Mesothelioma
Mesothelioma
Metastatic cutaneous mesothelioma is exceptional.130,131 Most cases of cutaneous involvement by mesothelioma result from direct extension or are a consequence of implantation from surgical procedures. The most common sites of metastases are the trunk, face, and scalp. Rare cases of metastatic disease to the umbilicus and penis have been described.132,133
Histologically, mesothelioma can present with an epithelioid, sarcomatoid, or mixed morphology. Most mesotheliomas are predominantly epithelioid and, in this setting, distinction from a metastatic adenocarcinoma can be very difficult (Fig. 30.53).134 An exceptional case with pagetoid metastatic
1538 Cutaneous metastases and Paget disease of the skin
A
B
spread has been described.133 There are no antibodies that are entirely specific for mesothelioma. Immunohistochemical markers including keratin, carcinoembryonic antigen (CEA), B72.3, Leu-M1, WT1, and Ber-EP4 are used routinely to try to establish a diagnosis.28,135,136 Mesotheliomas tend to be negative for all these markers except for keratin, which is consistently positive, and Ber-EP4. Staining for CK5/6 can also be helpful, as mesotheliomas are positive for this marker and metastatic adenocarcinomas tend to be negative.137 Calretinin may be positive in mesotheliomas, but is not specific (Fig. 30.54).74
the terminal ileum and appendix; those at the latter site are almost invariably benign. The rest develop in the colon, stomach, bronchus, and, very rarely, in the gallbladder and in ovarian teratoma. The bronchus appears to be the most common primary site in the setting of cutaneous metastasis.143 Rarely, patients can present with symptoms of the carcinoid syndrome.
Ultrastructurally, mesothelioma cells contain numerous characteristic elongated surface microvilli.
Carcinoid tumor Carcinoid tumor is uncommon, shows a predilection for females, and presents most often in the seventh decade. Although primary cutaneous lesions do occur very exceptionally, it is most probable that a cutaneous lesion represents metastatic disease.138–142 The majority of carcinoid tumors arise in
There is usually, although far from invariably, a positive argentaffin reaction; some tumors require the presence of an additional reducing agent – the argyrophil reaction. Occasional tumors, however, show neither of these reactions.
Histologically, the tumor has a characteristic appearance of variably sized nodules of strikingly uniform cells (Fig. 30.55). The cells have regular, round to oval, vesicular nuclei and show a tendency towards peripheral palisading. The cytoplasm is eosinophilic, and granules may be especially evident at the periphery of the nodules. Mitotic activity is usually low. Diagnosis can be confirmed by a variety of techniques including the diazo reaction, the Masson-Fontana technique, and Pearse lead-hematoxylin reaction. In addition, the tumor cells express chromogranin, synaptophysin, PGP 9.5, CD56, and neuron-specific enolase (Figs 30.56 and 30.57). Carcinoid tumors are usually negative for CK5/6 and p63, and this may be useful in the distinction from benign cutaneous adnexal tumors as the latter tend to be positive for these markers.144
1539 Individual tumors
extremely challenging.145 Amelanotic spindle cell deposits may be confused with spindle cell squamous carcinoma, atypical fibroxanthoma, or metastatic spindle cell sarcomas, particularly leiomyosarcoma. In these instances, the use of the Masson-Fontana reaction may reveal melanin pigment in quantities insufficient for easy detection using conventional hematoxylin and eosin staining. The diagnosis may also be facilitated by the use of S100 protein, Melan-A, MITF-1 (microphthalmia transcription factor 1), SOX10, and HMB-45 immunohistochemistry. Malignant smooth muscle tumors are distinguished by immunohistochemical evidence of actin, desmin, and h-caldesmon expression. Although most cases of metastatic melanoma lack an epidermal component, metastatic melanoma may occasionally be associated with prominent epidermotropism.146–149 In this setting, distinction from a primary melanoma is far from easy. When amelanotic, immunohistochemistry may be necessary to exclude the diagnosis of extramammary Paget disease. On histologic grounds alone, amelanotic melanoma with balloon cell change or the exceptional signet ring change can be very difficult to distinguish from primary adnexal or metastatic tumors.150
Metastatic melanoma Melanoma is the third most common source of cutaneous metastases (Fig. 30.58).35 Metastatic melanoma usually poses little diagnostic difficulty. In up to 5% of patients, a metastatic melanoma to skin is the first manifestation of the disease; if amelanotic, the histologic differential diagnosis can be
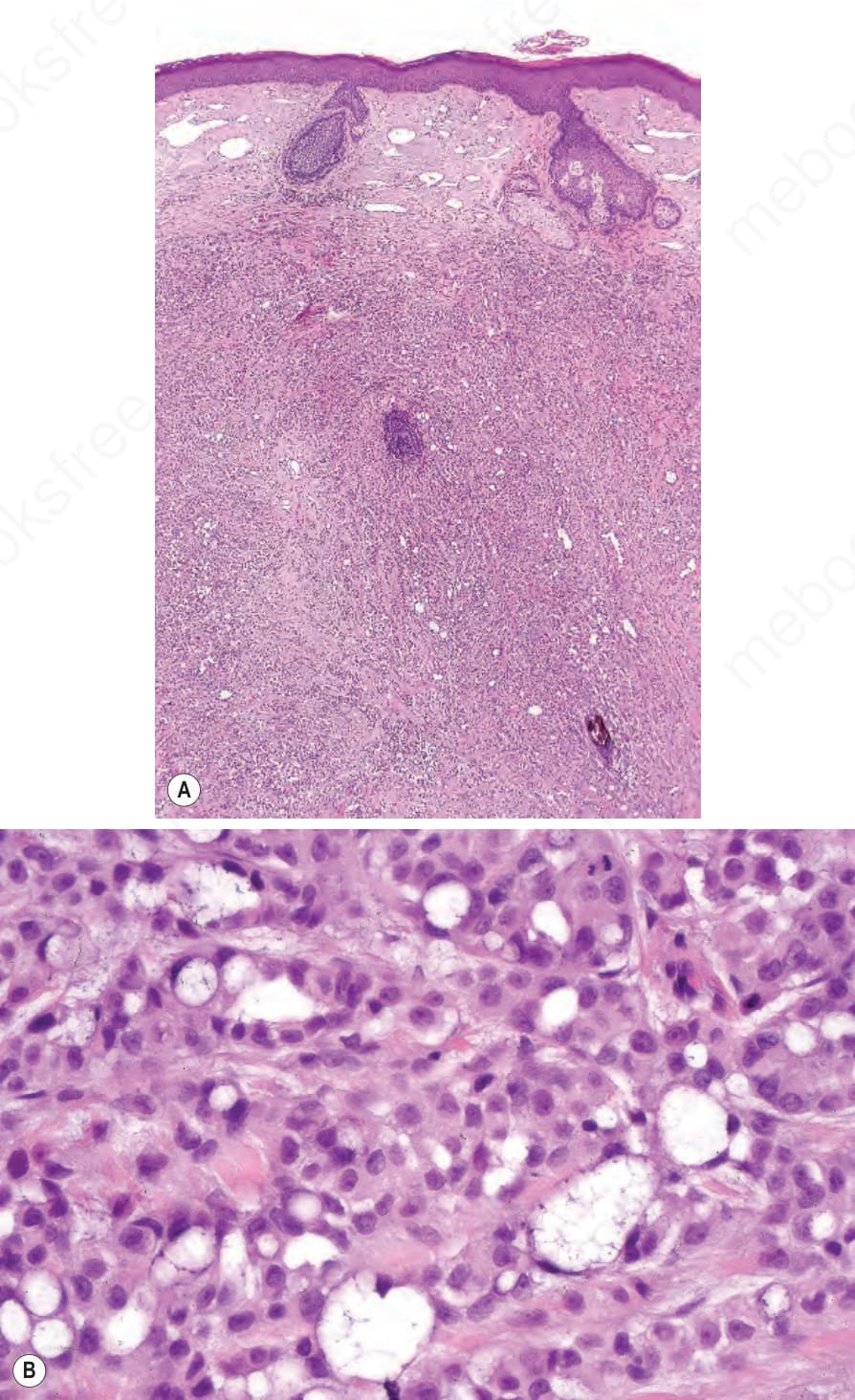
Fig. 30.53 Metastatic mesothelioma: (A, B) the features are indistinguishable from poorly differentiated carcinoma.
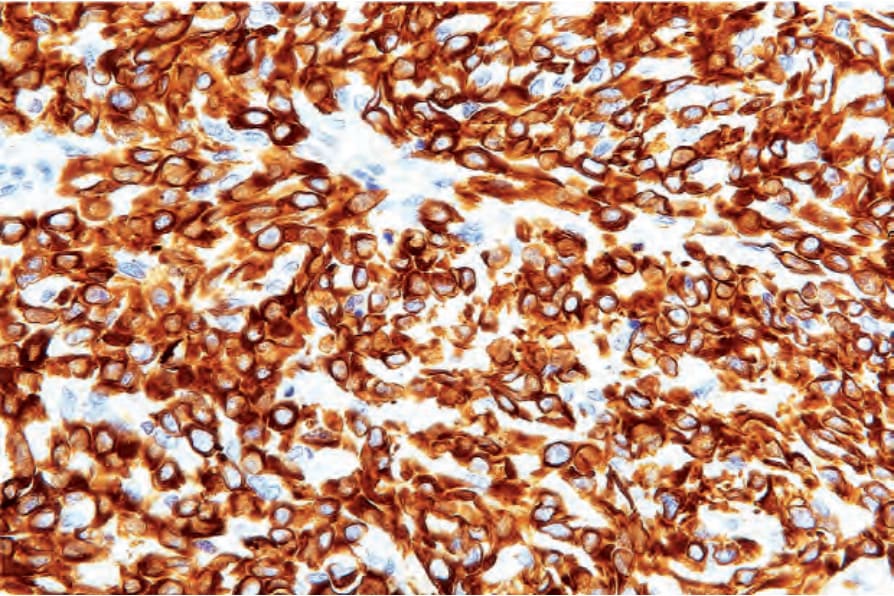
Fig. 30.54 Metastatic mesothelioma: the tumor cells are strongly positive for calretinin.
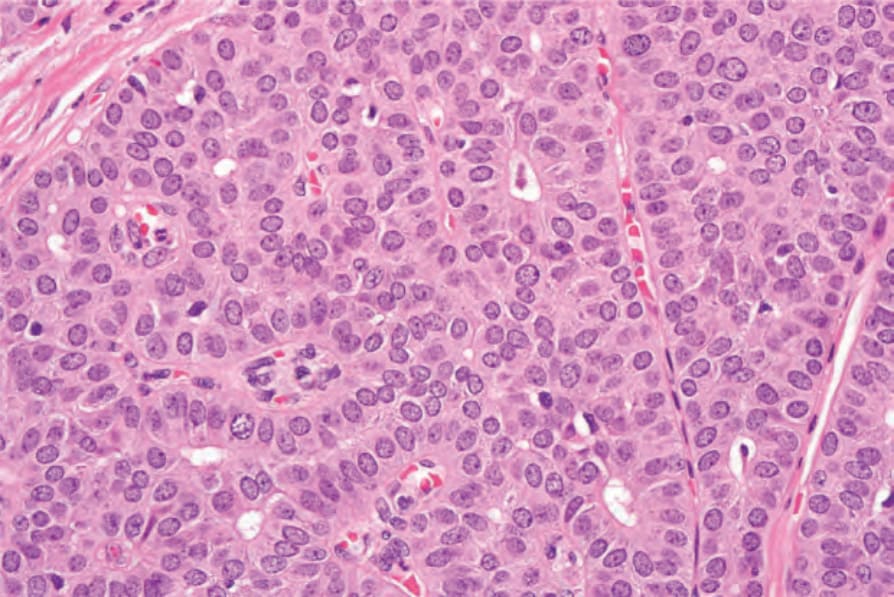
Fig. 30.55 Metastatic carcinoid tumor: note the uniform nuclear morphology, eosinophilic cytoplasm and acini.
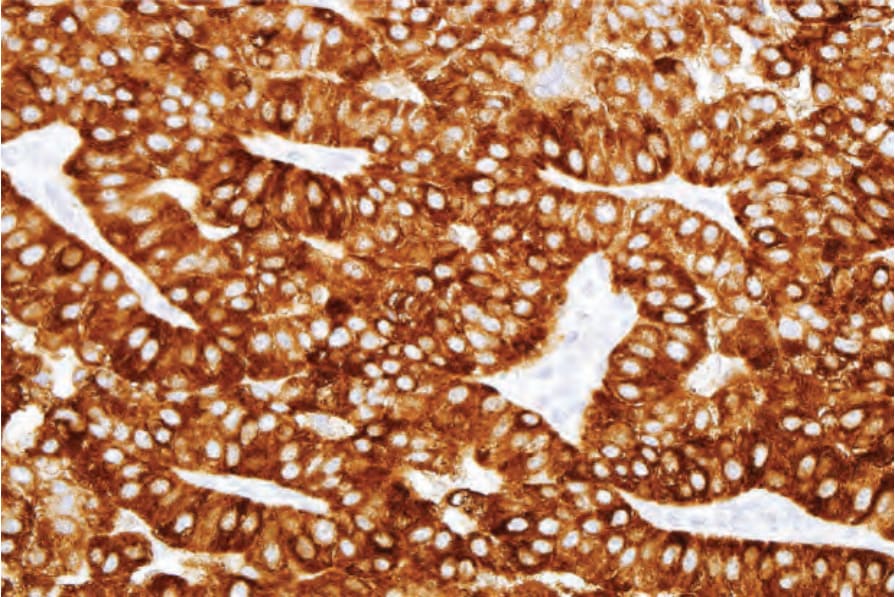
Fig. 30.56 Metastatic carcinoid tumor: the tumor cells are strongly positive for synaptophysin.
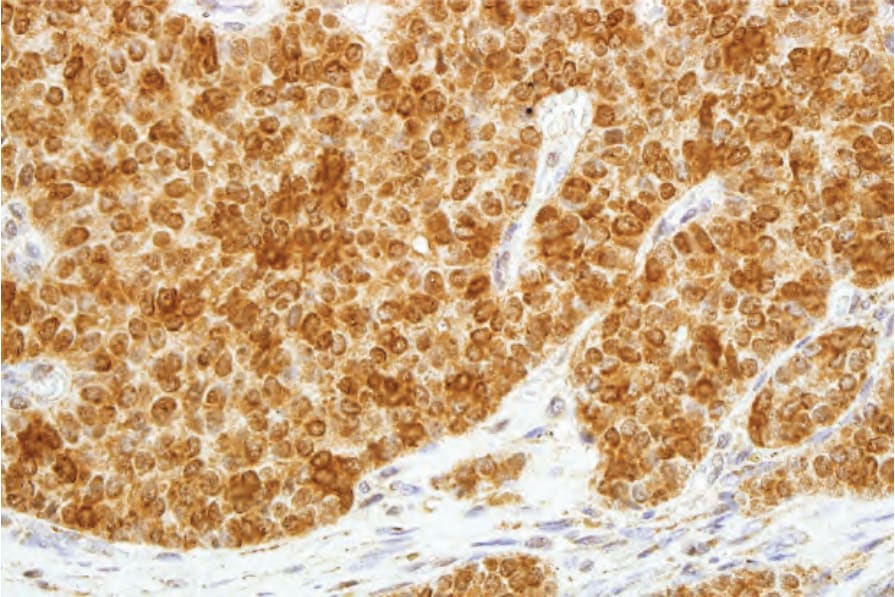
Fig. 30.57 Metastatic carcinoid tumor: neuron-specific enolase (NSE) is also expressed.
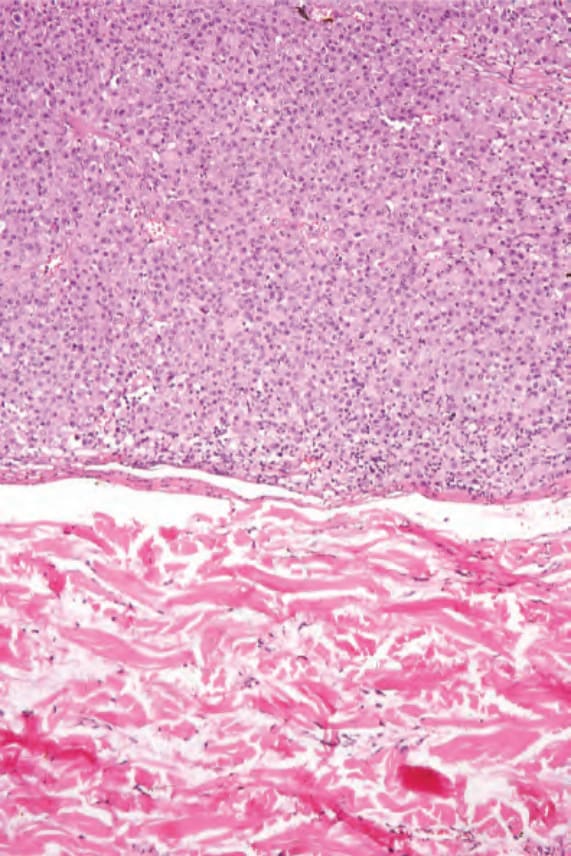
Fig. 30.58 Metastatic melanoma: the circumscribed, nodular growth pattern is very suggestive of a metastasis. Although amelanotic, the tumor cells expressed S100 protein and HMB-45.