Cutaneous Kikuchi-Fujimoto disease
Cutaneous Kikuchi-Fujimoto disease
Clinical features Kikuchi-Fujimoto disease (KFD) (Kikuchi-Fujimoto disease, histiocytic necrotizing lymphadenitis) is a relatively rare self-limited reactive disorder that characteristically presents with cervical lymphadenopathy, systemic symptoms including fever, weight loss, and sweating, and tends to be more common in young females, particularly in the Far East. Children may also be affected. Cutaneous involvement in KFD has been described in up to 40% of patients.1–14 Specific cutaneous lesions of KFD include macules and papules and more rarely nodules, plaques, pustules, or ulcerated lesions. Subcutaneous lesions are rare.14 They can occur anywhere in the body with predilection for the face, trunk, and upper limbs. Non-specific cutaneous associations of the disease include leukocytoclastic vasculitis and erythema multiforme.15–17 An association with lupus erythematosus has also been described.18–21 However, the histologic features of the lymphadenitis seen in lupus erythematosus are identical to those seen in KFD, and therefore it is likely that the patients reported in the literature had lupus erythematosus from the outset. In a single case, cutaneous disease has been associated with Sjögren syndrome.22
Pathogenesis and histologic features The pathogenesis of IH is unknown, and the disorder may represent a non-specific reaction pattern associated with various inflammatory conditions. Focal changes identical to those seen in IH can be identified in a number of inflammatory processes and even in association with tumors. Chronic inflammation associated with lymphedema and lymphangiectasia may be the trigger for the intravascular proliferation of histiocytes.6 Histologically, dilated, irregular thin-walled vascular channels are seen in the reticular dermis and many contain aggregates of cells with a histiocytic appearance including pale cytoplasm and vesicular, reniform nuclei with an inconspicuous nucleolus (Fig. 29.268). These cells are positive for histiocytic markers including CD68 and can occasionally be positive for myeloperoxidase.6 Cytological atypia is not a feature, and there are no mitotic figures. The histiocytes can be associated with lymphocytes and neutrophils, and a perivascular infiltrate composed of lymphocytes and plasma cells is often present. Endothelial cells may be slightly prominent and occasionally display focal proliferation. The lymphatic nature of the vascular channels is confirmed by positivity of the endothelial cells for podoplanin, LYVE-1, and Prox-1.2,6
Pathogenesis and histologic features Although a possible relationship with a viral infection including EBV has been suggested, this has not been proven in most cases.23 Histologic criteria for the diagnosis of KFD have recently been proposed based on a series of cases. The most consistent findings include hydropic degeneration of basal cells, necrotic keratinocytes, and a superficial and deep perivascular and focally interstitial infiltrate composed of lymphocytes and histiocytes with variable amounts of nuclear debris in the absence of neutrophils. A proportion of the histiocytic cells are plasmacytoid monocytes. Some histiocytes have a crescentic nucleus that is pressed against the cytoplasmic membrane.14 Involvement of the subcutis is seen in up to 60% of cases.14 Epidermal changes include acanthosis, hyperkeratosis, and parakeratosis, and there is often papillary dermal edema. Other inflammatory cells including plasma cells and eosinophils are rare. Interstitial mucin is sometimes identified. The histiocytes are positive for CD68 and CD163 and may be positive for myeloperoxidase.24 The plasmacytoid monocytes are positive for CD123. The lymphocytes are T cells, and there seems to be a more prominent number of CD8-positive cells.
Differential diagnosis The differential diagnosis includes reactive angioendotheliomatosis and intravascular lymphoma. It has been suggested that reactive angioendotheliomatosis and IH are part of the same spectrum, but this is unlikely.12,13 The former is a proliferation of endothelial cells that fill pre-existing blood vessels and frequently result in formation of new vascular channels. The proliferation involves blood vessels and not lymphatics as in IH. In intravascular lymphoma, an aggressive disease usually presenting with systemic dissemination, atypical and mitotically active lymphoid cells mostly with a B-cell phenotype fill dilated vascular channels. Morphology and immunohistochemistry should allow easy distinction between the two entities.
A further differential diagnosis is a recently described entity under the name intravascular histiocytosis with hemophagocytosis. Only three cases
1490 Cutaneous lymphoproliferative diseases and related disorders
have been reported, and presentation is with a reticulated symmetrical erythema with predilection for the skin of the breasts.14 The channels involved appear to be blood vessels, not lymphatics, and distinctively there is intravascular hemophagocytosis.
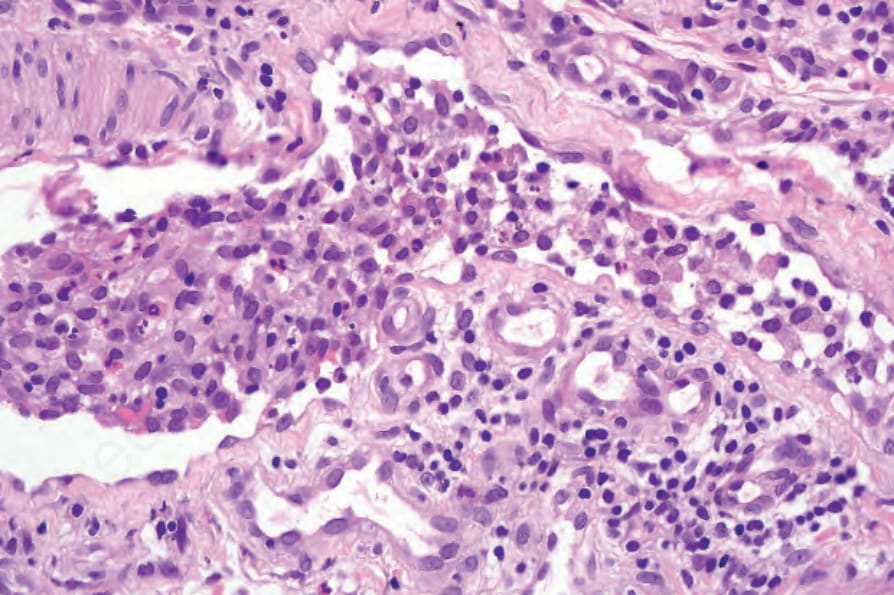
Fig. 29.268 Intralymphatic histiocytosis: innumerable histiocytes are present within the lumen of this dermal vessel.

Fig. 29.269 Unifocal LCH (eosinophilic granuloma): this example is a raised erythematous plaque. By courtesy of the Institute of Dermatology, London, UK.