Myeloid sarcoma
Myeloid sarcoma
Clinical features Myeloid sarcoma (MS) is defined as a tumor or mass of myeloblasts, with or without maturation, occurring at a site other than the bone marrow. The term leukemia cutis is often used to denote cases with skin involvement. MS occurs in the absence of other evidence of acute myeloid leukemia (ML) in about 25% of cases. A diagnosis of MS equates with one of AML, and the patient should be investigated, classified, and treated accordingly.1–6 In 35% of cases, MS is diagnosed simultaneously with another hematological malignancy, most frequently AML, but sometimes a myeloproliferative neoplasm or a myelodysplastic syndrome.1–3,7–10 In the remaining cases (approximately 40%), there is a previous history of hematological malignancy or myelodysplasia.1–3,11–13 Thus, MS may be the first sign of relapse in a patient with AML previously in complete remission, or indicate transformation to acute leukemia in patients with myeloproliferative disorders or
1513 Myeloid sarcoma
myelodysplastic syndromes. The commonest sites of presentation are in the skin (28.2%), lymph nodes (16.35%), testes (6.5%), intestine (6.5%), bone (3.25%), and CNS (3.25%), although virtually any tissue may be affected.2,3
Cutaneous MS is relatively uncommon and reported in between 2% and 30% of AML patients.14–19 There is an equal sex incidence, and it is seen in a wide range of ages.11,14,20,21 There is no clear site predilection, and the clinical appearances are varied and often non-specific. Erythematous or violaceous papules and nodules (which may be purpuric) are the most frequent clinical findings, but infiltrative plaques and, less commonly, macules, ulcers, and rarely blisters, are also sometimes seen (Fig. 29.341).20–23 Oral manifestations are not uncommon and include papules, nodules, and ulcers. Gingival hypertrophy may be found in patients with acute monocytic and myelomonocytic leukemia.22–27
Previously, it was suggested that skin involvement by AML was a poor prognostic indicator.15,28,29 However, a large study of MS showed that clinical behavior and response to therapy was not influenced by age, sex, anatomic location, de novo presentation, clinical history related to other myeloid neoplasms, histologic features, immunophenotype, or cytogenetic findings.2 Patients treated with intensive chemotherapy and bone marrow transplantation have the best chance of survival.2,30
appearance.2,11,15,36,37 Varying degrees of granulocytic differentiation may be seen, and immature eosinophils are common (Figs 29.342 and 29.343).21,29
The immunophenotype varies depending on the degree and type of maturation present. In cutaneous MS, this is often monocytic or monoblastic in nature. There may be expression of myeloid markers, such as myeloperoxidase, CD33, and CD117, but often at lower frequency compared to AML confined to bone marrow. Conversely, expression of CD4, CD14, CD68, and CD163 is more frequent. CD56 may also be expressed, but CD123 and CD303 are only present in a small minority, and CD34 is often also negative.11,20,36,37
Pathogenesis and histologic features The pathogenesis of MS is theoretically the same as for AML. In the few cytogenetic studies performed, an increased incidence of MLL rearrangements, monosomy 7, and trisomy 8 have been noted.2,18,31 Mutations of nucleophosmin-1 are also frequent, as they are in AML as a whole.3 A high incidence of t(8;21)(q22;q22) has also been reported, and appears to be associated with pediatric and/or orbital tumors.2,32–35
Cutaneous lesions consist of a moderate to dense dermal infiltrate, displaying a nodular or diffuse growth pattern, and sometimes involving the subcutis. Perivascular or periadnexal accentuation is frequent. The epidermis is typically spared.11,14,21,36,37 The tumor cell cytology is variable and dependent on the direction and degree of differentiation. Most cases comprise medium to large blasts, which often infiltrate in rows between collagen bundles, and frequently display a monoblastic or myelomonocytic
Differential diagnosis The main differential diagnoses include blastic plasmacytoid dendritic cell neoplasm, LLL, large B-cell lymphomas, and small round blue cell tumors of childhood. Immunohistochemistry and clinical information should make the diagnosis relatively easy, although a broad range of antibodies may be required. The greatest overlap is with blastic plasmacytoid dendritic cell neoplasm, and this is most reliably distinguished by demonstrating evidence of plasmacytoid dendritic cell differentiation (e.g., CD123, BDCA-2) and absence of myeloid markers other than CD33 (e.g., myeloperoxidase).
1514 Cutaneous lymphoproliferative diseases and related disorders

Fig. 29.341 Myeloid sarcoma: there are erythematous nodules on the medial aspect of the lower leg of this young child.
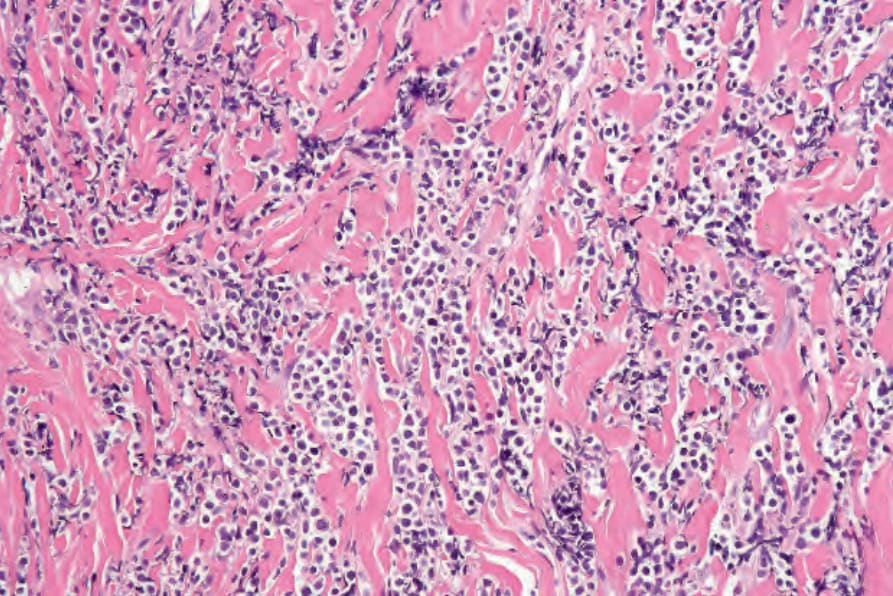
Fig. 29.342 Myeloid sarcoma: there is a heavy dermal infiltrate with prominent dissection of collagen.
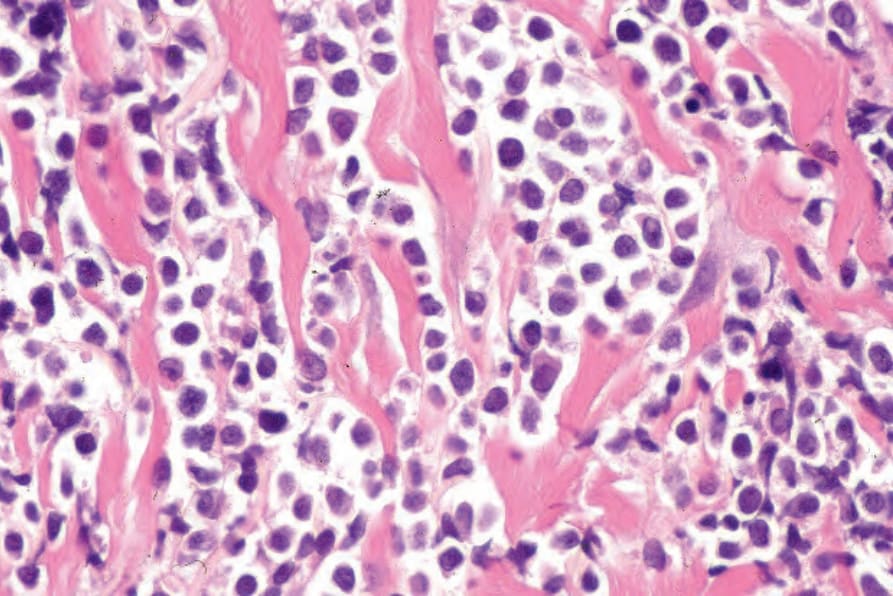
Fig. 29.343 Myeloid sarcoma: the blast cells have darkly staining nuclei and minimal cytoplasm.