Pilomatrixoma
Pilomatrixoma
Clinical features Pilomatrixoma (pilomatricoma, calcifying epithelioma of Malherbe) usually represents a solitary lesion, but occasionally multiple tumors are evident as part of an autosomal dominant disorder.1–6,7 Rarely, it may represent a dermatological marker of systemic disease (e.g., myotonic dystrophy, Gardner syndrome, or MYH-associated polyposis [MAP]).8–21 Multiple pilomatrixomas have also been reported in patients with Turner syndrome, trisomy 9, Rubinstein-Taybi syndrome, Sotos syndrome, and spina bifida.22–28 Synchronous appearance of multiple tumors is exceptional.29
mitoses, and geographic necrosis with or without perineural or lymphovascular invasion.35 Malignant proliferating pilar tumors may display aneuploidy, an increased proliferative index, and loss of staining for CD34 and wild-type p53 protein.44–46 Malignant proliferating pilar tumor has been reported to occur in patients with keratosis-ichthyosis-deafness (KID) syndrome and shows risk for distant metastasis and associated mortality.31,47
Differential diagnosis Usually, proliferating trichilemmal cysts can be distinguished from squamous cell carcinoma by the presence of multiple circumscribed nodules showing a noninfiltrative palisaded border, sometimes accompanied by a hyaline basement membrane and showing abundant trichilemmal rather than epidermoid keratinization.
It presents as a slowly growing, firm-to-hard nodule of around 0.5–3 cm on the head, upper limbs, neck, trunk, and lower limbs, in decreasing order of frequency (Fig. 31.52).2,20,30–32 The cheek is the most commonly affected site.33,34 Unusual locations include the spermatic cord and paratesticular region.35,36 Large chalky deposits are sometimes evident, and calcification may be revealed by radiology. Tumors are rarely extremely large, measuring up to 12 cm in diameter (giant pilomatrixoma).37–43 The overlying skin can be bluish, and show dilated vessels, bullous, anetodermic, or perforating changes.44–68
1561 Pilomatrixoma
Young people are mainly affected, with some 60% of cases being excised before 20 years of age and most before 10 years.3,69 There is a female predominance.2,30,33,34,69–72 More recent studies, however, have documented a somewhat wider age distribution with a second peak among those in their sixth and seventh decades of life.4,9,73–75 Surgical excision is curative although there is local recurrence in 2% to 3% of cases.1,33,34,71,76
Pathogenesis and histologic features Recently, insights have been gained into the molecular pathogenesis of pilomatrixoma implicating β-catenin as a key molecule. β-Catenin is an important intracellular protein with a dual role. It has a structural function and is involved in cell-cell junction formation by binding to cadherins as well as α-catenin, thereby providing a link between adherens junctions and the actin cytoskeleton.77–79 It is also part of the Wnt/wingless signal transduction pathway and mediating transcriptional activation of target genes such as c-myc and cyclin D1.80–82 Cytosolic β-catenin is phosphorylated at its N terminus and is subsequently subject to ubiquitin-mediated degradation involving the APC gene.83,84 Wnt signaling prevents phosphorylation of β-catenin leading to its cytosolic accumulation. Cytosolic β-catenin then interacts with lymphoid enhancer factor-1/T-cell factor (Lef-1/Tcf) to form a nuclear transcription factor complex.85,86 β-Catenin stabilization caused by truncating mutations in its N terminus (which prevents phosphorylation) has been shown to result in the formation of pilomatrixoma in a mouse model.87 These observations have led to the identification of mutations in the N-terminal portion of β-catenin in human pilomatrixoma predominantly affecting direct sites of phosphorylation.88–95 By immunohistochemistry, pilomatrixoma expresses cyclins D1, D2, and D3 and β-catenin nuclear staining within the basaloid/matrix cells while only cytoplasmic and membranous staining is observed in areas of maturation/transitional area. Staining is absent in ghost cells.96–101 Analogous to the findings in anagen hair follicles, the sequential expression of hair keratins is preserved in the transitional layer of pilomatrixoma, and there is subsequent loss of expression in the ghost cell layer.102,103 While cortical differentiation of matrix cells in anagen hair follicles is accompanied by LEF-1/α-catenin induced expression of the hair keratin hHa1, nuclear coexpression of LEF-1 and α-catenin is
not observed in the outer transitional layer of pilomatrixoma, arguing that cortical differentiation in pilomatrixoma is not under the control of the Wnt signaling pathway.104,105
Mutations in the β-catenin gene have also been identified in other tumors showing morphological overlap with pilomatrixoma including basal cell carcinoma with ghost cell differentiation, cribriform trichoblastoma, and craniopharyngioma.95
Differentiation of pilomatrixoma toward the hair matrix is supported by a number of studies on keratin, S100, and gene expression involved in the α-catenin pathway, and apoptosis represents the main mechanism leading to ghost cells.88,98,106–113
Pilomatrixoma is a tumor that expresses differentiation toward the hair matrix; hair shaft formation is therefore not a feature. The epidermis is usually normal, although rarely transepidermal elimination of tumor in addition to anetoderma-like changes and blister formation have been documented.3,48–55 Situated within the dermis and sometimes extending into the subcutaneous fat is a multilobulated tumor, which may on occasion be surrounded by a fibrous pseudocapsule of compressed adjacent connective tissue elements (Fig. 31.53). Individual tumor lobules are composed of a variable admixture of basaloid and ghost cells; the former predominate in evolving lesions and the latter in mature lesions.114 Basaloid cells are small and uniform with round vesicular nuclei and prominent nucleoli (Fig. 31.54). Early lesions may show very brisk mitotic activity, but this is never
1562 Tumors of the hair follicle
abnormal and is indicative of a rapid growth phase rather than malignant potential (Fig. 31.55). With tumor maturation, the basaloid cells transform into ghost cells, acquiring abundant eosinophilic cytoplasm and developing small hyperchromatic nuclei (Fig. 31.56). Eventually, the nuclei are lost, leaving sheets of intensely eosinophilic keratinous debris in which the ghost outlines of tumor cells are faintly visible, and giant cells are often present (Fig. 31.57). Keratinization in pilomatrixoma is therefore predominantly pilar, although occasionally small foci of epidermoid keratinization may be found. An additional feature in some tumors is melanin pigment within both basaloid cells and tumor histiocytes.3,115 Calcification is seen in 80% of lesions, more commonly in those that have achieved maturity.73 Basophilic stippling of ghost cells is the most common expression (Fig. 31.58). Rarely, large calcific concretions are present, and in 20% of cases ossification takes place (Figs 31.59 and 31.60).73 Bone morphogenetic protein-2 (BMP-2), an important molecule involved in bone and cartilage formation, has been demonstrated in shadow cells by immunohistochemistry and may play a role in bone formation in pilomatrixoma.116 Stromal amyloid deposition and focal clear cell change are occasionally seen (Fig. 31.61), and differentiation toward other aspects of the hair follicle including the follicular infundibulum and the inner root sheath as well as follicular germinal cells is a rare finding.117
A
B
1563 Pilomatrix carcinoma
Pilomatrixomas in the elderly generally show features similar to those of the childhood variant. Occasionally, however, atypical features include basaloid cell pleomorphism, loss of polarity, nuclear hyperchromatism, and marked mitotic activity including atypical forms.73,118 This variant has also been referred to as proliferating pilomatrixoma.118–120 Lymphatic and perineural spread are not features. These atypical variants do not appear to behave in any way differently from more conventional lesions. Nevertheless, their complete removal with careful follow-up is advised.
An unusual tumor showing features of pilomatrixoma in an intraepidermal location with cutaneous horn formation has been described as pilomatricomal horn.121 This tumor is characterized by papillomatous and thickened epidermis composed of well-defined lobules of matrical cells budding into papillary dermis. Tumor cells mature to produce ghost cells, and there is an overlying keratinaceous horn.
Differential diagnosis Although ghost cells are characteristic of pilomatrixoma, they can also be seen in a variety of other follicular neoplasms including infundibular cysts, trichoepithelioma, and its desmoplastic variant.122,123 Matrical differentiation may also sometimes be seen in basal cell carcinoma and combined cysts.

Fig. 31.52 Pilomatrixoma: note the small chalky nodule on the cheek of this young girl, a characteristic site. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
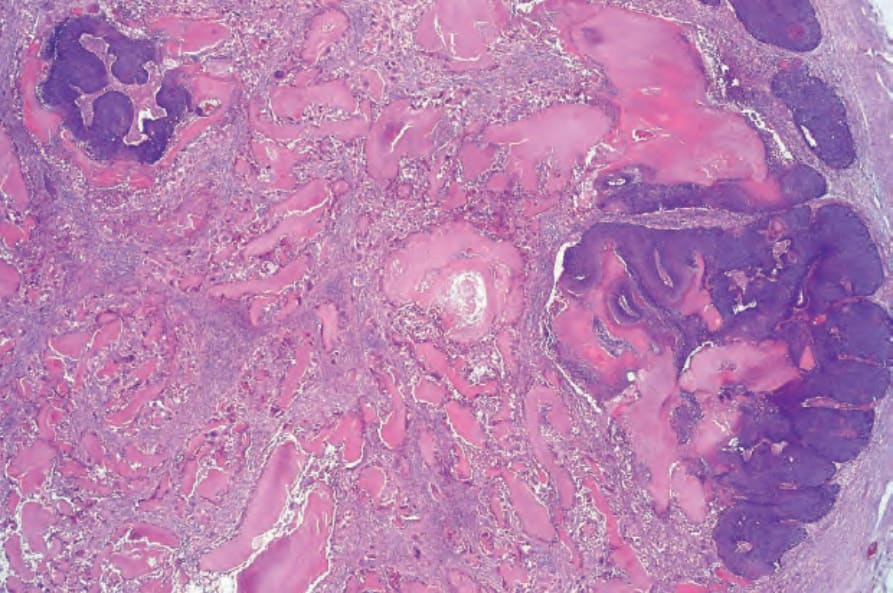
Fig. 31.53 Pilomatrixoma: this low-power view shows the typical biphasic population.
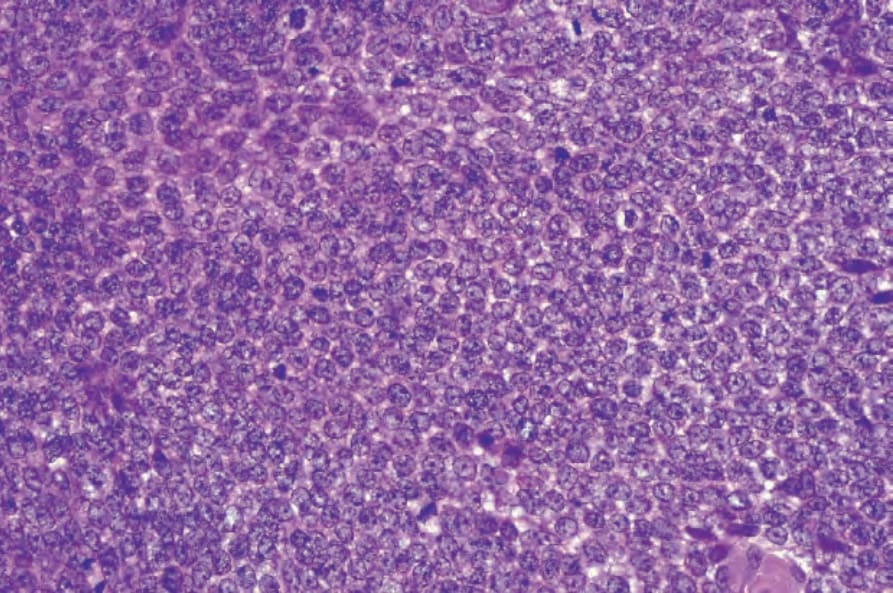
Fig. 31.54 Pilomatrixoma: early lesions are composed predominantly of sheets of germinative basaloid cells with uniform nuclei and small nucleoli.
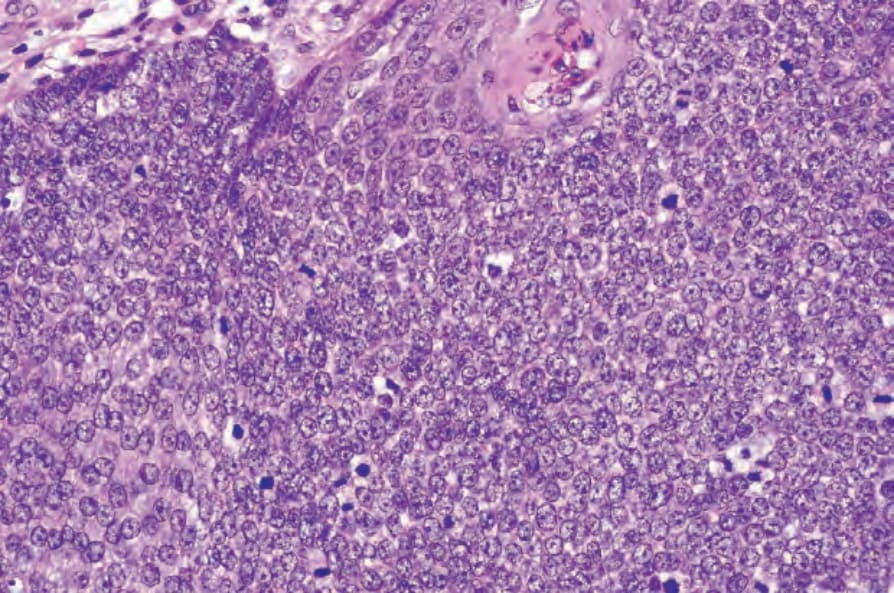
Fig. 31.55 Pilomatrixoma: note the presence of conspicuous mitotic figures. These are often numerous in early lesions and are not a cause for alarm.
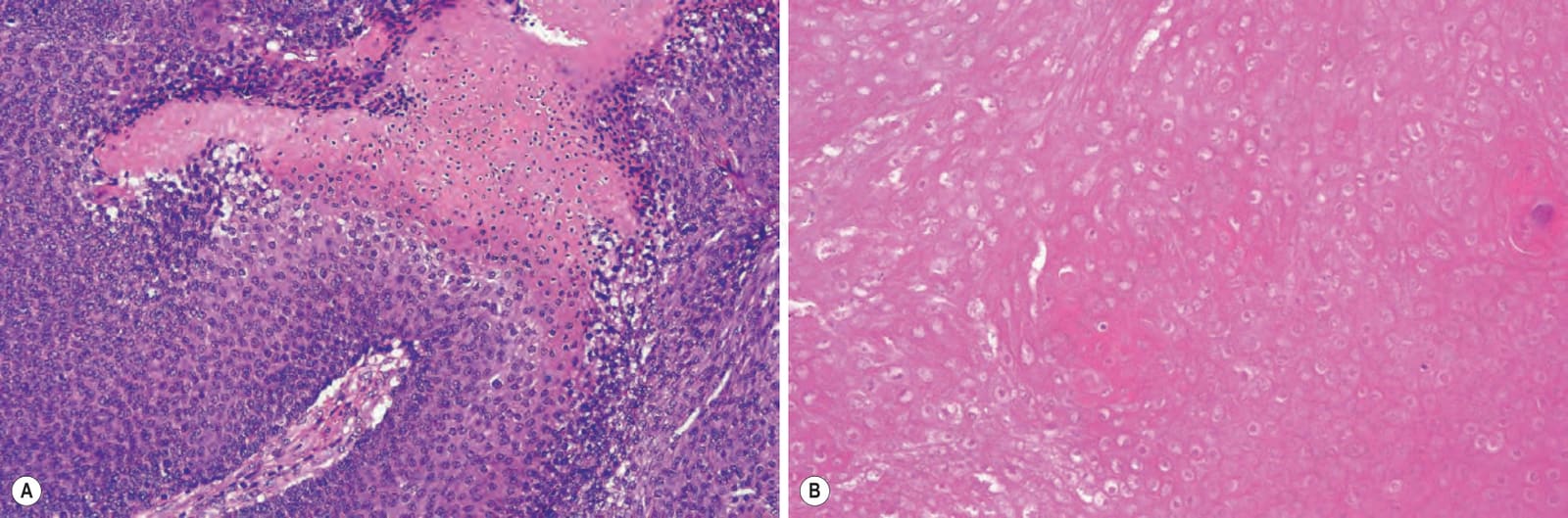
Fig. 31.56 (A, B) Pilomatrixoma: with maturation, the cells become larger, acquire abundant eosinophilic cytoplasm, and show nuclear pyknosis.
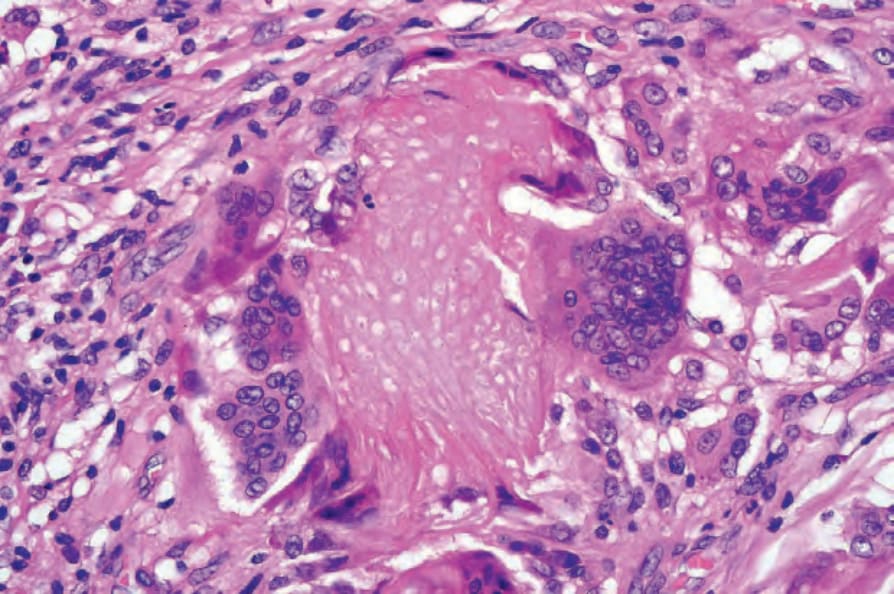
Fig. 31.57 Pilomatrixoma: a foreign body giant cell reaction is commonly present.
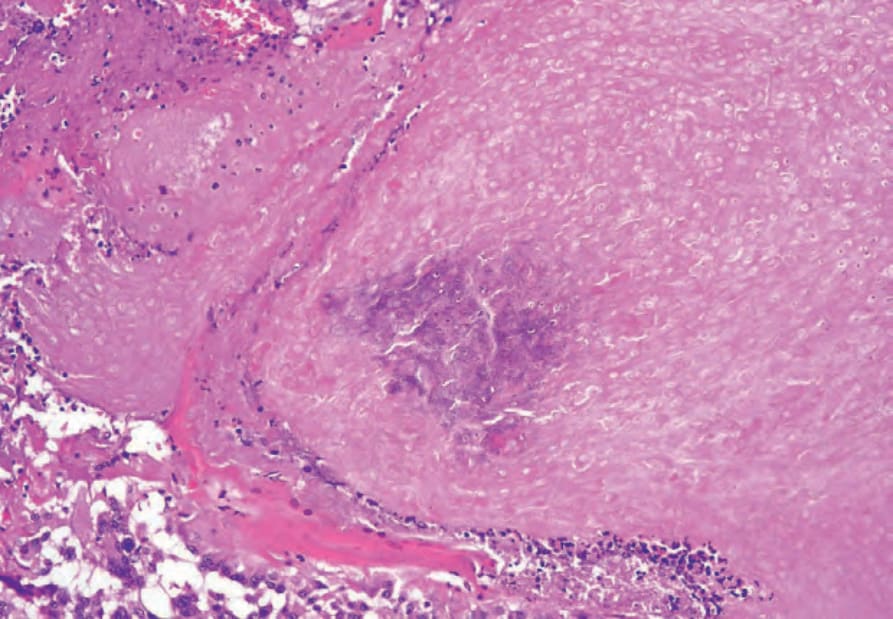
Fig. 31.58 Pilomatrixoma: note the fine basophilic calcification.
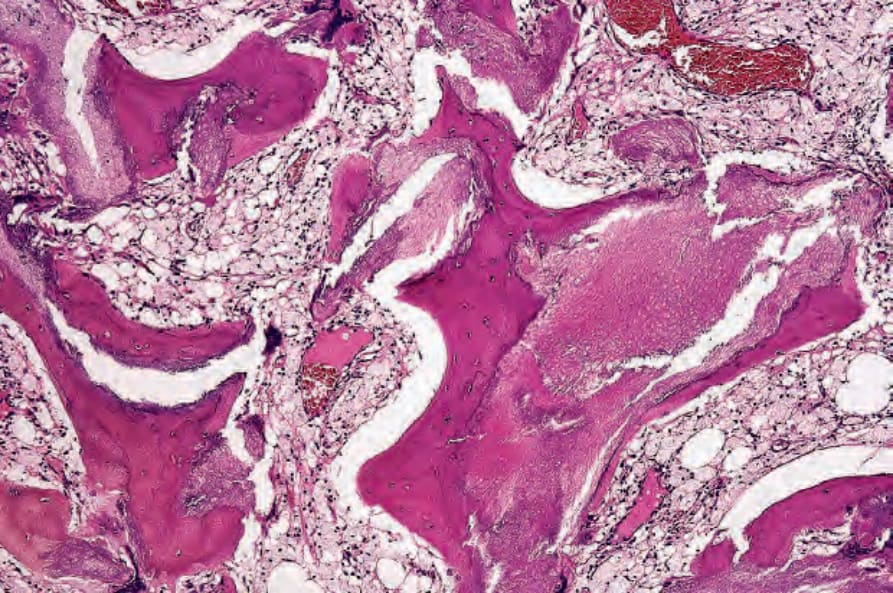
Fig. 31.59 Pilomatrixoma: this tumor shows widespread osseous metaplasia including the formation of marrow spaces.
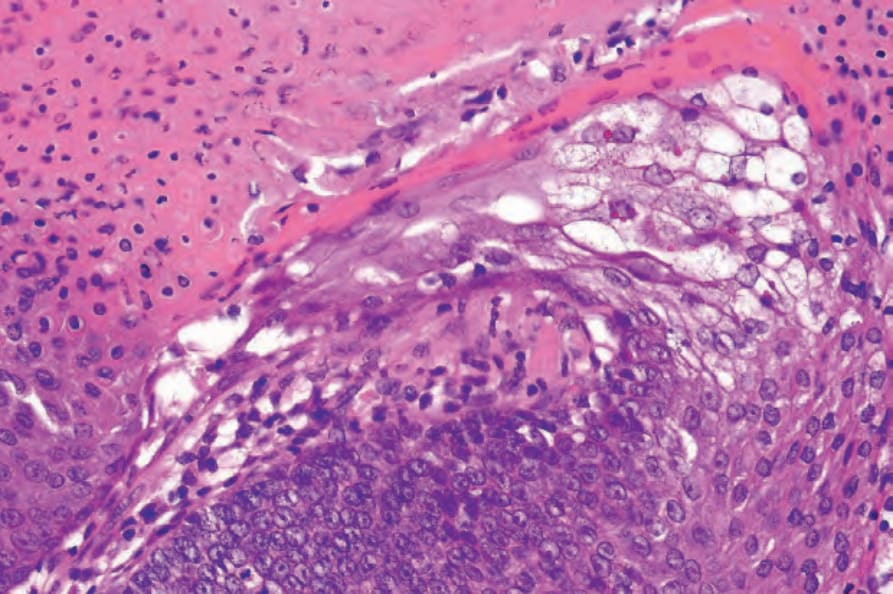
Fig. 31.61 Pilomatrixoma: high-power view showing focal clear cell change.