Cutaneous extramedullary hematopoiesis
Cutaneous extramedullary hematopoiesis
Clinical features Extramedullary hematopoiesis (EMH) (myeloid metaplasia) describes the development of hematopoietic tissue outside the bone marrow. Most frequently, EMH is associated with an underlying myeloproliferative neoplasm or myelodysplastic syndrome, usually chronic idiopathic myelofibrosis.1–9
Rarely, it is seen following marrow replacement by lymphoma or metastatic carcinoma, in storage disorders, and in patients with severe anemia from many causes, including hereditary spherocytosis, sickle cell anemia, Rhesus incompatibility, and twin-to-twin transfusion.5,7 It has also been described following severe intrauterine infection and in patients receiving myeloid growth factors.5,7,10,11
EMH is mainly seen in the liver and spleen. EMH elsewhere is rare.10,12–14
The clinical presentation in skin is variable, lesions being described as
The majority of systemic mastocytosis cases belong to an indolent group, but rare aggressive variants also exist, and are defined according to further clinical and laboratory parameters. The following subtypes of mastocytosis that will be recognized in the 2016 update of the WHO classification are:2
• cutaneous mastocytosis,
• systemic mastocytosis,
• indolent systemic mastocytosis,
• smoldering systemic mastocytosis,
• systemic mastocytosis with an associated hematological neoplasm,
• aggressive systemic mastocytosis,
1516 Cutaneous lymphoproliferative diseases and related disorders
Cutaneous mastocytosis Typical clinical findings of urticaria pigmentosa/maculopapular cutaneous mastocytosis or solitary mastocytoma with appropriate histologic mast cell infiltrates in skin biopsy. Absence of criteria for systemic mastocytosis.
Systemic mastocytosis Requires presence of major criterion and one minor criterion, or at least three minor criteria.
Major criterion: Multifocal infiltrates of mast cells in bone marrow and/or other extracutaneous organ(s); must be ≥15 mast cells/aggregate
Minor criteria:
-
25% spindle shaped or otherwise atypical mast cells in biopsy sample
- Activating point mutation at codon 816 of KIT
- Aberrant expression of CD2 and/or CD25 by mast cells
- Serum tryptase >20 ng/mL in absence of associated clonal myeloid
disorder
Modified from Horny, H.P., et al. (2008) WHO classification of tumors of haematopoietic and lymphoid tissues. Swerdlow, S.H., Campo, E., Harris, N.L., et al (eds). Lyons: IARC Press, pp 54–63.
• mast cell leukemia,
• mast cell sarcoma. A full discussion of the intricacies of this subclassification is beyond the scope of this text (see references 1–3 and 5), and although general clinical features of systemic mastocytosis are summarized below, detailed discussion is limited to cutaneous disease.
Clinical features Patients may be affected at any age. Cutaneous mastocytosis is most common in children, may be present at birth, and up to half of cases manifest in the first 6 months of life. It is much less frequent in adults, most cases of skin involvement in this age group being associated with systemic mastocytosis.5,10–12 Systemic mastocytosis generally arises after the second decade. There is no clear sex or ethnic predilection.13,14 Skin lesions are common in mastocytosis, overall being present in 80% of patients, including 50% of cases of systemic mastocytosis. Bone marrow is almost always involved in systemic mastocytosis, and there may rarely be a leukemic blood picture with significant numbers of circulating mast cells.15–20 Virtually any other tissue may be involved, but the most frequently reported are spleen, lymph node, liver, and gastrointestinal tract.7,8,15,18,21–23
to 30% of patients with systemic mastocytosis, either preceding, concurrent with, or succeeding the mast cell disease. This is usually chronic myelomonocytic leukemia, but may be myelodysplasia, AML, lymphoma, or any other recognized hematological malignancy.4,5,17,32–37 Such cases fall into the systemic mastocytosis category of ‘systemic mastocytosis with an associated hematological neoplasm’.2
Cutaneous involvement in the absence of criteria for systemic mastocytosis is subdivided into one of three clinicopathological variants:
• solitary mastocytoma,
• maculopapular mastocytosis/urticaria pigmentosa,
• diffuse mastocytosis. Skin is also frequently involved in indolent forms of systemic mastocytosis, but much less often not in aggressive variants. It may also be a presenting site for very rare cases of mast cell sarcoma.
Symptoms are often related to release of a wide range of mast cell mediators, as well as to the direct effects of organ infiltration. These include histamine, eicosonoids, proteases, and heparin. They may induce localized or more generalized reactions such as anaphylaxis, flushing, headache, urticarial rhinitis, palpitations, and hypotension with syncope.4,24,25 Gastrointestinal symptoms include vomiting, colicky abdominal pain, peptic ulceration, and diarrhea.4,7 In the skin, mast cell degranulation also accounts for the common presence of pruritus, a positive Darier sign, and dermographism (Fig. 29.346). Darier sign refers to localized swelling or urticaria induced by stroking of a lesion; this may reach bullous proportions.

Fig. 29.346 Mastocytosis: a classic example of dermographism.
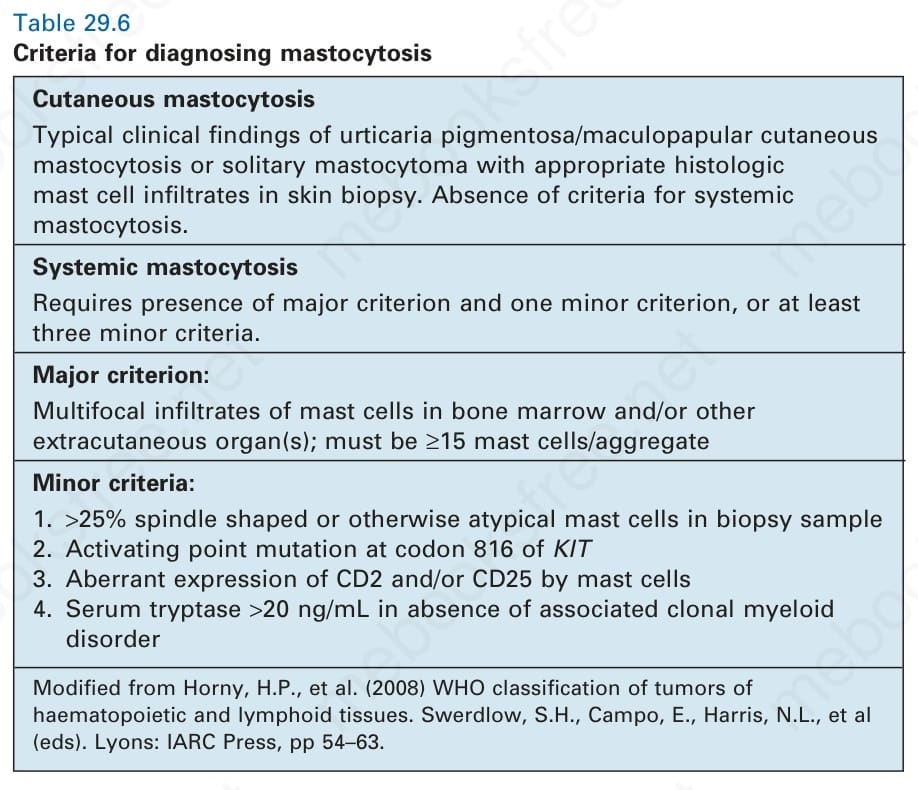
Table 29.6 Criteria for diagnosing mastocytosis