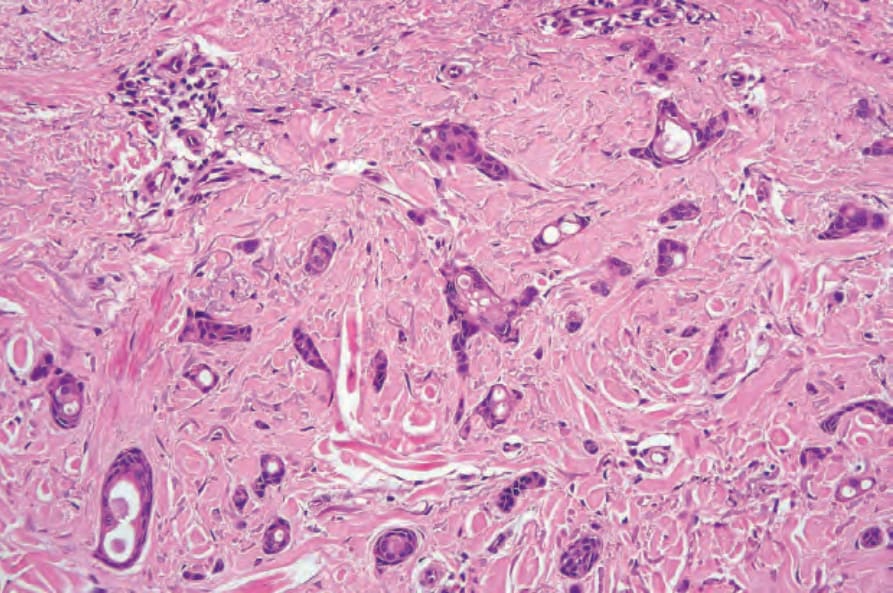
Fig. 33.122 Syringoma: note the epithelial strands and ductal differentiation.