Juvenile xanthogranuloma
Juvenile xanthogranuloma
Juvenile xanthogranuloma (JXG) (xanthogranuloma, nevoxanthoendothelioma, xanthoma multiplex) arises in the first 5 years of life, usually in the first year, and may be present at birth.1–4 However, up to 20% of cases develop in adolescents and young adults, and it also occurs in adults and elderly patients.4–10 Sex incidence is equal, and most patients are Caucasian.4,11,12
JXG is usually limited to the skin, but may arise at extracutaneous sites, with or without concomitant cutaneous lesions. Approximately two-thirds
1498 Cutaneous lymphoproliferative diseases and related disorders
the upper trunk and proximal limbs, predominantly in girls (5 : 1).11,13–16 Congenital presentation is common and ulceration is often seen.11 The agminate variant is exceptional, presenting as clustered papules, and may be associated with alopecia.17,18 In contrast to the more usual sites, the arm and leg have been affected. One case of lichenoid JXG has been described.19
Extracutaneous involvement is seen in up to 25% of cases and may take the form of a solitary lesion without associated skin disease.4,20 Solitary extracutaneous lesions usually present as a large subcutaneous (up to 3 cm in diameter) or soft tissue (usually >4 cm diameter) mass. The soft tissues of the head and neck are most frequently involved, and rarely lesions occur on the trunk and limbs, and in the abdomen–pelvis.4,21–24 The orbit is another common site.2,3,25,26 Patients with ocular involvement are under 2 years of age, and most present with a unilateral asymptomatic iris tumor, a red eye with signs of uveitis, unilateral glaucoma, and spontaneous hyphema.12,25,26 Solitary lesions can also occur in bone, tongue, nasal cavity and paranasal sinuses, and lung.4
Visceral disease is usually multifocal and associated with multiple skin lesions.4 Organs involved include liver, spleen, lungs, and CNS, and less commonly in the heart, oropharynx, muscle, kidney, bone, pancreas, peripheral nerve, ovaries, testes, and adrenal gland.
Skin lesions tend to flatten, disappearing over months to years, sometimes leaving atrophic or hypopigmented scars. Most systemic lesions also completely regress within 3 to 6 years.1–3 Rare fatalities have occurred in patients with CNS or hepatic involvement.4,27–29 There is a well-documented association between JXG and neurofibromatosis type I and/or juvenile myelomonocytic leukemia (Fig. 29.296).9,30–32 In cases associated with leukemia, JXG usually precedes or presents concurrently.
of cases present as a solitary cutaneous nodule, typically in the head and neck region, followed by the trunk or upper limbs (Fig. 29.294).4,11,12 Multiple skin lesions are much less common (approximately 7% of cases) (Fig. 29.295).4 Patients are usually young children (median age, 5 months) with head and neck involvement. In one series, nearly all cases were male.4 Cutaneous lesions are usually described as yellowish, orange, red-brown, or flesh-colored papules or nodules and rarely plaques measuring a few millimeters to several centimeters in diameter. The appearances may mimic a Spitz nevus or mastocytoma.11 Lesions are usually asymptomatic, although pruritus may be a feature and rarely they are painful.12
Rare presentations include giant, clustered (agminate), and lichenoid forms.11 Giant lesions are >2.0 cm in diameter, and most commonly affect
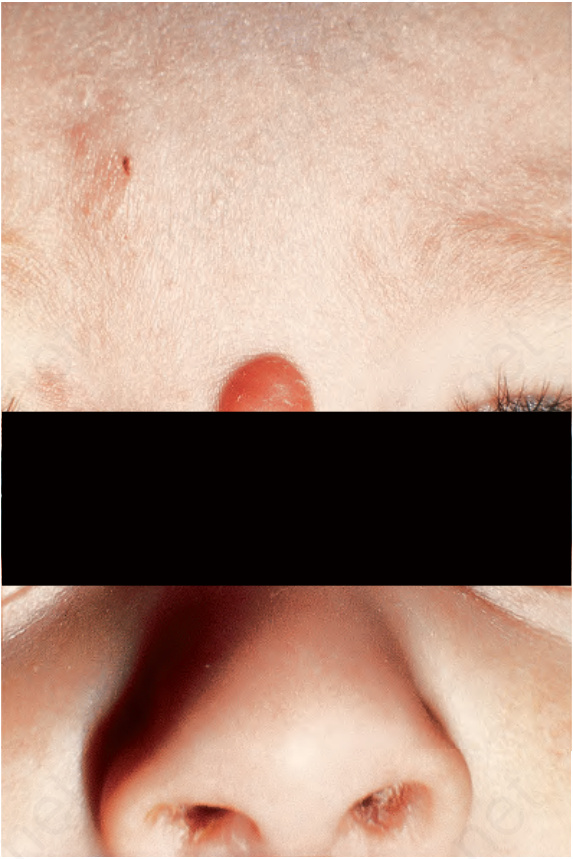
Fig. 29.294 Xanthogranuloma: there is a characteristic reddish-brown nodule on the bridge of the nose of this infant. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 29.295 Xanthogranuloma: this child has multiple lesions. By courtesy of the Institute of Dermatology, London, UK.

Fig. 29.296 Xanthogranuloma: this is a rare example of xanthogranulomata presenting in a child with neurofibromatosis type I. By courtesy of the Institute of Dermatology, London, UK.