Papular xanthoma
Papular xanthoma
Papular xanthoma (PX) is exceptional, presenting most often as disseminated, asymptomatic 2–15 mm diameter, round, yellow to orange discrete papules and nodules with predilection for the head, trunk, and upper limbs, and rarely mucous membranes (Fig. 29.303).61,87–95 The flexures are typically spared.88 Rarely, the distribution is more limited.96 There is a slight female predilection. Only two cases presented with systemic involvement. One of these involved the larynx, and the other involved the conjunctiva, gums, ears, and upper airways.97,98 Lesions were congenital in a single case.99 Most patients are normolipemic, although there is one case associated with primary dysbetalipoproteinemia.89 In adults, the lesions appear to be persistent, whereas in childhood, lesions appear to be self-healing.90 In one case, resolution followed oral doxycycline.98 A variant – so-called progressive PX in which disfiguring chronic lesions may be accompanied by mucosal involvement – has been described and shows considerable overlap with progressive nodular histiocytosis.95
Solitary lesions may be seen mainly on the trunk, followed by the extremities and the head and neck, in children or middle-aged adults, with marked predilection for males (4 : 1).94
including hoarseness, respiratory embarrassment, and problems with closure of the mouth or with defecation.71,73,74 Lower respiratory tract involvement resulting in respiratory failure has also been rarely reported.12,65,68
Systemic disease is frequently encountered, the most common manifestation being diabetes insipidus, which occurs in about 40% of cases and is due involvement of the hypothalamus–pituitary region.74,75 The diabetes insipidus is usually both mild and transient. Meningeal lesions are rare and give rise to epilepsy. Ocular involvement affecting the cornea and conjunctiva occurs in approximately 20% of patients.62 Rarely, bone disease is a feature with progressive and osteolytic lesions.63,71,76,77 Hepatic involvement is very rare.64
A rare association with multiple myeloma and Waldenström macroglobulinemia has been reported.78,79
Progressive nodular histiocytosis and spindle cell xanthogranuloma
Progressive nodular histiocytosis is very rare.100–108 Presentation is usually with small yellowish papules or large nodules measuring up to 5.0 cm in diameter with predilection for the trunk.104 Rarely, a leonine facies is a feature.105,106 Mucosal lesions are exceptional.107 Spontaneous regression is not usual. The sex distribution is equal, with predilection for the fifth and sixth decades.104 Serum lipids are generally normal. Rare associations include hypercholesterolemia, chronic myeloid leukemia, and hypothalamic involvement with precocious puberty and growth failure.106,108
Solitary spindle cell xanthogranuloma predominantly affects younger adults (20–40 years) with equal sex incidence. Anatomic distribution is wide
including the head, neck, upper trunk, and extremities, in decreasing order of frequency. Lesions are slightly elevated to dome-shaped yellow-brown papules or nodules.104
Pathogenesis and histologic features The pathogenesis of this group of disorders is unknown, as is the precise cell of origin. Derivation from a dermal/interstitial dendritic cell is currently favored, in view of the phenotype shared by the dominant histiocytes in all cases, particularly expression of factor XIIIA, fascin, and macrophage markers.20,109–111 Monocytes/macrophages, indeterminate cells, and plasmacytoid monocytes (plasmacytoid dendritic cells) have also been suggested as likely sources of the main cell type.4,11,23,112,113 Although foam cells are a prominent feature, serum lipids are normal. This had led some to propose that lipid accumulates in histiocytes as a result of enhanced uptake and intracellular biosynthesis.114 It has also been suggested that viruses, such as CMV and varicella, or physical factors, may act as triggering stimuli, but this remains speculative.30,115–118 Clonality has been demonstrated in one case.119 BRAF mutations are not typically seen.120
1501 Xanthogranuloma family
The diseases referred to in this section overlap clinically and histologically, suggesting that they represent a continuous spectrum of disease, the manifestations of which are determined by the state of maturation of the constituent cells.110 Thus, disorders of histiocytes at the most immature end of the spectrum tend to arise in early life, run a short clinical course, and undergo spontaneous resolution, i.e., JXG and benign cephalic histiocytosis. Generalized eruptive histiocytosis and XD are proposed to be proliferations of more mature histiocytes, occurring in young adults. Although spontaneous resolution is the norm, the clinical course is longer, from months to many years. Progressive nodular histiocytosis lies at the most mature end of the spectrum. Middle-aged adults and the elderly are most commonly affected; the histiocytes display a fully matured spindled morphology, and the disease is progressive, resistant to treatment, and shows no tendency to spontaneous resolution. This approach is useful, not least in that it acts as a useful aide memoire for the various clinical manifestation of this group of diseases.3,85,110 It has also been proposed that the morphology of the constituent histiocytes within a lesion can be used to predict maturational status, and hence permit pathological discrimination between entities. Vacuolated or lightly eosinophilic histiocytes predominate in immature lesions, scalloped and/or xanthomatized histiocytes in more mature cases, and spindled histiocytes in the most mature. Although there is some evidence to support this, histologic differentiation of entities is often irreproducible in practice.3,85
Lesions in the JXG family are typically well-circumscribed dermal nodules comprising a dense cellular infiltrate. The epidermis is normal, although attenuation over the lesion may be seen (Figs 29.304 and 29.305). Mononuclear and multinucleate histiocytes make up the majority (95%) of cells.85 Mononuclear histiocytes are most frequently small, round, or oval cells with ill-defined lightly eosinophilic, often vacuolated cytoplasm. The nuclei are round to oval with euchromatin and sometimes prominent, albeit small, nucleoli.4,7,103,121–124 Mitotic figures may be seen (Fig. 29.306). Variations on this theme include: larger xanthomatized cells with finely vacuolated, foamy, cytoplasm; ‘scalloped’ histiocytes with angulated, scalloped, or jagged borders; and spindle-shaped histiocytes, sometimes with mildly vacuolated cytoplasm and occasionally showing a storiform pattern.85 The multinucleate cells are typically Touton-type and are present in 85% of lesions but are not a prerequisite for diagnosis. They are very large cells with wreath-like nuclei encircling a central eosinophilic core with a peripheral rim of xanthomatized, foamy cytoplasm (Fig. 29.307). Multinucleate foreign body-like giant cells are rare. Other inflammatory cells are usually present to varying degrees, particularly small lymphocytes, but also eosinophils, neutrophils, and even plasma cells can be present (Fig. 29.308).
Lesions of JXG typically contain histiocytes with a variety of appearances, those with lightly eosinophilic and/or vacuolated cytoplasm predominating (Figs 29.309–29.311). Xanthomatized histiocytes predominate in PX, and scalloped histiocytes in XD and scalloped cell xanthogranuloma. Progressive nodular histiocytosis and spindle cell xanthogranuloma are characterized by a predominance of spindled histiocytes (Figs 29.312 and 29.313). Early lesions are characterized by an abundance of cells with
lightly vacuolated cytoplasm, which become progressively lipidized (xanthomatized) with age. Spindled cells represent the most aged end of this spectrum. Systemic lesions more frequently lack Touton-type giant cells, and spindled cells are often present and may predominate.1,4,21,85,109,113,125
The immunophenotype of the main histiocytic component is the same in all variants of the JXG family. There is positive staining for the macrophage markers CD14, CD68 (both coarse granular cytoplasmic pattern), and CD163 (surface and cytoplasmic) (Fig. 29.314). Dendritic cell markers are also expressed, fascin always, and factor XIIIA frequently. Staining for S100 may be positive in up to 25% of cases. CD1a and langerin are negatvie.113
1502 Cutaneous lymphoproliferative diseases and related disorders
A
Differential diagnosis Although there may be histologic variation between the different members of the JXG family, it is not possible to reliably distinguish them on pathological grounds alone. This is done primarily on the basis of clinical features. All types of xanthogranuloma are distinguished from cutaneous xanthomas by the lack of an inflammatory component and/or multinucleate cells in the latter and normal levels of serum lipids in the former. Langerhans cell histiocytosis is differentiated on immunophenotypic grounds, being uniformly positive for S100 and also expressing CD1a and langerin. RH is usually composed of larger histiocytes with typical eosinophilic ground-glass cytoplasm, and lacks Touton-type giant cells. In Rosai-Dorfman disease, the histiocytes are larger and usually paler staining, show emperipolesis, and are positive for S100. Xanthogranulomas with a prominent spindle cell component may resemble dermatofibroma. However, the distinctive phenotype of xanthogranulomas, and often the clinical features, should allow these two entities to be easily separated.
B

Fig. 29.302 Xanthoma disseminatum: multiple lesions are present on the cheek. By courtesy of the Institute of Dermatology, London, UK.

Fig. 29.303 Papular xanthoma: typical bright yellow papules. By courtesy of the Institute of Dermatology, London, UK.
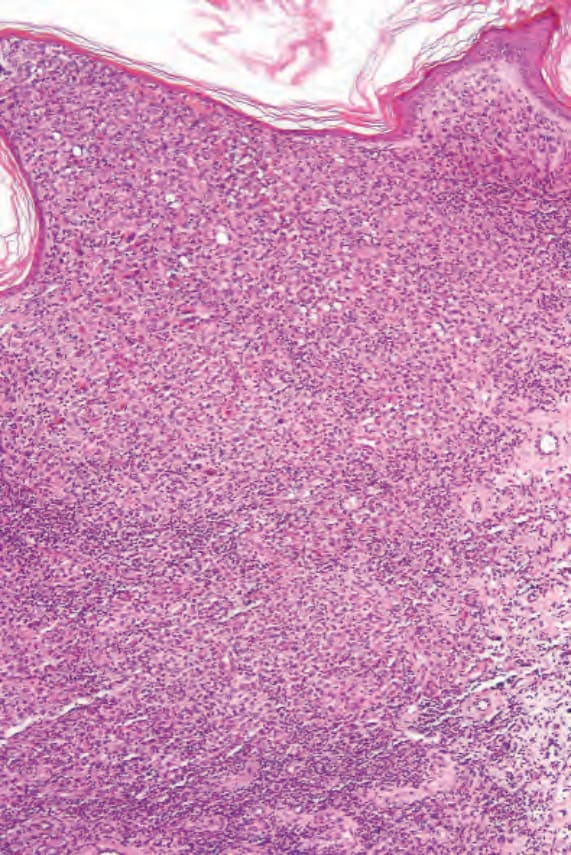
Fig. 29.304 Xanthogranuloma (generalized eruptive histiocytoma): there is a dense infiltrate occupying the papillary and reticular dermis.
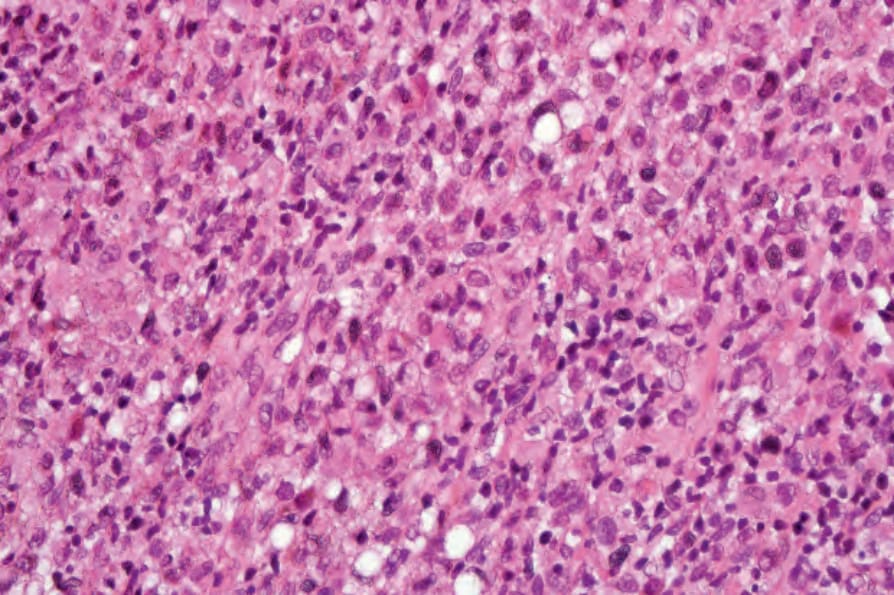
Fig. 29.305 Xanthogranuloma (generalized eruptive histiocytoma): there is a uniform population of nonxanthomatized histiocytes.
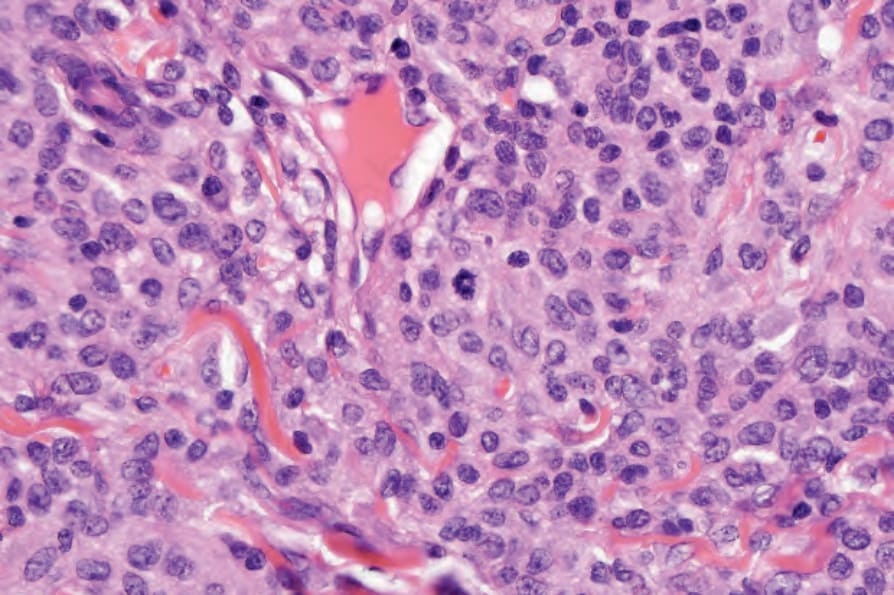
Fig. 29.306 Xanthogranuloma: note the mitotic figure.
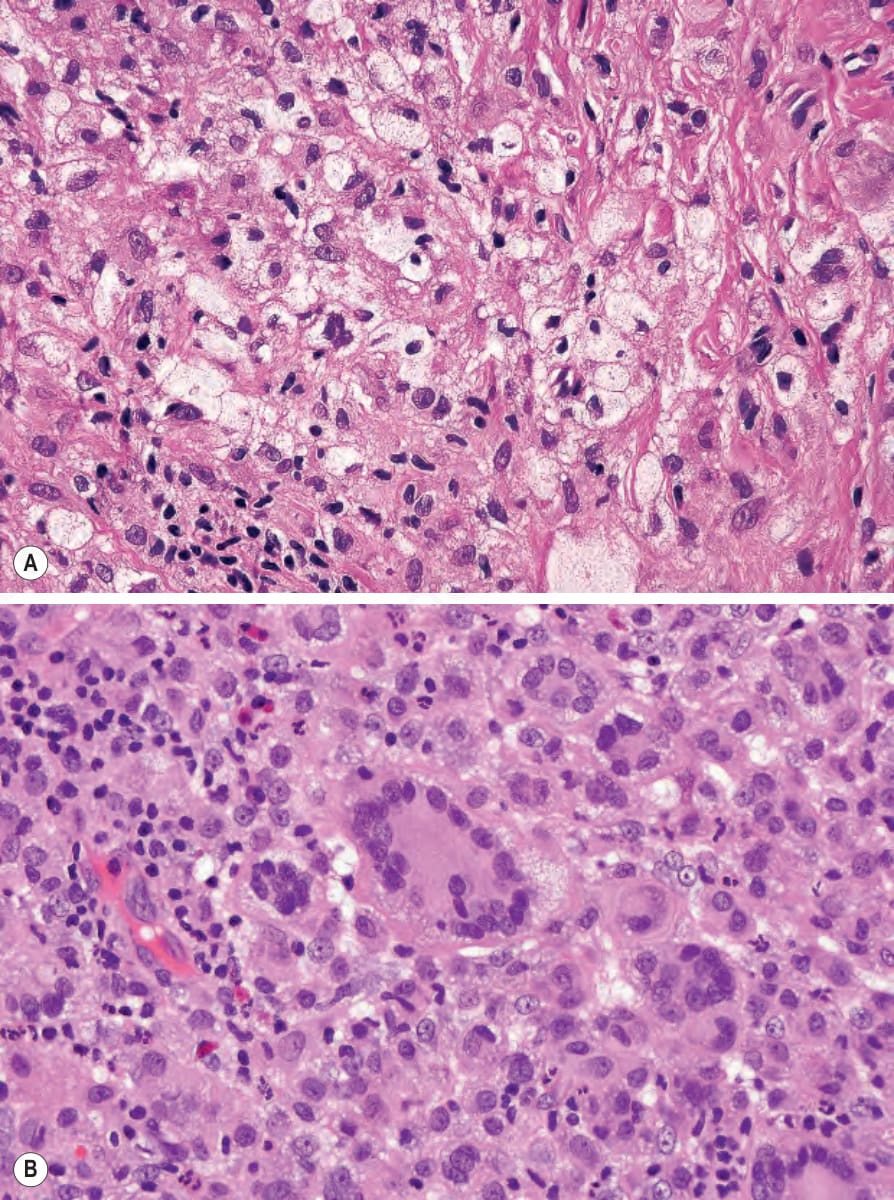
Fig. 29.307 (A, B) Xanthogranuloma: (A) high-power view showing xanthomatized cells; (B) high-power view of a typical Touton giant cell.
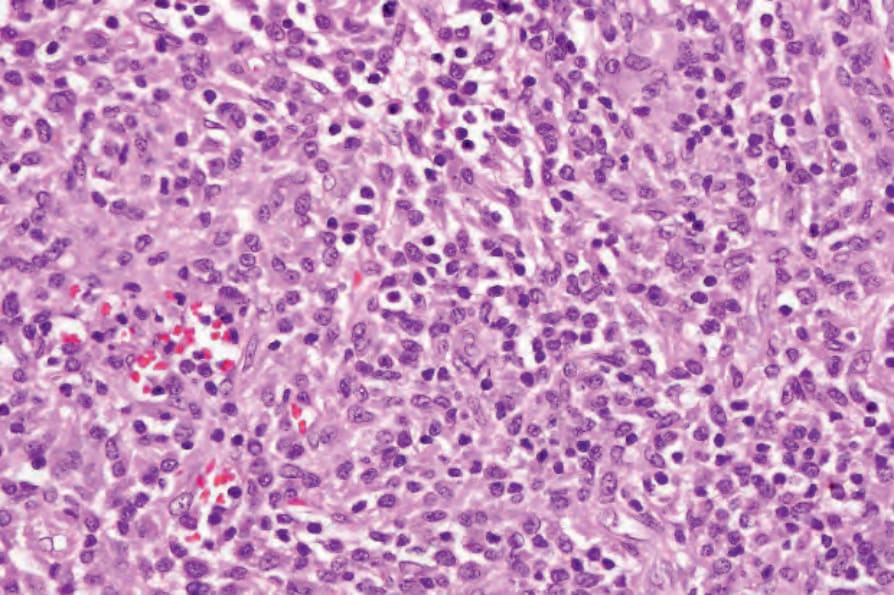
Fig. 29.308 Xanthogranuloma: note the background population of lymphocytes.
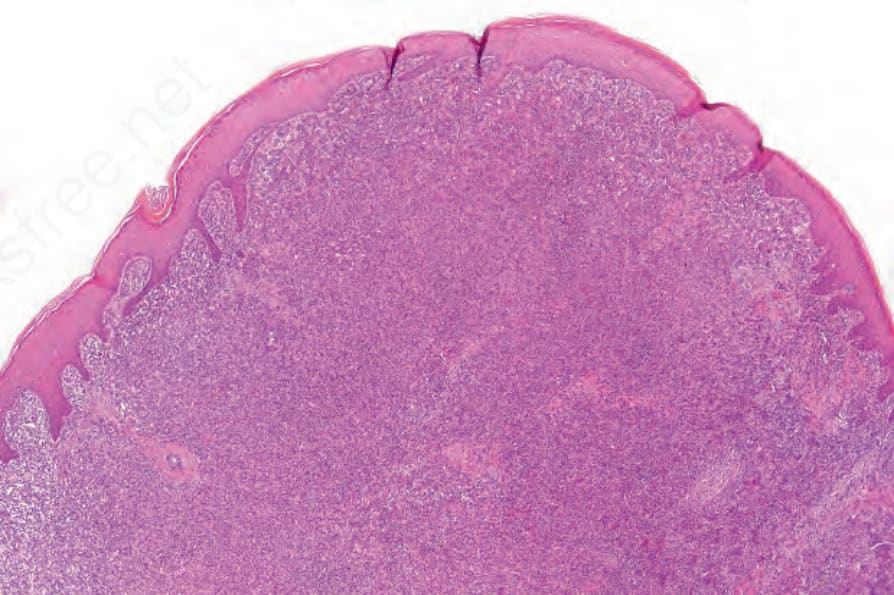
Fig. 29.309 Xanthogranuloma: the dermis is expanded by a dense cellular infiltrate.
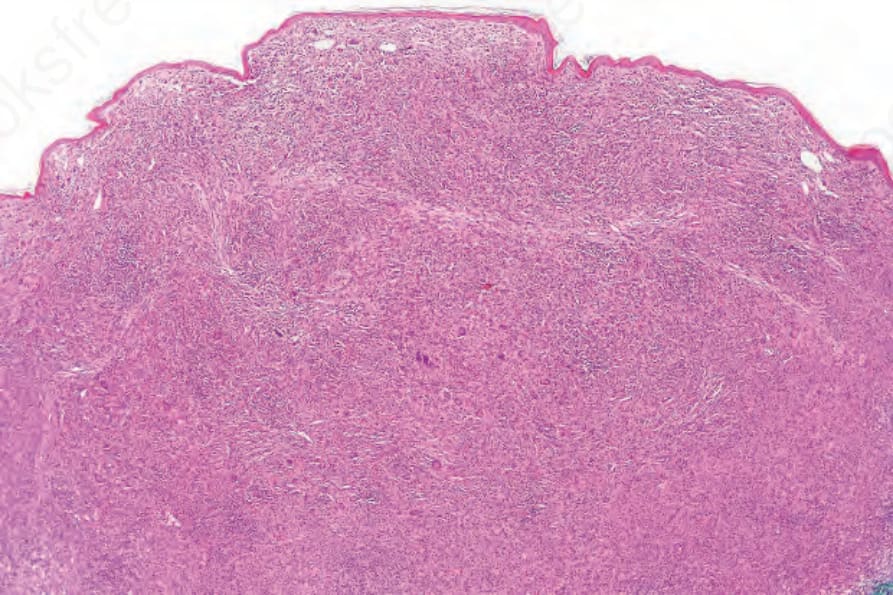
Fig. 29.312 Xanthogranuloma: scanning view of a dermal nodule.
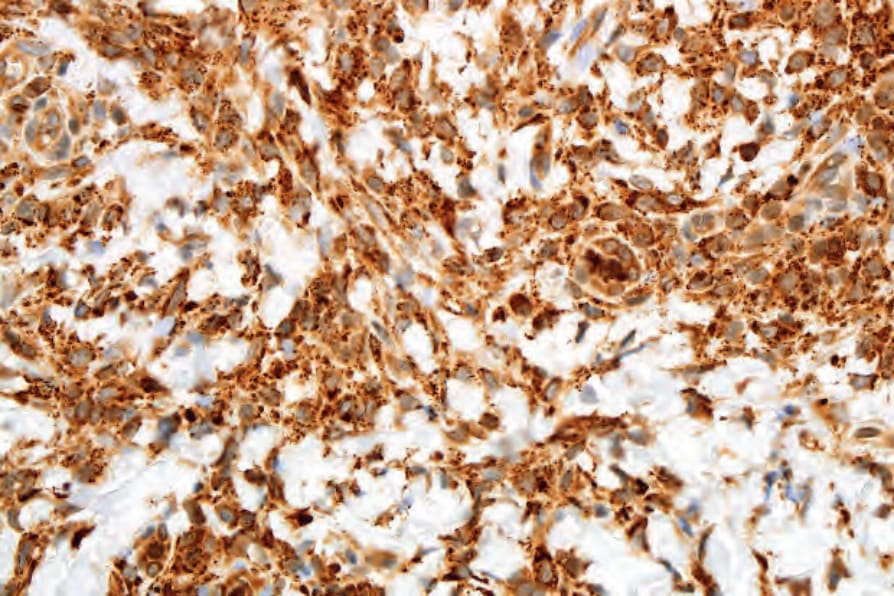
Fig. 29.314 Xanthogranuloma: the histiocytes show strong expression of CD68.